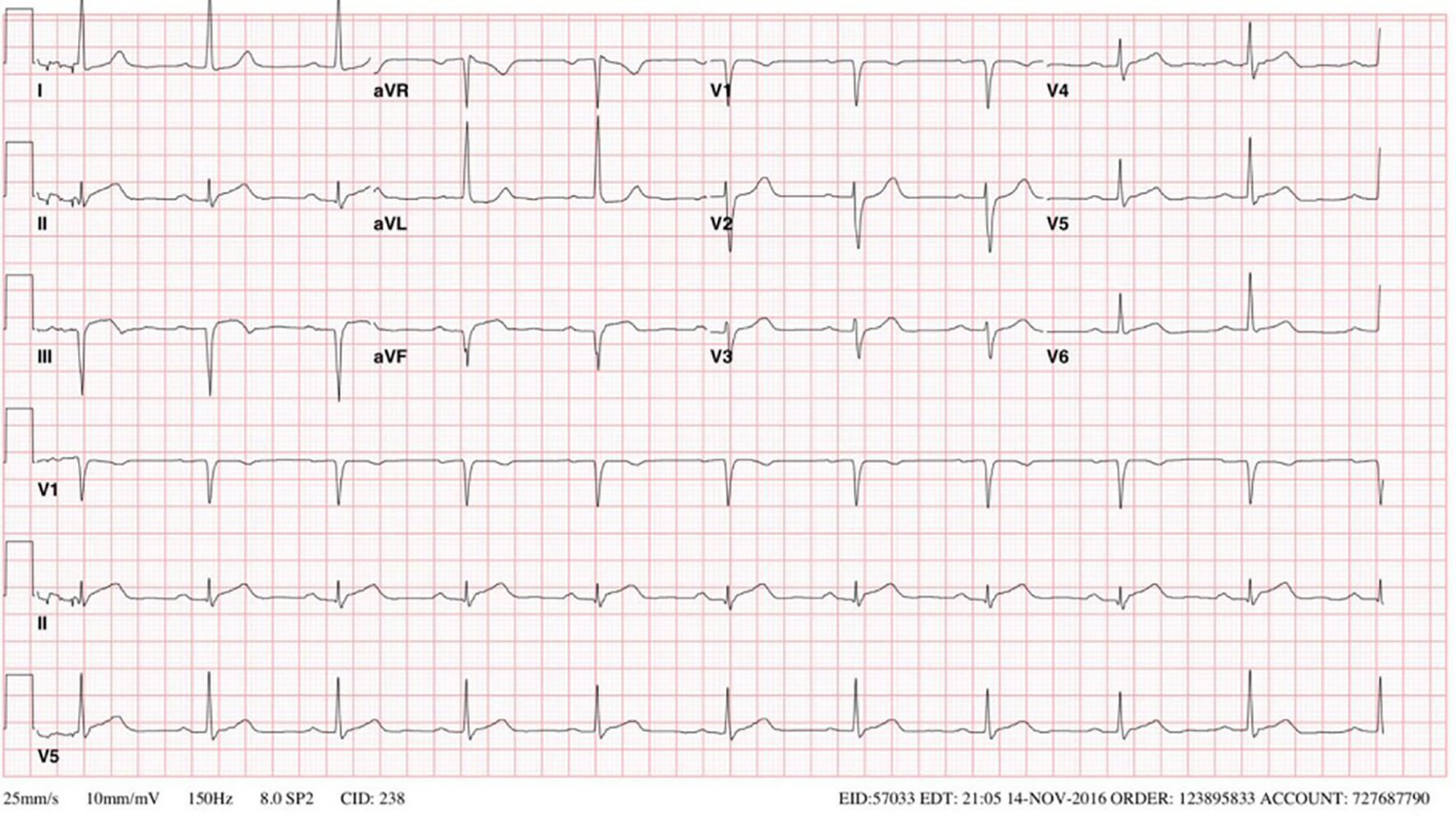
Figure 1. EKG done on 2009 showing sinus bradycardia, first degree AV block and ST segment elevations > 0.1mV in the inferior leads II, III, and aVF. EKG: electrocardiogram; AV: atrioventricular.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 8, Number 6, December 2017, pages 344-348
A History of Kawasaki Disease From Childhood and Coronary Artery Ectasia With Recurrent ST Elevation Myocardial Infarction: A Therapeutic Challenge
Figures