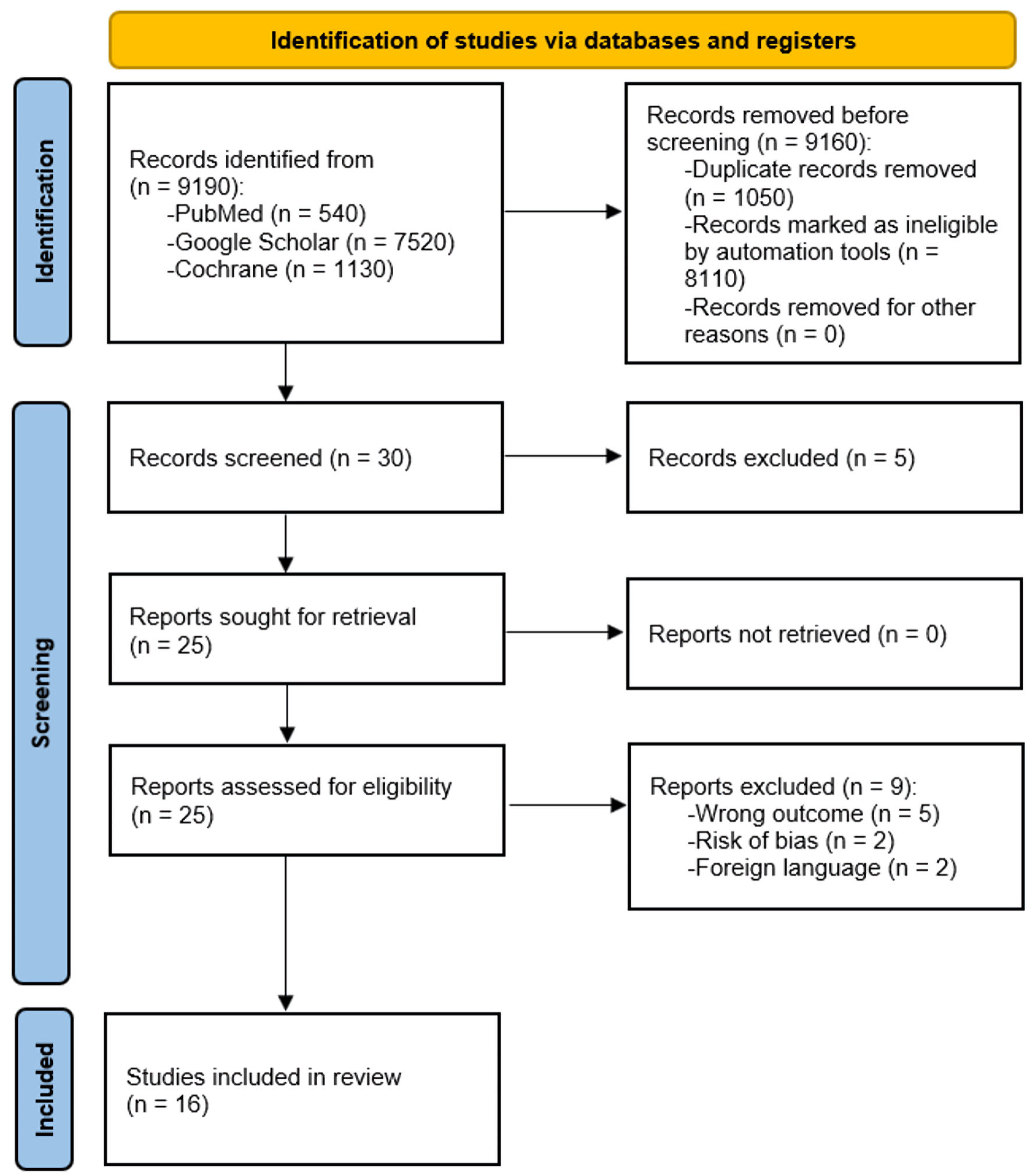
Figure 1. PRISMA flowchart illustrating the study selection process. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 15, Number 4, August 2024, pages 281-297
Efficacy of Beta-Blockers and Angiotensin-Converting Enzyme Inhibitors in Non-Ischemic Dilated Cardiomyopathy: A Systematic Review and Meta-Analysis
Figures

Tables
| No. | Questions | Seghatol et al, 2004 [20] | Yamada et al, 1993 [23] | Ng et al, 2007 [24] | Parent et al, 2016 [25] |
|---|---|---|---|---|---|
| Y: yes; N: no; ?: cannot answer; CASP: Critical Appraisal Skills Programmer; CI: confidence interval; LVEF: left ventricular ejection fraction; SMD: standardized mean difference; ED: effect difference. | |||||
| 1 | Did the study address a clearly defined problem? | Y | Y | Y | Y |
| 2 | Did the authors approach their research question appropriately? | Y | Y | Y | Y |
| 3 | Were cases recruited appropriately? | Y | Y | Y | Y |
| 4 | Were controls selected in a way that made logical sense? | Y | Y | ? | Y |
| 5 | Was bias minimized by accurate measurement of exposure? | Y | N | Y | Y |
| 6a | Did the groups receive the same treatment except for the experimental intervention? | Y | Y | Y | Y |
| 6b | Did the authors account for potential confounding variables in their analysis or design? | ? | Y | Y | Y |
| 7 | What was the effect of the treatment? | Increase in LVEF with SMD 40±9%; 95% CI: 31 - 49; P < 0.05 | SMD 14.2±9.7%; 95% CI: 4.5 - 23.9; P < 0.05 | 2.9-fold relative risk; 95% CI: 1.34 - 6.42, P < 0.01 | LVEF: SMD 16±12%; 95% CI: 4 - 28; P < 0.0001, ED z-score: SMD 0.83±1.93%; 95% CI: -1.1 - 2.76; P < 0.05 |
| 8 | How accurate was the treatment effect estimate? | Statistically significant association with P < 0.05 | Statistically significant association with P < 0.001 (sensitivity of 72%, specificity of 91%, and predictive accuracy of 80%) | Significant association with P < 0.01 | SMD 14.2±9.7%; 95% CI: 4.5 - 23.9; P < 0.05 |
| 9 | Are the results credible? | Y | Y | ? | Y |
| 10 | Can the local community use the results? | N | N | N | N |
| 11 | Are the results of this research consistent with other data that may be available? | Y | ? | ? | Y |
| Score out of a possible 11 | 10 | 9 | 8 | 10 | |
| Study, year | Drug used | Participants | Study model | Intervention | Impact on EF | Adverse events | Deaths | Result |
|---|---|---|---|---|---|---|---|---|
| EF: ejection fraction; CR: contractile reserve; IDC: ischemic dilated cardiomyopathy; LV: left ventricular; LVEF: left ventricular ejection fraction; DCM: dilated cardiomyopathy; ICM: ischemic cardiomyopathy; NICM: non-ischemic cardiomyopathy; ACE: angiotensin-converting enzyme; MI: myocardial infarction; HF: heart failure; AV: atrioventricular; CHF: congestive heart failure; QoL: quality of life; NIDCM: Non-ischemic dilated cardiomyopathy. | ||||||||
| Waagstein et al, 1993 [19] | Metoprolol | 383 | Randomized, placebo-controlled, parallel-group | The primary objective was to study the effect of metoprolol on a combined fatal and non-fatal endpoint | Significant improvement in EF in the metoprolol group | 19 in the placebo group, two in the metoprolol group | 38 in the placebo group, 25 in the metoprolol group | Metoprolol both improves hemodynamic stability and decreases chances of adverse events |
| Seghatol et al, 2004 [20] | Carvedilol, metoprolol, atenolol | 14 | Prospective cohort | The objective of the study was to assess contractile reserve and EF improvement | Significant improvement in both CR and EF in IDC patients | Reactive airway diseases, sexual dysfunction with carvedilol | 3 (not included in final analysis as unrelated) | Beta-blockers have significant impact on improving EF in both short and long term |
| Patrianakos et al, 2005 [21] | Nebivolol | 60 | Randomized, placebo-controlled, parallel-group | Assessment of nebivolol in improving LV function in non-ischemic dilated cardiomyopathy | Improvement in EF in nebivolol group along with improved systolic and diastolic LV function | Well tolerated; however, exercise duration decreased | None | Third-generation beta-blockers are both well tolerated and improve LVEF |
| Lowes et al, 2002 [22] | Metoprolol, carvedilol | 49 | Randomized, placebo-controlled, parallel-group | To test the hypothesis of whether beta-blockers improve EF by altering myocardial contractility genes | Improvement in LVEF with other hemodynamic stabilizations | None reported | None | 26 out of 30 patients in the beta-blocker group had improved EF |
| Yamada et al, 1993 [23] | Metoprolol | 30 | Retrospective cohort | To test beta-blocker long-term effect in DCM and observe histological differences | Long-term increase in LVEF | Not discussed | None | Beta-blockers are helpful in improving LVEF in patients with lesser fibrosis in the myocardium in the setting of DCM |
| Ng et al, 2007 [24] | Beta-blocker | 78 | Cohort | To evaluate difference in outcomes for ICM and NICM | Short- and long-term increase in LVEF | Insignificant incidences of peripheral vascular diseases and hyperlipidemia, and significant reports of atrial fibrillations | 17% mortality rate in 40 months in ICM and NICM groups combined | Beta-blockers and ACE inhibitors decrease risk of mortality and increase LVEF in long-term management plans |
| Hall et al, 1995 [26] | Metoprolol | 16 | Randomized, placebo-controlled, parallel-group | To assess improvement in LV function, mass, and geometry in patients with either ICM or NIDCM | Improvement in LVEF, LV mass reduction, and regression to normal elliptical shape of LV after 18 months | Not mentioned | None | Beta-blockers have been shown to improve various dynamics of LV function and mass as well |
| Parent et al, 2016 [25] | Metoprolol, ACE inhibitors | 51 | Retrospective cohort | To assess whether beta-blockers and ACE inhibitors are useful in cardiac remodeling in left ventricle non-compaction cardiomyopathy with DCM | LVEF and LV dimensions showed improvement by 16% | None | None | Beta-blockers and ACE inhibitors both showed promising results in terms of LVEF improvement and cardiac remodeling of the heart in dilated heart disease |
| Olsen et al, 1995 [27] | Carvedilol | 60 | Randomized, placebo-controlled, parallel-group | To assess LVEF impact and symptoms through carvedilol | Reduction in heart rate, and LVEF had increased | 1 patient suffered from worsened heart symptoms, 1 had embolic cerebrovascular, 1 had non-Q wave MI | 3 deaths during the trial but deemed unrelated to medicinal intervention | Reduction in LVEF and other hemodynamic factors was shown due to carvedilol intervention |
| Gilbert et al, 1990 [28] | Bucindolol | 24 | Randomized, placebo-controlled, parallel-group | To assess long-term effects of bucindolol in patients developing heart failure in the setting of NIDCM | Improvement in LVEF and hemodynamic stability was seen in 22 patients | 1 patient underwent transplant within 3 weeks of the trial, and 1 patient suffered from a pulmonary embolus and also had to undergo cardiac transplant at the 6th-week mark | 1 death occurred before the trial’s advent | Bucindolol was well tolerated by patients and favored the hemodynamic state towards stability in heart failure |
| Metra et al, 1994 [29] | Carvedilol | 40 | Randomized, placebo-controlled, parallel-group | To check carvedilol efficacy as a drug for NIDCM | Reduction in heart rate was observed along with improvement in the heart’s working capacity with reported lessening of HF symptoms. LVEF was improved. | 1 patient reported worsening of dyspnea | None | Carvedilol showed promising prospects in both managing NIDCM and improving the QoL of patients |
| Di Lenarda et al, 1999 [30] | Carvedilol | 30 | Randomized, placebo-controlled, parallel-group | To assess carvedilol’s efficacy in patients showing no response to metoprolol therapy | Marked improvement in both LVEF and decrease in LV dimensions were observed. | 4 patients showed signs of nocturnal AV conduction, and 1 patient suffered from symptomatic paroxysmal atrial fibrillation | None | Carvedilol has promising benefits for patients on chronic therapy of metoprolol through cardiac remodeling and improvement in LVEF |
| Sanderson et al, 1999 [31] | Carvedilol, metoprolol | 23 | Randomized, placebo-controlled, parallel-group | To compare the efficacy of carvedilol and metoprolol in CHF in the setting of idiopathic dilated cardiomyopathy | Both drugs have shown significant improvement in LVEF. | None | None | Both drugs have been shown to have efficacy for improving hemodynamic criteria and QoL |
| Quaife et al, 1996 [32] | Carvedilol | 36 | Randomized, placebo-controlled, parallel-group | To study carvedilol’s efficacy in idiopathic DCM through systolic and diastolic LV function | Significant improvement in LVEF | Not discussed | None | In moderate chronic heart failure, systolic LV performance improves, but diastolic LV function does not improve when compared with placebo after treatment with carvedilol |
| Franciosa et al, 1985 [33] | Enalapril | 13 | Randomized, placebo-controlled, parallel-group | To study the effect of enalapril’s role in improving symptoms of heart failure | Significant improvement in LVEF seen in the group receiving enalapril | No adverse events in the enalapril group | None | Enalapril showed improvement in hemodynamics, LVEF and exercise tolerance tests |
| Sharpe et al, 1984 [34] | Enalapril | 28 | Randomized, placebo-controlled, parallel-group | To study the long-term effects of enalapril in chronic heart failure | LVEF and LV diameters showed improvement in their parameters | No significant adverse events | 5 deaths (1 in enalapril group and deemed unrelated to the drug) | Enalapril improves the lifestyle of long-term cardiac patients, along with stabilizing hemodynamic properties significantly |