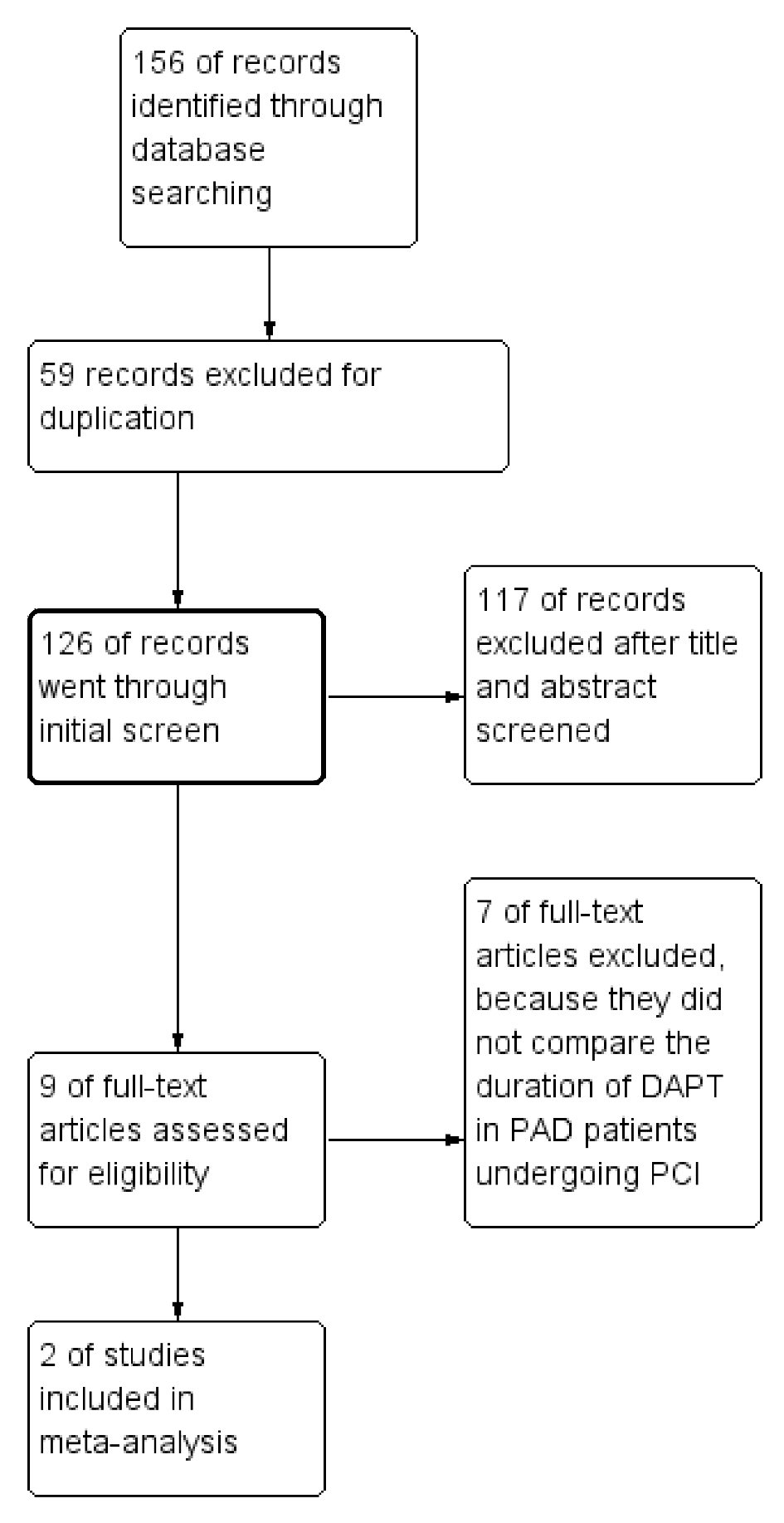
Figure 1. Summary of the study selection and exclusion process.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 9, Number 3, June 2018, pages 137-143
Extended Duration Dual Antiplatelet Therapy After Percutaneous Coronary Intervention in Patients With Peripheral Arterial Disease: A Meta-Analysis
Figures






Tables
| The PRODIGY trial | The DAPT trial | |
|---|---|---|
| CABG: coronary artery bypass grafting; MI: myocardial infarction; PAD: peripheral artery disease; SD: standard deviation. | ||
| No of patients | 1970 | 11,648 |
| No of patients with PAD | 246 | 649 |
| Randomization groups | Aspirin 75 - 160 mg/d + clopidogrel 75 mg/d vs. aspirin + placebo | Aspirin 75 - 162 mg/d + clopidogrel 75 mg/d or prasugrel 10/5 mg/d vs. aspirin + placebo |
| Follow-up | ≤ 6-month vs. 24-month | 12-month vs. 30-month |
| Age among patients with PAD (SD) | 74.5 (8.94) | 66.2 (9.57) |
| Male among patients with PAD | 76.83% | 70.42% |
| Diabetes mellitus among patients with PAD | 33.74% | 44.29% |
| Hypertension among patients with PAD | 87.40% | 87.98% |
| Smoking among patients with PAD | 15.45% | 28.55% |
| Congestive heart failure among patients with PAD | 6.50% | 14.73% |
| Prior PCI among patients with PAD | 23.98% | 40.87% |
| Prior CABG among patients with PAD | 17.89% | 25.15% |
| Prior MI among patients with PAD | 40.65% | 30.77% |
| Indication for PCI | ||
| STEMI among patients with PAD | 20.32% | 4.62% |
| NSTE-ACS among patients with PAD | 52.44% | 26.81% |
| Stable angina among patients with PAD | 27.23% | 44.53% |
| DAPT trial | PRODIGY trial | |||||
|---|---|---|---|---|---|---|
| % Patients with PAD (n = 649) | % Patients without PAD (n = 10,999) | P value | % Patients with PAD (n = 246) | % Patients without PAD (n = 1,724) | P value | |
| ST: stent thrombosis; MACCE: major adverse cardiovascular and cerebrovascular event; MI: myocardial infarction. | ||||||
| MACCE | 11.65 (73) | 4.62 (494) | < 0.001 | 21.9 (54) | 8.4 (144) | < 0.001 |
| MI | 5.88 (36) | 2.90 (308) | < 0.001 | 7.5 (18) | 3.6 (62) | 0.006 |
| Definite/probable ST | 1.47 (9) | 0.83 (88) | 0.094 | 3.0 (7) | 1.2 (21) | 0.04 |
| GUSTO moderate/severe bleeding | 4.86 (30) | 1.74 (185) | < 0.001 | 2.6 (6) | 2.7 (45) | 0.95 |