Figures
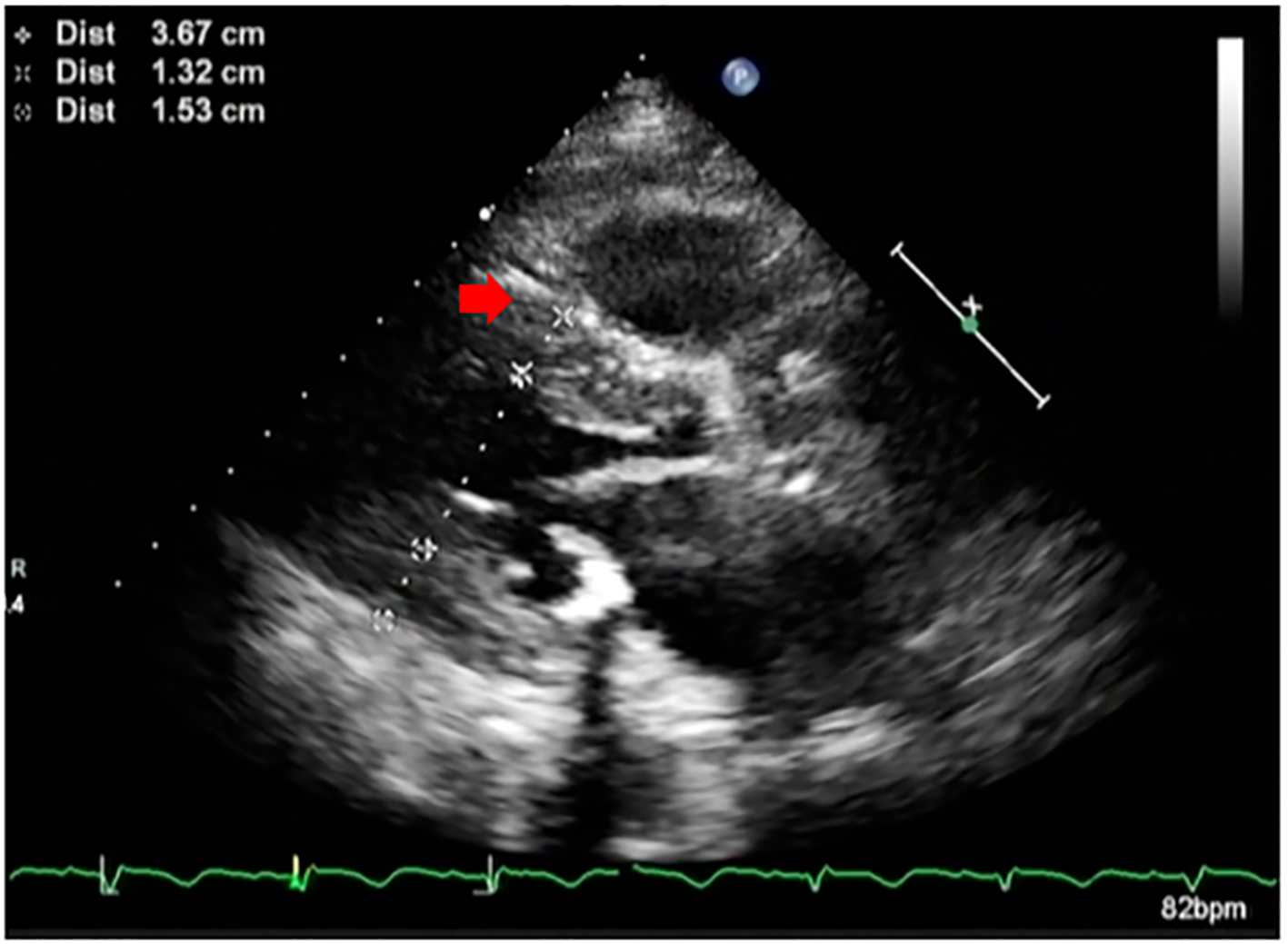
Figure 1. Parasternal long axis echocardiographic image of the patient showing hypertrophied septum (red arrow) and reduced left ventricular cavity size.
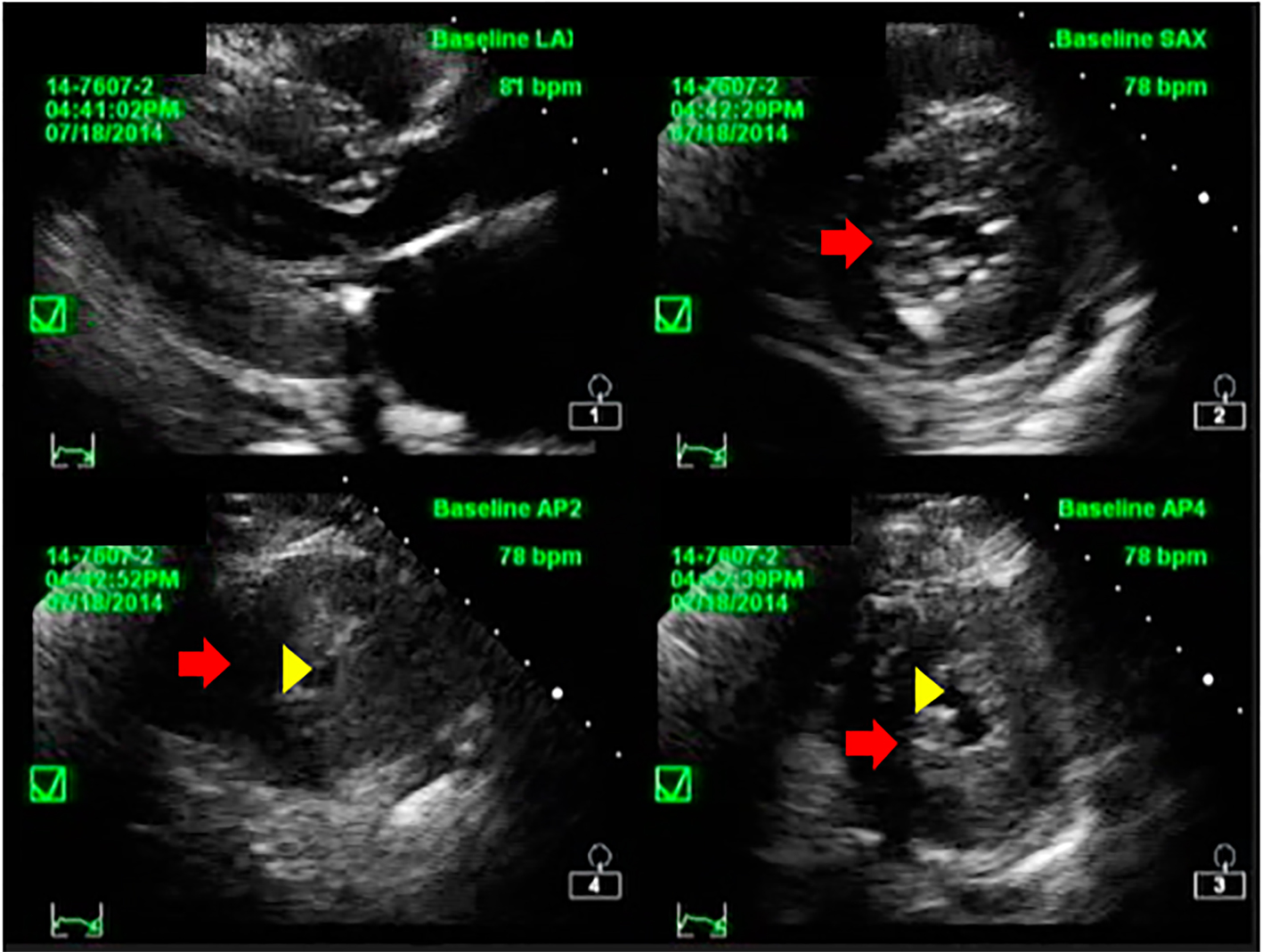
Figure 2. Short axis echocardiographic image of the patient showing concentric hypertrophy of the left ventricular wall (red arrow) and reduced LV cavity (yellow arrowhead).
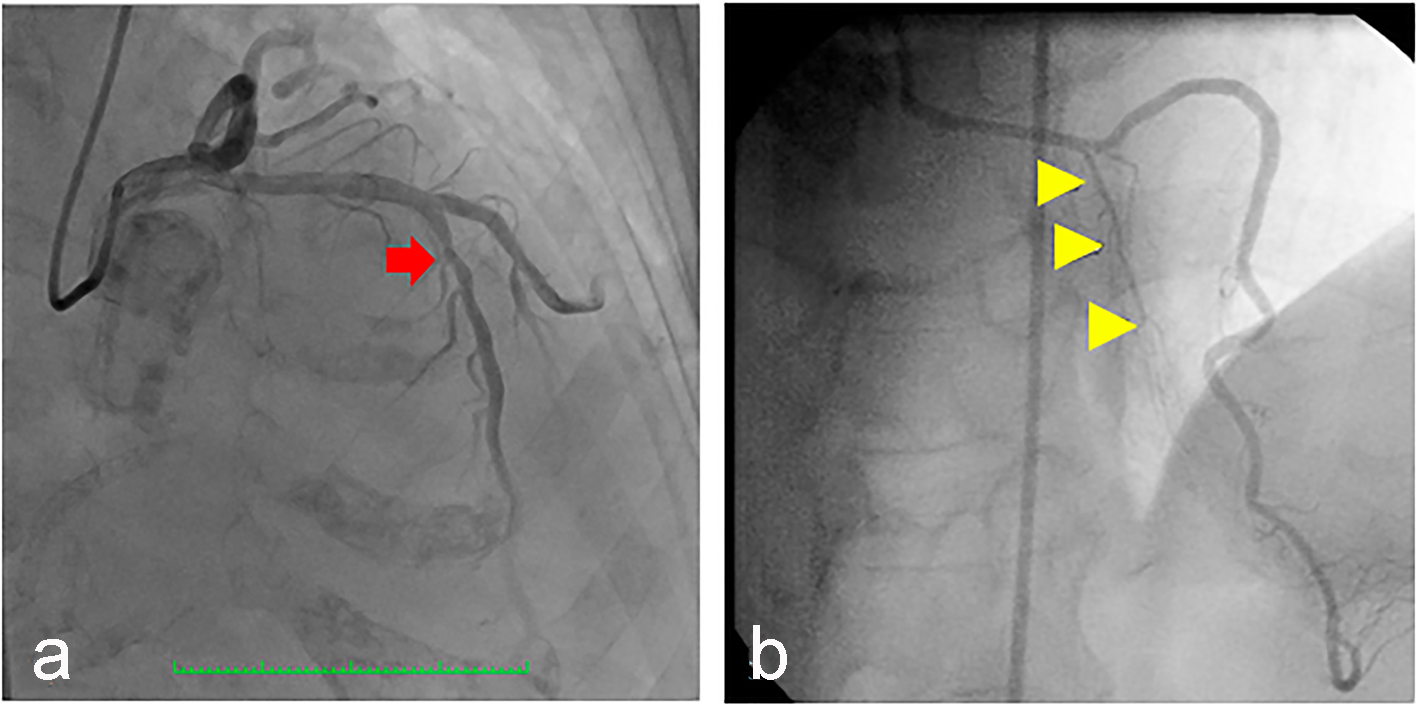
Figure 3. (a) Coronary angiography of the patient showing the left anterior descending artery (arrow) which was a good-sized vessel, with no significant stenosis but with absent first (major) septal perforator branch. (b) Normal major septal perforator (yellow arrowheads) originating from the long LAD from a 52-year-old female [11].
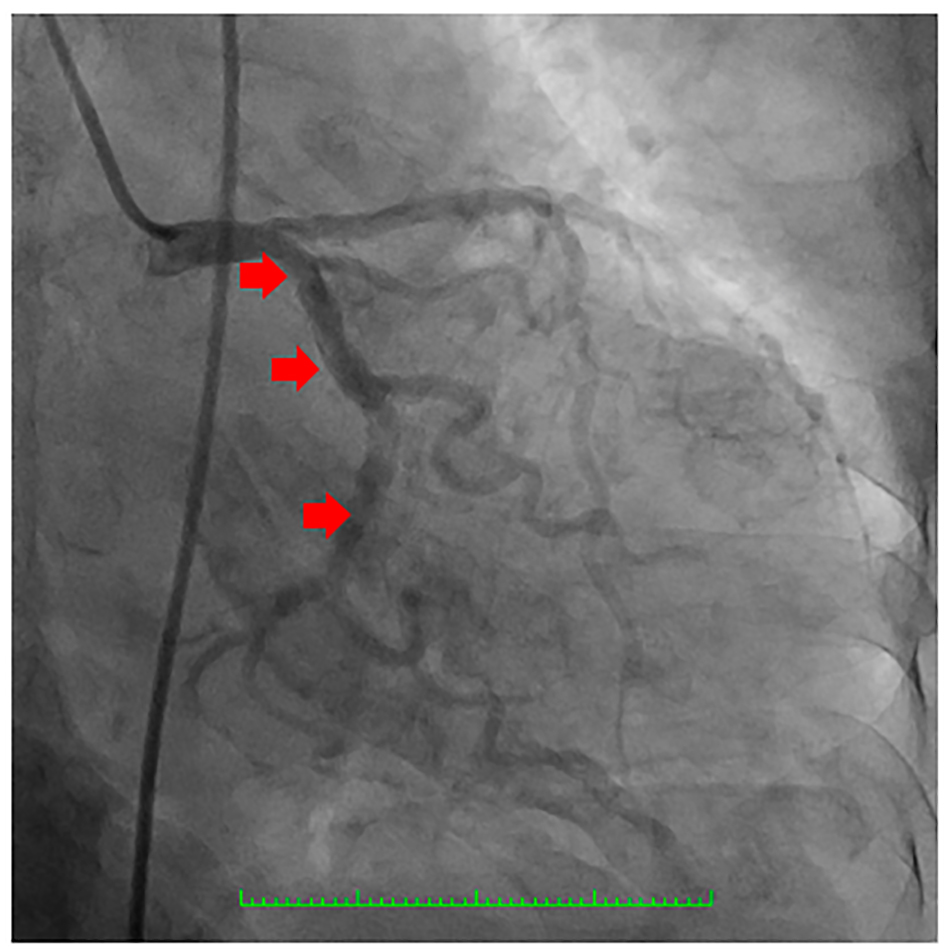
Figure 4. Coronary angiography showing the left circumflex coronary artery which was a good-sized vessel with no significant stenosis (arrows).
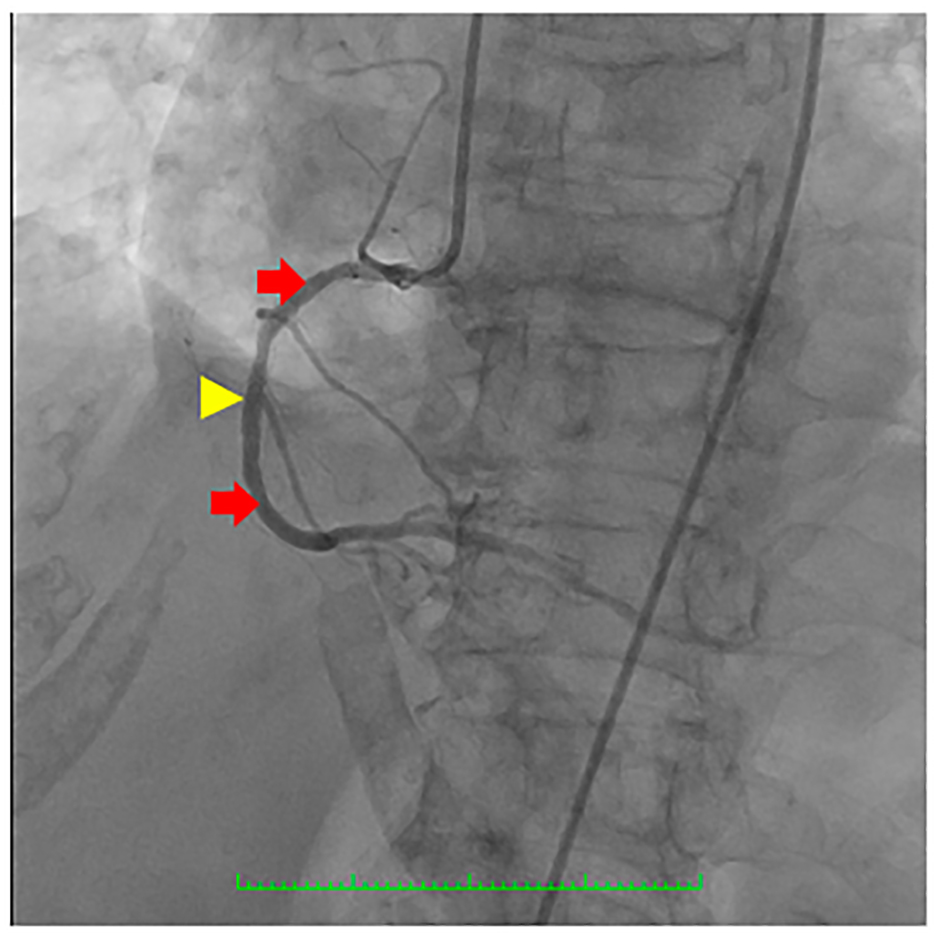
Figure 5. Coronary angiography showing the right coronary artery (RCA) (red arrows) which was a good-sized vessel with patent stent at the proximal to mid segment (yellow arrowhead) with good flow and with no significant stenosis.
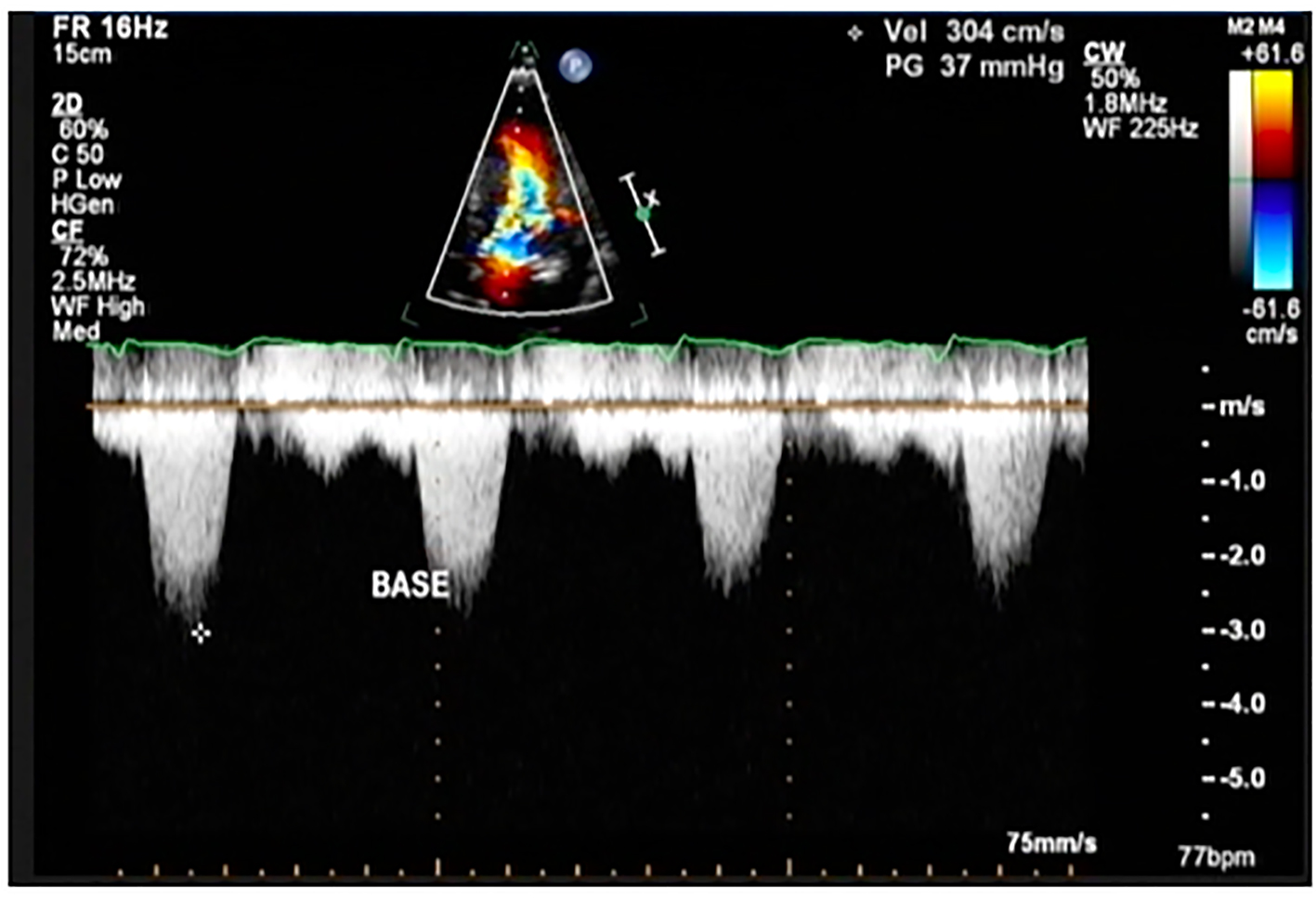
Figure 6. Color flow Doppler study of the patient showing a peak instantaneous gradient of 37 mm Hg at post-implantation of dual chamber pacemaker (This was previously described as 194 mm Hg before implantation pacemaker).