Figures
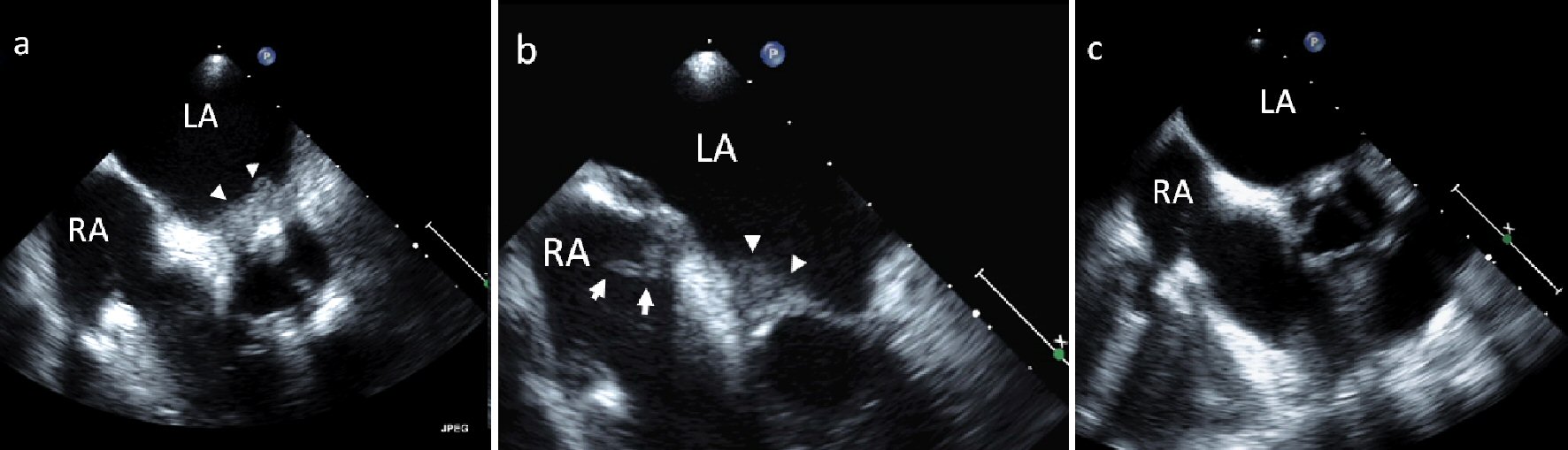
Figure 1. (a, b) TEE of sessile masses in the LA and RA (arrow heads) as well as a pedunculated mass in the RA (arrow with tail) in a patient with rheumatoid arthritis. (c) TEE 2 months after initiation of warfarin, prednisone, and cessation of methotrexate shows near-complete resolution of the atrial masses.
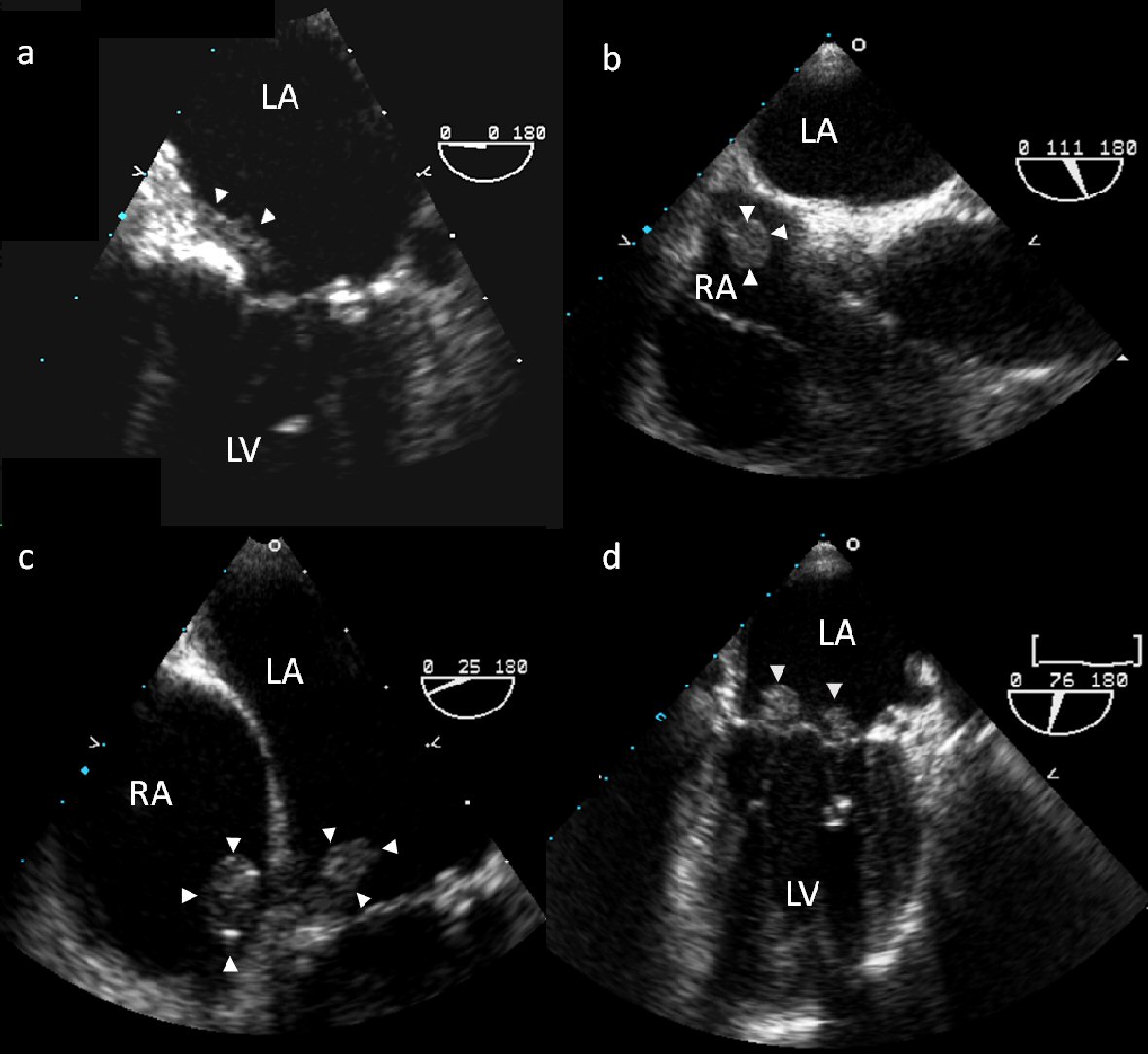
Figure 2. TEE of echodensities associated with the atrial surface of the mitral valve (a) and the posterior RA free wall (b). TEE 1 month following surgical resection shows new pedunculated masses in the RA and on the mitral and tricuspid valves (c, d).
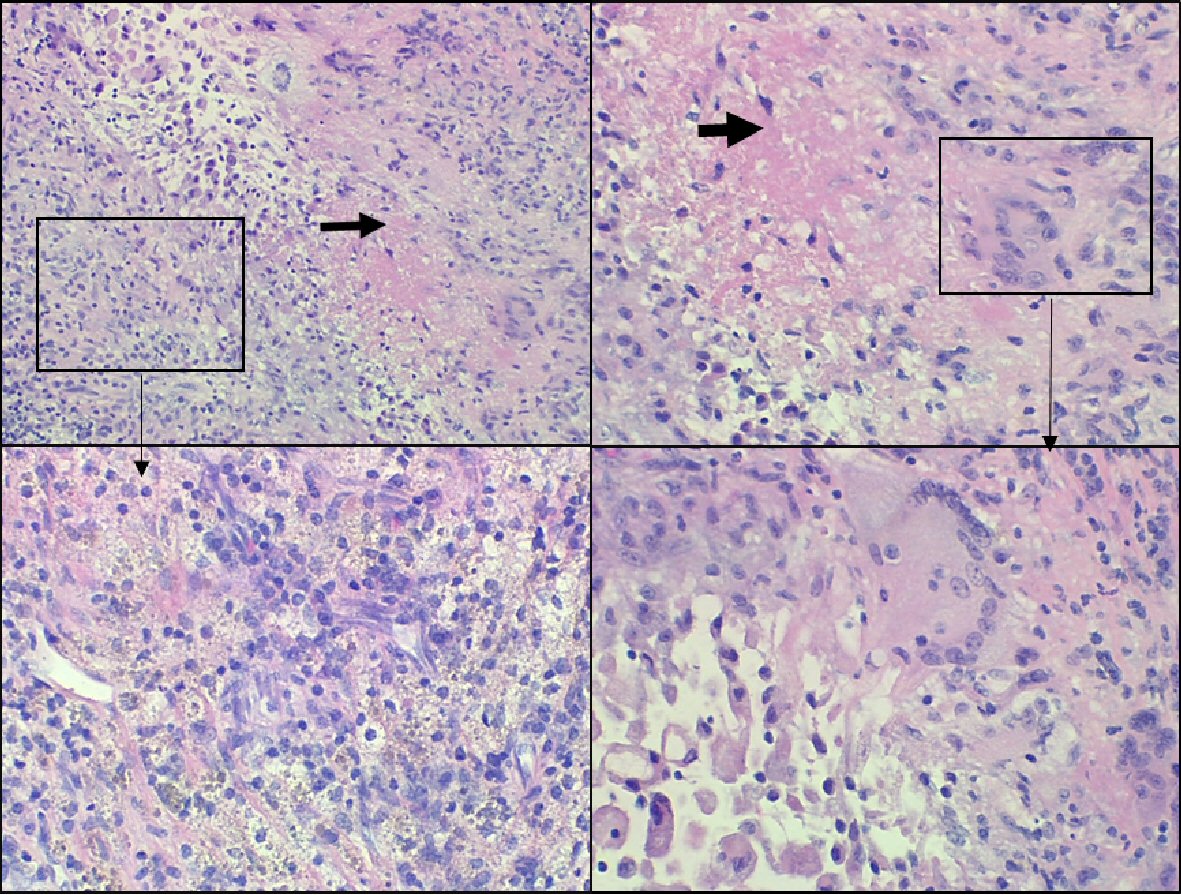
Figure 3. Surgical pathology images of right atrial mass. Lesional area showing necrosis (black arrow) containing eosinophilic debris surrounded by histiocytes, lymphocytes, plasma cells, and giant cells (box). These changes are compatible with rheumatoid nodule.
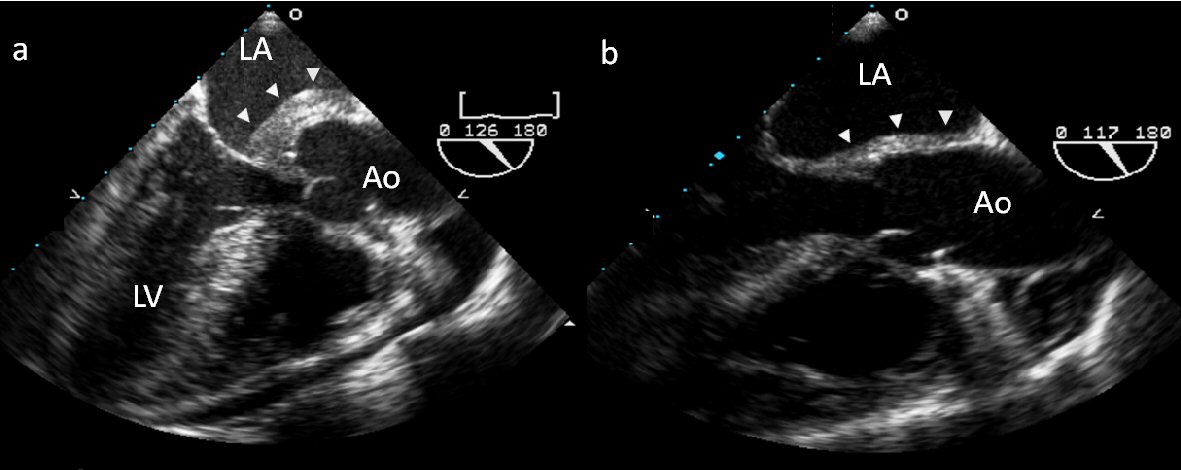
Figure 4. (a) TEE of a large complex mass invading the intaatrial septum and encasing the aortic root. Cyclophosphamide and prednisone were started and serial TTEs showed progressive regression of the aortic mass. (b) Follow-up TEE the following year shows near resolution.
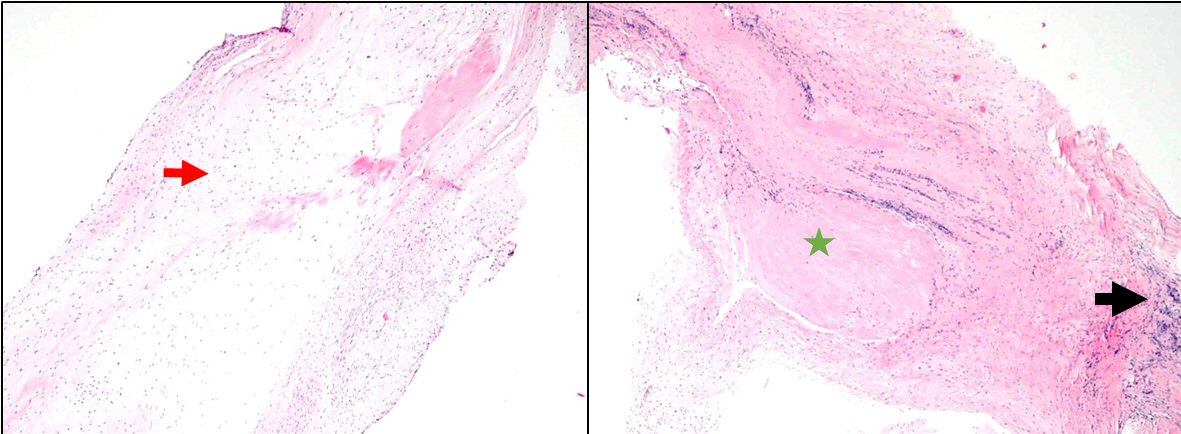
Figure 5. Surgical pathology images of valvular tissue: valvular tissue with myxoid changes (red arrow), focal chronic inflammation (black arrow), and fibrosis (green star). These changes could represent changes compatible with previously active vasculitis.
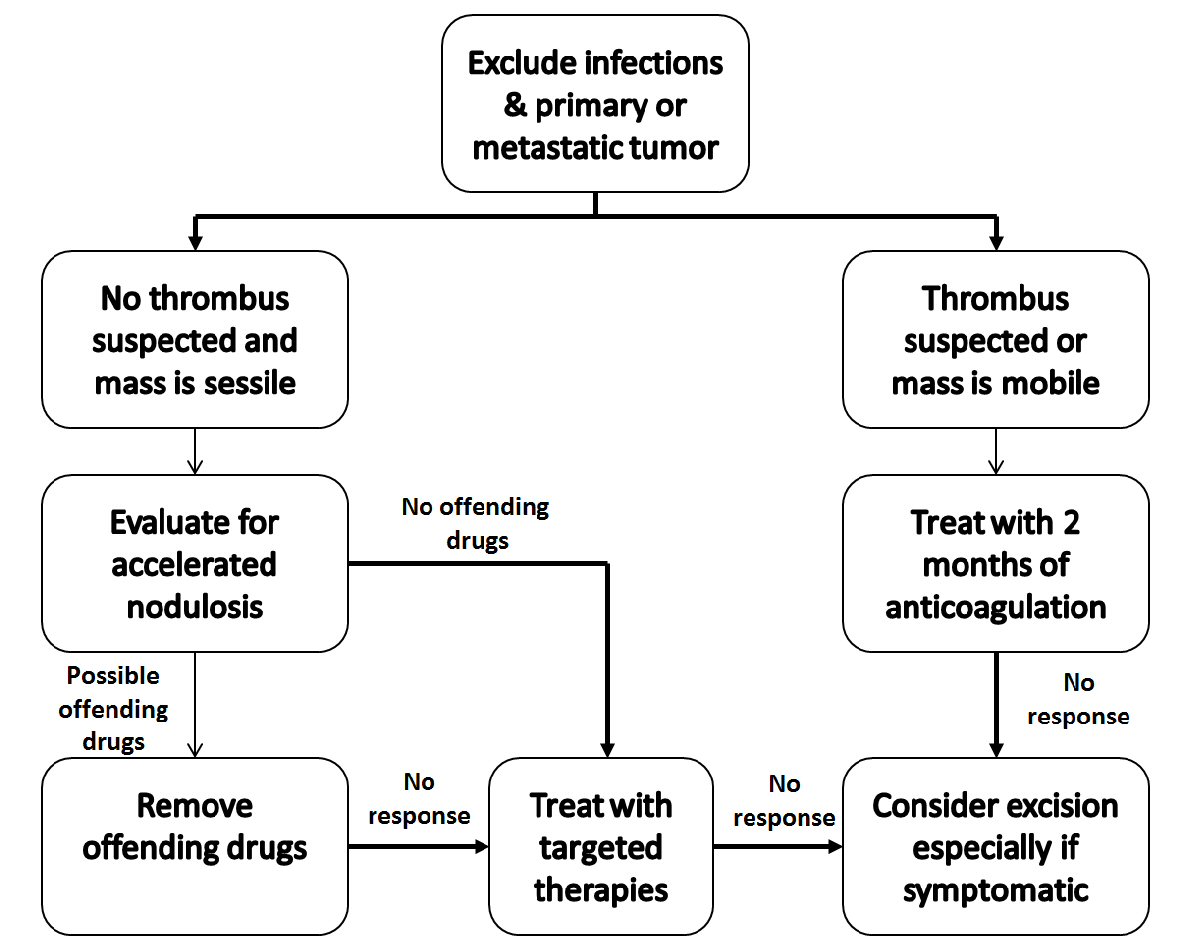
Figure 6. Proposed management strategy for suspected inflammatory cardiac masses.