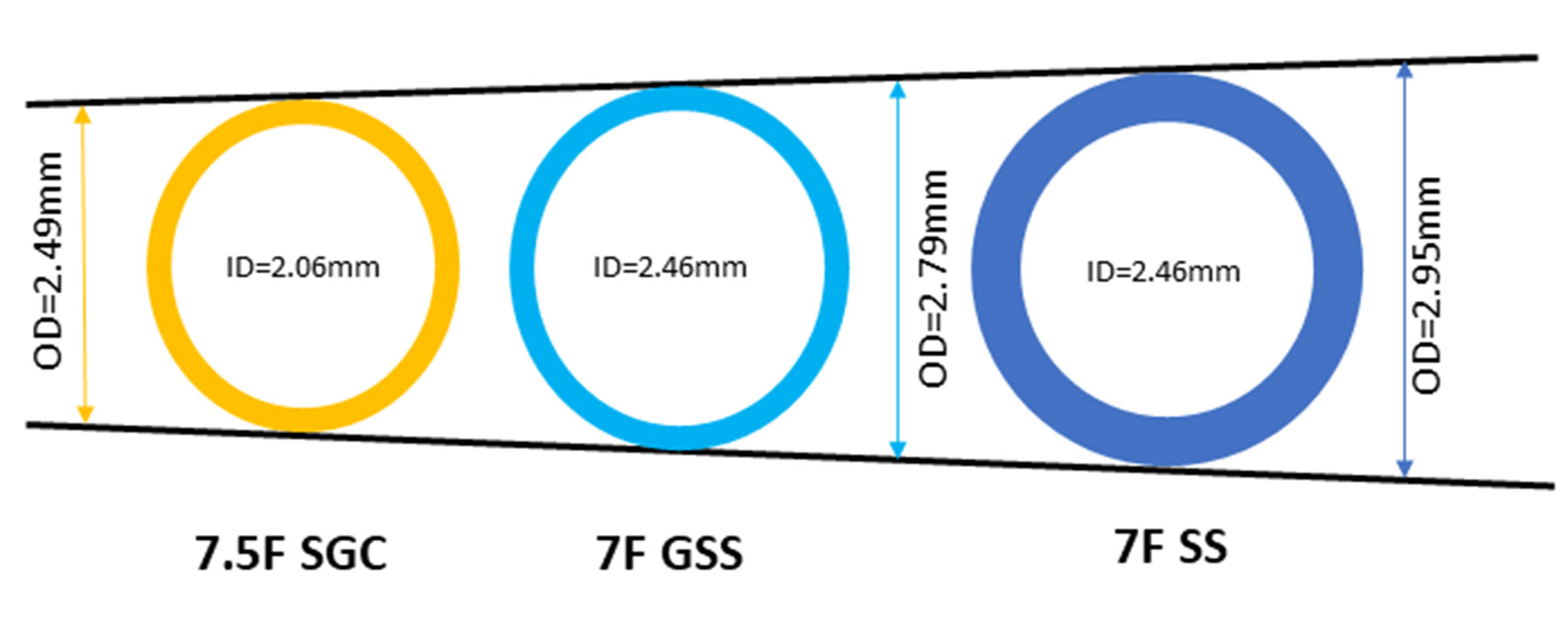
Figure 1. Internal and outer diameters of 7F standard sheath, 7.5F Eaucath sheathless guiding catheter and 7F glidesheath slender sheath. SS, standard sheath; SGC, sheathless guiding catheter; GSS, glidesheath slender sheath.
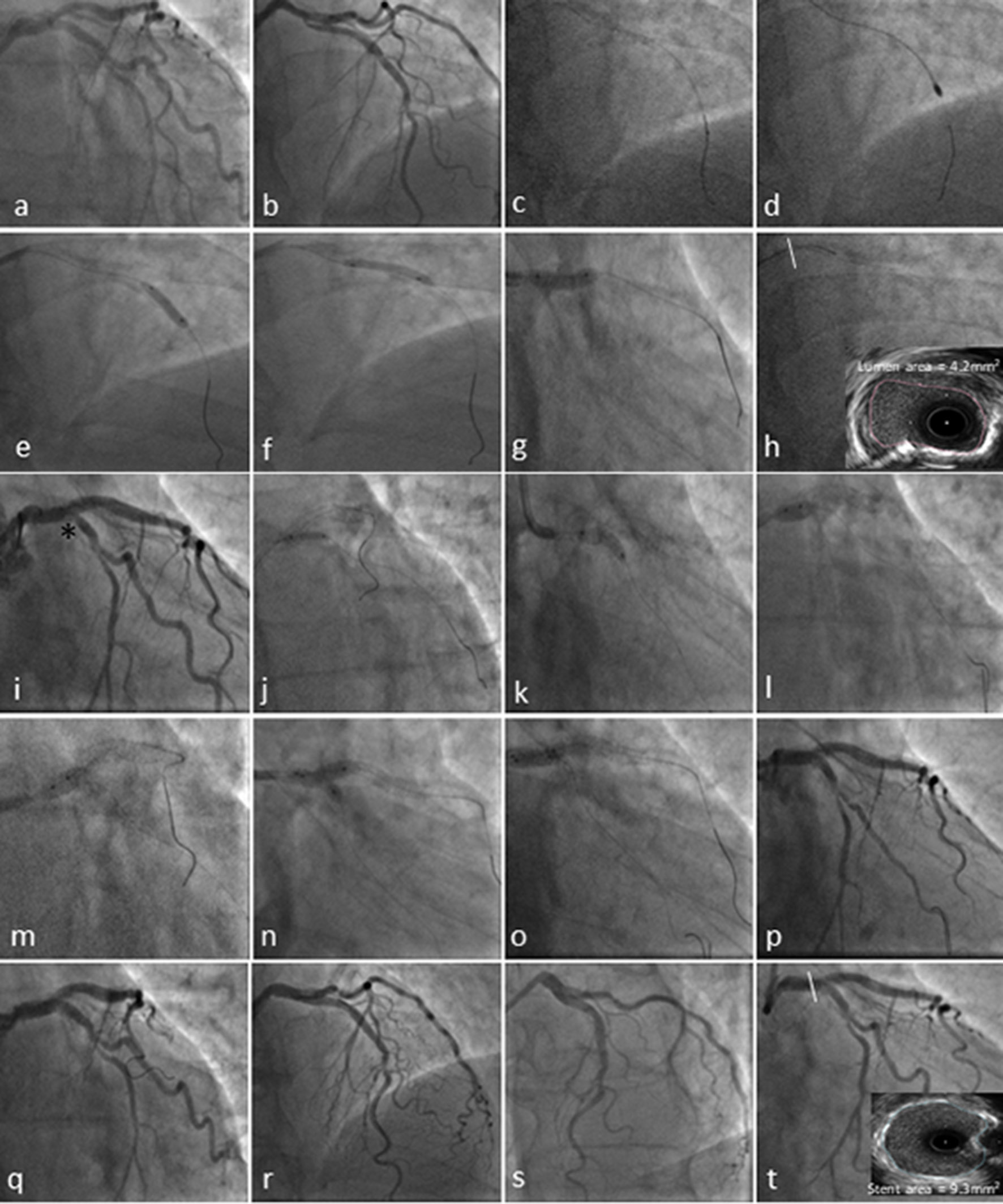
Figure 2. Coronary angiography and transradial percutaneous coronary intervention using the 7.5F Eaucath sheathless guide catheter. Coronary angiography demonstrated severe ostial and mid left anterior descending (LAD) disease and at least moderate distal calcified left main stem (LMS) (1,1,0 Medina) disease in a right coronary artery (RCA) unobstructed dominant system (not shown). The circumflex (LCx) ostium was angiographically free of disease, with a mild lesion just before the bifurcation with a relatively big first obtuse marginal (a and b). The LAD was wired with a BMW wire and exchanged using a Finecross microcatheter with the rotawire (2c). A 1.75-mm burr was used to ablate LMS and LAD lesions (2d), and predilated with a 3.0 × 15 mm and 3.5 × 15 mm NC Quantum Apex balloons (e-g). The pullback IVUS images showed significant calcified disease in the distal LMS with a cross-sectional luminal area of 4.2 mm2 (2h). The mid LAD lesion was stented with 3.5 × 16 mm Promus Premier and a second stent Promus Premier 4.0 × 28 mm was implanted from LMS to LAD across the Cx and post-dilated with a 4.5 NC Quantum Apex balloon (i). Due to the threatened morphology of the LCx ostium and an FFR 0f 0.78 following LMS/LAD stenting (i*), we decided to convert the strategy to a two-stent bifurcation culotte procedure. We crossed the LCx with a Pilot 50 wire and opened the struts of LMS to Cx with a semi-compliant balloon Sprinter Legend 2.0 × 12 mm (j). A 3.5 × 12 mm Promus Premier was implanted from LMS to Cx (k) and then potted the LMS with a 4.5 × 6 mm NC Quantum Apex (l and m). A final kissing balloon inflation was performed with a 3.5 × 12 mm NC balloon in the LAD and 3.25 × 12 mm NC balloon in Cx (n and o). A good angiographic result was obtained in LMS, LAD and Cx (p-s) with a post-PCI IVUS in distal LMS demonstrating a stent area of 9.3 mm2.