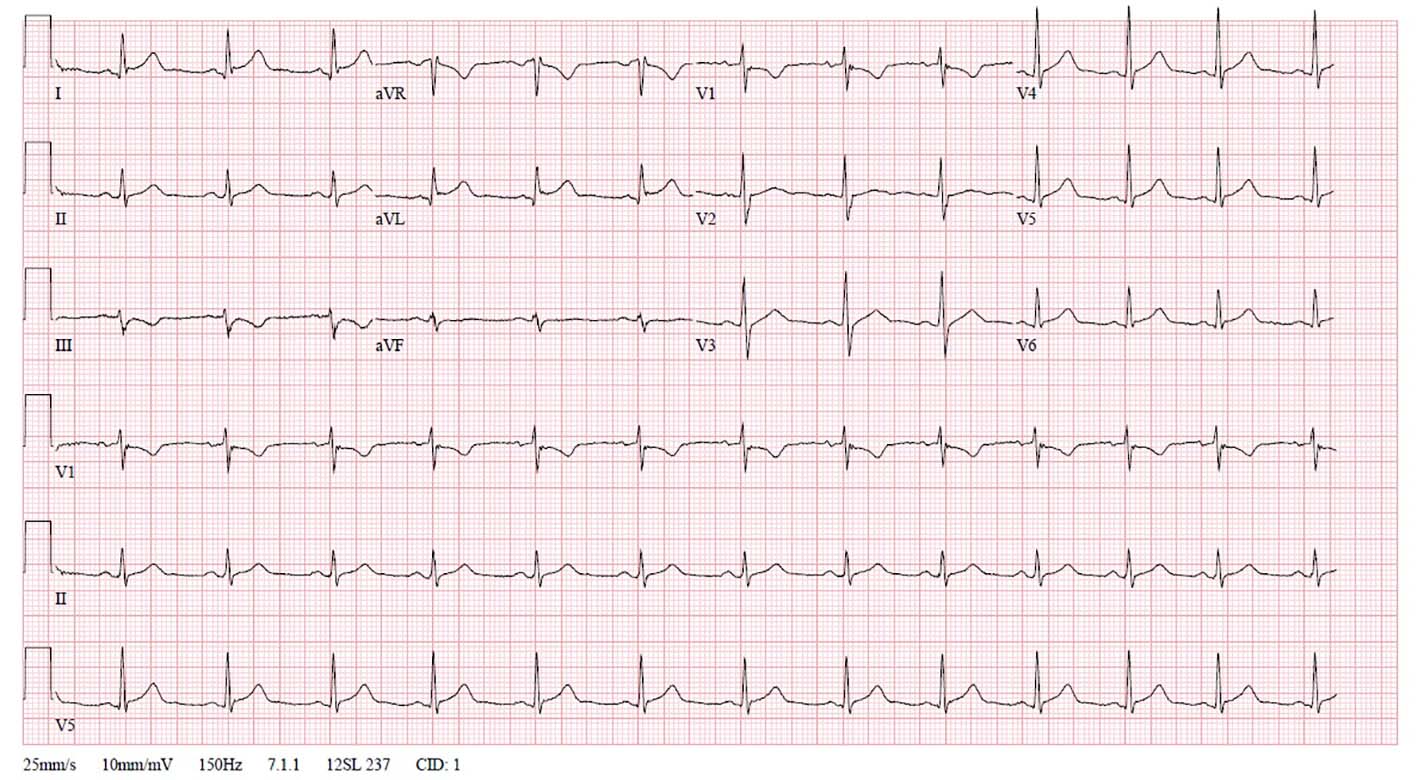
Figure 1. Electrocardiogram of presenting patient acquired upon arrival in the emergency department. Illustrative of ST elevation in lead I and aVL, and ST depression in lead III.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 7, Number 6, December 2016, pages 209-213
Diagnostic Approach to Myocarditis Mimicking Myocardial Infarction at Initial Presentation
Figures

Table
| Class I: clinical scenarios where EMB “should be performed” | |
| 1 | New-onset heart failure (HF) with onset < 2 weeks duration, in addition to: 1) normal or dilated left ventricle (LV); 2) hemodynamic compromise |
| 2 | New onset HF with duration 2 weeks to 3 months, in addition to either dilated LV and new ventricular arrhythmias or second/third degree heart block, or failure to respond to usual care within 1 to 2 weeks |
| Class IIa: clinical scenarios where EMB “may be considered reasonable” | |
| 3 | HF of more than 3 months duration, in addition to either dilated LV and new ventricular arrhythmias or second/third degree heart block, or failure to respond to usual care within 1 - 2 weeks |
| 4 | HF with dilated cardiomyopathy of any duration with suspected allergic reaction and/or eosinophilia |
| 5 | HF with suspected anthracycline cardiomyopathy |
| 6 | HF with unexplained restrictive cardiomyopathy |
| 7 | Suspected cardiac tumors (exception of typical myxomas) |
| 8 | Unexplained cardiomyopathy in the pediatric population |
| Class IIb: clinical scenarios where EMB “may be considered” | |
| 9 | HF with duration of 2 weeks to 3 months with a dilated LV, without new arrhythmia/heart block, that does respond to usual care within 1 - 2 weeks |
| 10 | Suspicion for iron overload in unexplained HF of > 3 months duration with a dilated LV, without arrhythmias/heart block, that does respond to usual care |
| 11 | HF associated with unexplained hypertrophic cardiomyopathy (if an infiltrative or storage disease is suspected) |
| 12 | Suspected arrhythmogenic right ventricular cardiomyopathy when other evaluations have been inconclusive |
| 13 | Unexplained ventricular arrhythmia |