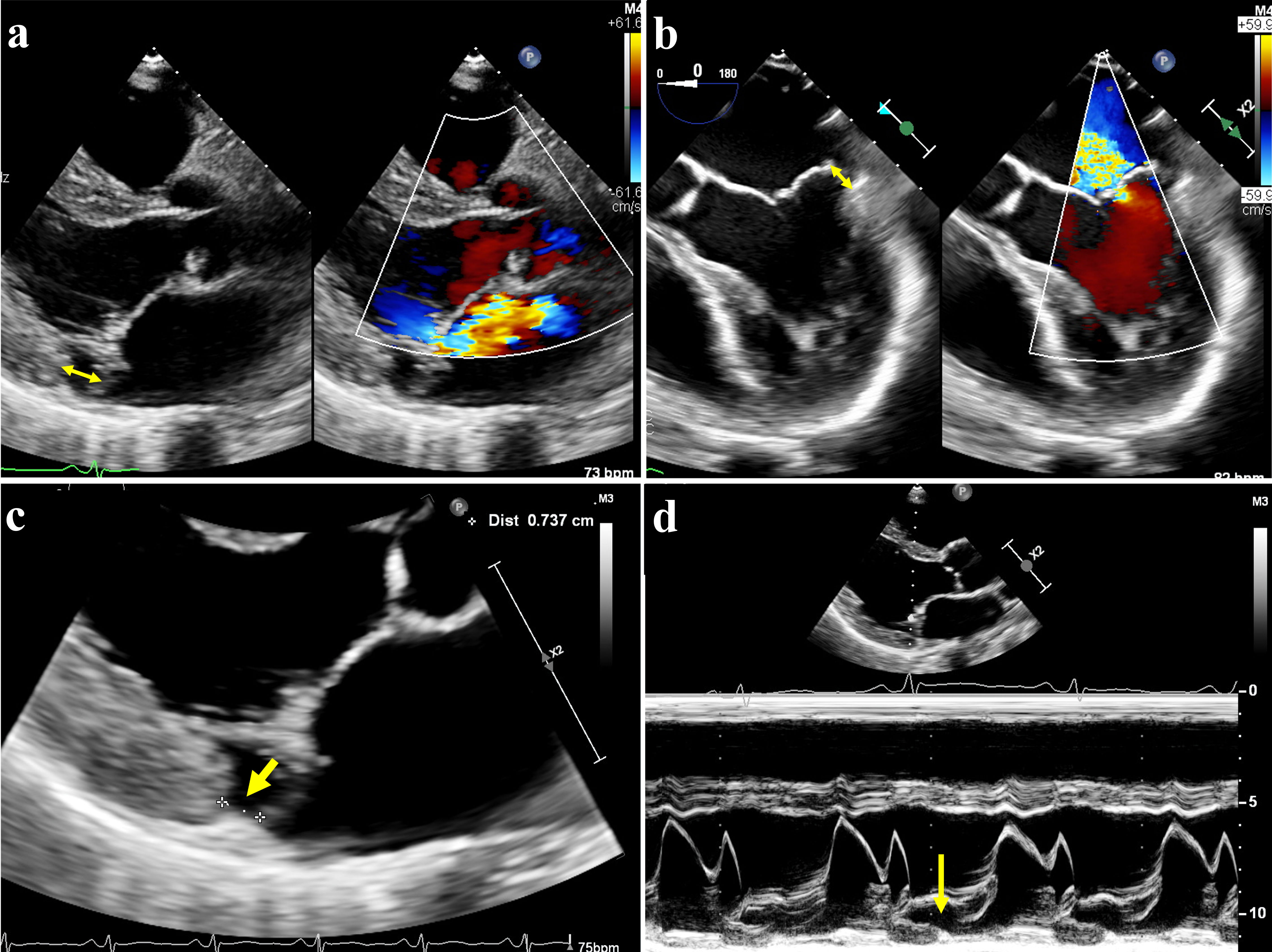
Figure 1. Mitral annular disjunction (MAD) on echocardiography. (a) Transthoracic echography (TTE) showed posterior leaflet prolapse with eccentric mitral regurgitation, with MAD seen (double-arrow). (b) Transesophageal echocardiography (TEE) of same patient also demonstrated MAD in systole (double-arrow). (c) MAD was demonstrated on parasternal long axis view on TTE, with the distance between mitral valve leaflet-atrial wall and left ventricle measured at 7 mm (arrow). (d) The hypermobile posterior annulus could be appreciated on the M-mode of TTE (arrow).
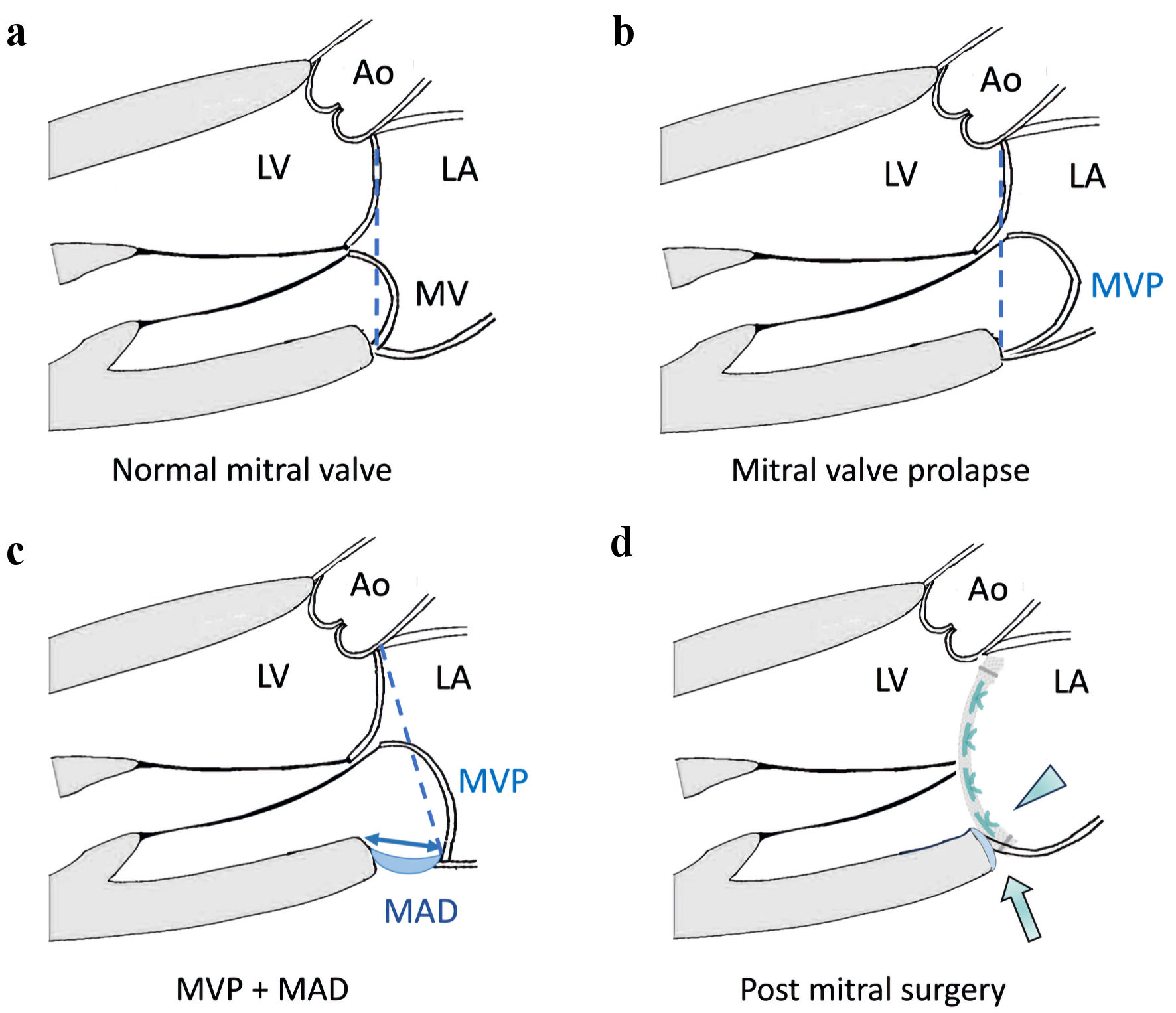
Figure 2. Illustrations of mitral annular disjunction (MAD) and surgical principles for mitral valve surgery. (a) Normal mitral valve: mitral annular plane is in its normal position (dashed line). (b) Mitral valve prolapse (MVP) without MAD: mitral annulus plane (dashed line) remains in its normal position despite prolapse of the mitral leaflet. (c) MVP with MAD: the mitral annulus is “dislocated” away from the normal left ventricle-left atrial (LV-LA) myocardium junction resulting in MAD (double-arrow), and the mitral annular plane (dashed line) has shifted towards LA. (d) MAD can be treated by mitral valve surgery, by suturing the prosthetic ring or valve (arrowhead) to the correct level of the LV-LA myocardial junction. The mitral annulus is stabilized, and the MAD can be obliterated after mitral surgery (arrow). Ao: aorta; LV: left ventricle; LA: left atrium; MV: mitral valve; MVP: mitral valve prolapse; MAD: mitral annular disjunction.