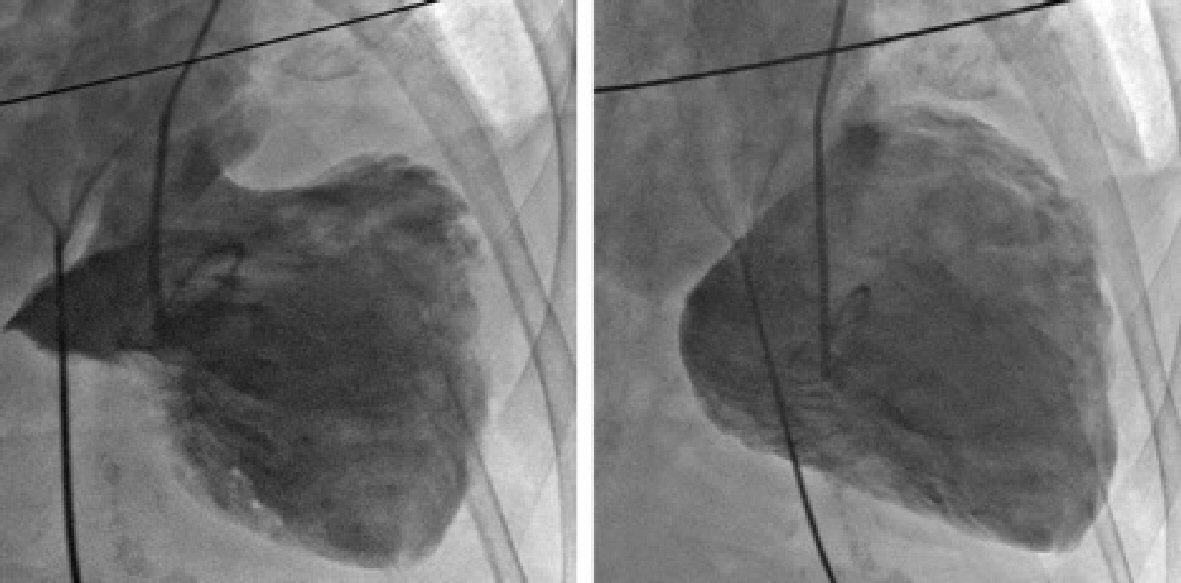
Figure 1. Left ventriculogram showing the characteristic apical ballooning of TCM with moderate to severe mitral regurgitation.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 9, Number 4, August 2018, pages 244-249
Takotsubo Cardiomyopathy-Induced Cardiac Free Wall Rupture: A Case Report and Review of Literature
Figures


Table
| Study | Age (Y) | Gender | EKG findings | Pathology findings | Interval to rupture |
|---|---|---|---|---|---|
| Akashi et al [22] | 70 | F | STE in leads I, II, III, aVL, aVF, V2 - V6. Pathologic Q waves were present in leads V1 - V5 | Not done | 75 h |
| Ishida et al [27] | 67 | F | STE in leads I, aVL, and V2 - V5 without reciprocal ST depression | Not done | 7 days |
| Ohara et al [20] | 79 | F | STE in leads I, aVL and V1 - V5, depression in leads III and aVF, and abnormal Q wave in leads V1 - V4 | Rupture in the anterior portion of the LV. Microscopically, inflammatory infiltrates and myocyte necrosis was evident at the site of the rupture with normal surrounding myocardial tissue | 7 days |
| Mafrici et al [28] | 87 | F | STE in the inferior and V2 - V6 leads | Not done | 1 day |
| Yamada et al [29] | 71 | F | STE in leads V4 - V6 and abnormal Q waves in leads V4 - V5 | Not done | 16 h |
| Sacha et al [24] | 81 | F | STE in leads I, II, III, aVL, aVF, V2 - V6 | 10 mm apical LV free wall rupture. Microscopically, transmural necrosis with hemorrhage and mild focal PMNL infiltration at the rupture site. Around the rupture, there were multiple fused foci of coagulation necrosis in various phase of myodestruction with contraction band necrosis | 44 h |
| Shinozaki et al [19] | 90 | F | STE in leads I, aVL and V1 - V4 | Not done | 8 days |
| Stollberger et al [30] | 71 | F | STE and Q waves in leads II, III, aVF, V5 - V6 | 5 mm LV rupture in the apico-posterior region | 4 h |
| Tsunoda et al [31] | 74 | F | STE in leads I, aVL, and V3 - V6; ST-depression in leads II, III, aVF; and R-wave diminishment in leads V3 and V4 | 11mm rupture at the anterior LV wall 30 mm above the apex and a small mural thrombus inside the necrotic wall. Microscopically, there were inflammatory cell infiltrations, interstitial fibrosis, hemorrhage, and coagulation necrosis without evidence of contraction band necrosis | 10 days |
| Kurisu et al [18] | 81 | F | STE in leads I, II, III, aVF and V2 - V6 | Not done | 64 h |
| Mendiguchia et al [32] | 69 | F | STE in the anterolateral leads | Not done | 2 days |
| Jagszewski et al [23] | 82 | F | STE in leads V1 - V5 | Wide penetrating apical rupture. Microscopically, there were hypertrophied and disarrayed cardiomyocytes, surrounded by predominantly mononuclear inflammatory infiltrate and loose connective tissue as well the foci of hemorrhage | 5 days |
| Kumar et al [21] | 62 | F | STE in leads I, II, V5 - V6 | Slit-like transmural rupture at the midportion of the posterior ventricular wall with overlying epicardial hemorrhage. Microscopically, there were necrotic fibers with increased eosinophilic staining, contraction band necrosis, along with PMNL infiltration and bundles of wavy myocardial fibers | 8 h |
| Hassan et al [26] | 73 | M | STE and Q waves in the inferior leads and ST depression over the anterolateral leads | 1.2 cm perforation at the infero-basal region | Not reported |
| Indorato et al [25] | 70 | F | Not reported | 0.4 cm apical rupture with hemorrhagic infarction extending from the anterior to posterior wall of LV. Microscopically, there were neutrophilic infiltration with small areas of spotty necrosis, hemorrhagic changes and a form of catecholaminergic myocarditis | 4 h |