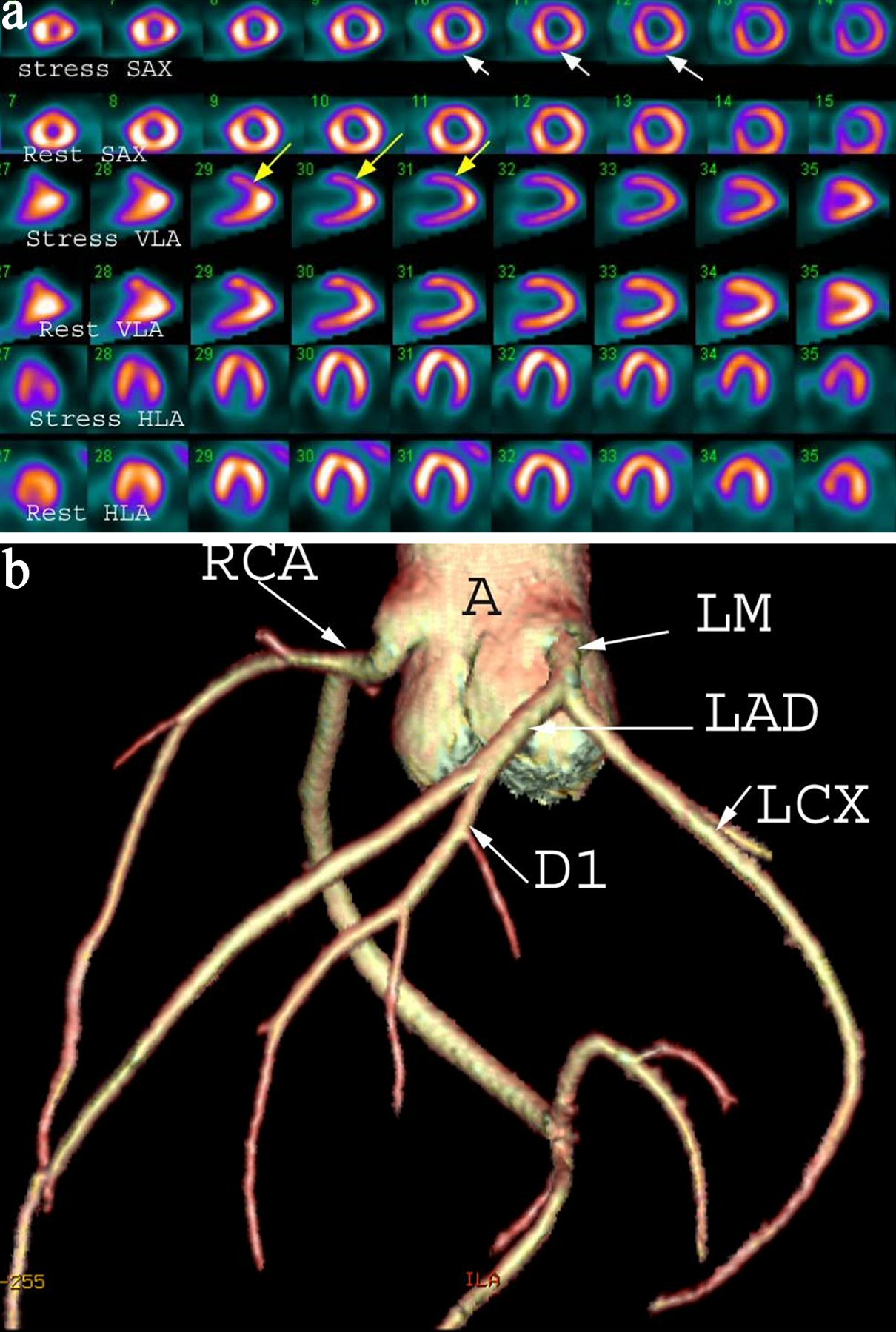
Figure 1. (a) A 42-year-old female with chest pain and shortness of breath. Myocardial perfusion scintigraphy demonstrates reversible defects in the apex and anterior wall (yellow arrows) and inferior wall (white arrows) suggesting inducible ischemia. Gated images (not shown) demonstrate mildly dilated left ventricular cavity and global hypokinesis and impaired left ventricle ejection fraction of 35%. SAX: short axis; VLA: vertical long axis; HLA: horizontal long axis. (b) Shaded surface display coronary computed tomography angiogram demonstrating normal coronary arteries without calcified or non-calcified plaques. A: ascending aorta; LM: left main; LAD: left anterior descending artery; D1: first diagonal artery; LCX: left circumflex artery; RCA: right coronary artery.