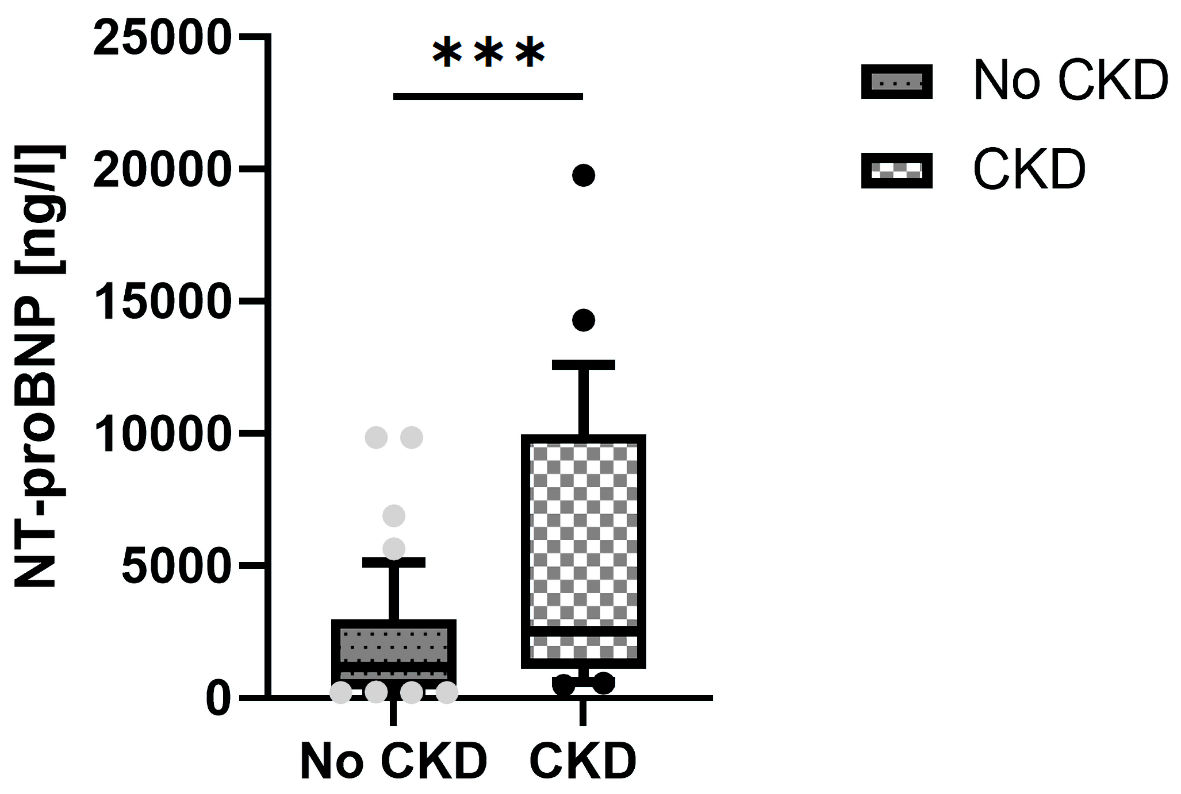
Figure 1. NT-proBNP levels in patients with and without CKD. NT-proBNP: N-terminal pro-brain natriuretic peptide; CKD: chronic kidney disease.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 13, Number 2, April 2022, pages 73-80
The Association of N-Terminal Pro-Brain Natriuretic Peptide With Time to Clinical Worsening in Hispanic Patients With Pulmonary Arterial Hypertension
Figures
Tables
| All patients (n = 115) | No clinical worsening (n = 89) | Clinical worsening (n = 26) | P value | |
|---|---|---|---|---|
| BMI: body mass index; WHO-FC: World Health Organization-Functional Classification; mRAP: mean right atrial pressure; mPAP: mean pulmonary arterial pressure; PCWP: pulmonary capillary wedge pressure; CO: cardiac output; 6MWD: 6-min walk distance; NT-proBNP: N-terminal pro-brain natriuretic peptide; SCr: serum creatinine. | ||||
| Age (years) | 52 (46 - 68) | 50 (44 - 69) | 61 (48 - 69) | 0.14 |
| Female (%) | 67 | 72 | 58 | 0.53 |
| BMI (kg/m2) | ||||
| WHO-FC (I - IV) | 2.5 ± 0.8 | 2.0 ± 0.5 | 2.9 ± 0.6 | < 0.05 |
| mRAP (mm Hg) | 9 (6 - 14) | 8 (6 - 13) | 11.5 (8 - 18) | < 0.05 |
| mPAP (mm Hg) | 40 (29 - 51) | 37 (27 - 50) | 43 (35 - 51) | 0.13 |
| PCWP (mm Hg) | 11 (7 - 14) | 11 (6 - 12) | 11.5 (9 - 14) | 0.66 |
| CO (L/min) | 5.4 (4.2 - 6.7) | 5.4 (3.8 - 5.3) | 5.0 (3.2 - 5.2) | 0.78 |
| 6MWD (m) | 389 (282 - 450) | 396 (297 - 453) | 288 (187 - 364) | < 0.05 |
| NT-proBNP (ng/L) | 486 (135 - 2,540) | 242 (118 - 1,210) | 3,585 (1,840 - 6,893) | < 0.05 |
| SCr (mg/dL) | 1.04 (0.6 - 1.2) | 0.8 (0.6 - 1.1) | 1.1 (0.6 - 1.4) | 0.81 |
| No CKD (n = 88) | CKD (n = 27) | |
|---|---|---|
| CKD: chronic kidney disease; PDE5-i: phosphodiesterase type 5 inhibitors; ERAs: endothelin receptor antagonists. | ||
| PDE5-i | 88 (100%) | 27 (100%) |
| ERAs | 65 (74%) | 21 (77%) |
| Prostacyclin | 17(19%) | 4 (14%) |
| Mono-therapy | 23 (26%) | 6 (23%) |
| Double combination therapy | 48 (55%) | 17 (63%) |
| Triple combination therapy | 17 (19%) | 4 (14%) |
| Variables | All patients (n = 115) | No CKD (n = 88) | CKD (n = 27) | P value |
|---|---|---|---|---|
| CKD: chronic kidney disease; BMI: body mass index; WHO-FC: World Health Organization-Functional Classification; mRAP: mean right atrial pressure; mPAP: mean pulmonary arterial pressure; PCWP: pulmonary capillary wedge pressure; CO: cardiac output; 6MWD: 6-min walk distance; NT-proBNP: N-terminal pro-brain natriuretic peptide; SCr: serum creatinine. | ||||
| Age (years) | 52 (46 - 68) | 53 (44 - 69) | 56 (48 - 61) | 0.28 |
| Female (%) | 67 | 76 | 51 | 0.31 |
| BMI (kg/m2) | ||||
| WHO-FC (I - IV) | 2.5 ± 0.8 | 2.0 ± 0.6 | 3.0 ± 0.7 | < 0.05 |
| mRAP (mm Hg) | 9 (6 - 14) | 8 (5 - 14) | 10 (8 - 16) | 0.60 |
| mPAP (mm Hg) | 40 (29 - 51) | 38 (29 - 50) | 39 (32 - 52) | 0.88 |
| PCWP (mm Hg) | 11 (7 - 14) | 10 (4 - 7) | 13 (10 - 14) | 0.62 |
| CO (L/min) | 5.4 (4.2 - 6.7) | 5.3 (4 - 7) | 4.6 (3.9 - 5.8) | 0.74 |
| 6MWD (m) | 389 (282 - 450) | 389 (306 - 503) | 326 (300 - 399) | 0.21 |
| NT-proBNP (ng/L) | 486 (135 - 2,540) | 381 (122 - 1,940) | 1,188 (235 - 3,240) | < 0.05 |
| SCr (mg/dL) | 1.04 (0.6 - 1.2) | 0.7 (0.6 - 0.8) | 1.3 (1.1 - 2.1) | < 0.05 |