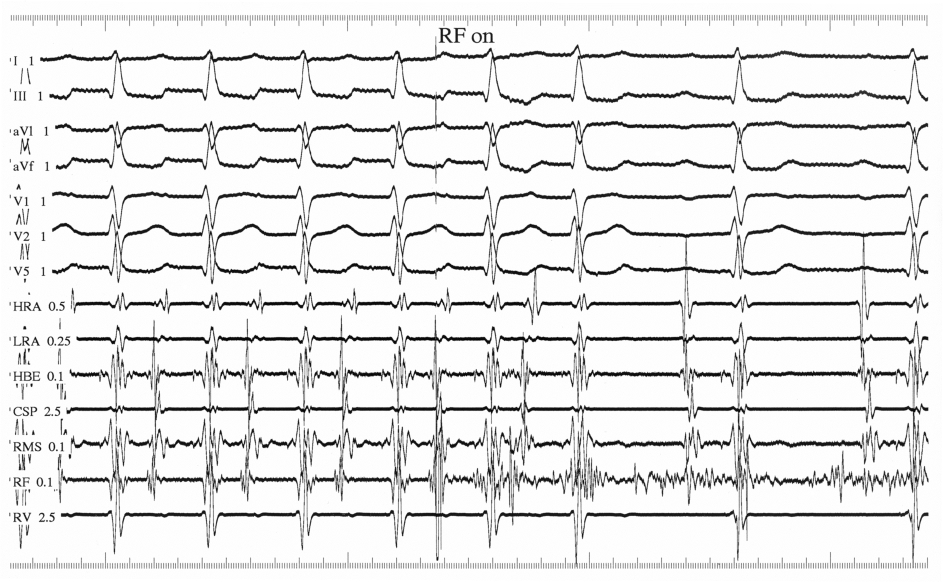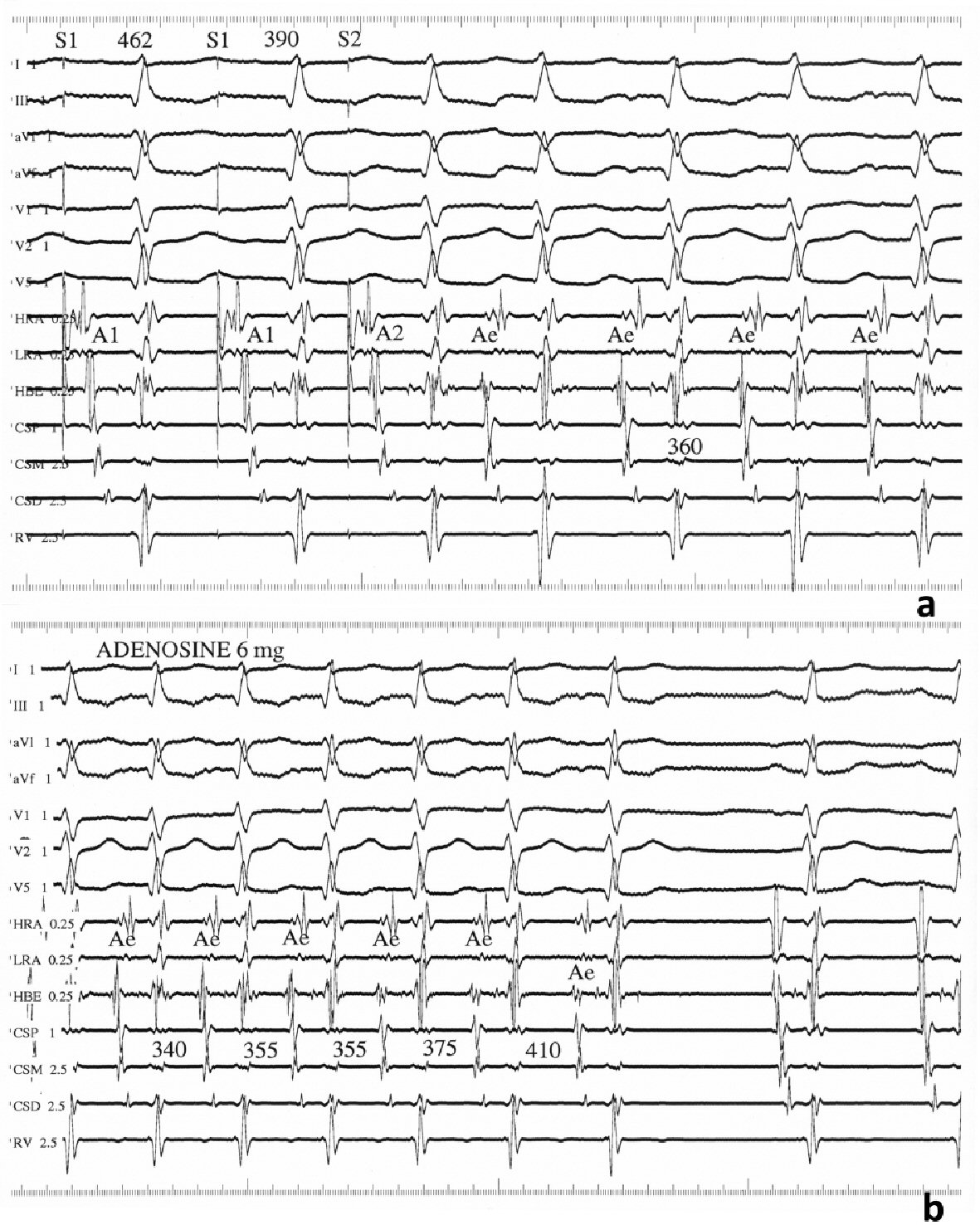
Figure 1. Findings from the electrophysiological study. (a) Intracardiac recordings showing tachycardia induction with an atrial extrastimulus at a prematurity (S1S2) of 390 ms coupled with a drive cycle length (S1S1) of 462 ms. Paper speed = 100 mm/s. (b) Tachycardia termination after intravenous bolus of 6 mg adenosine. Paper speed = 75 mm/s. A1, A2, and Ae: atrial electrograms; CSP, CSM, and CSD: proximal, middle, and distal coronary sinus, respectively; HRA: high right atrium; HBE: His-bundle electrogram; LRA: low right atrium; RV: right ventricular apex.
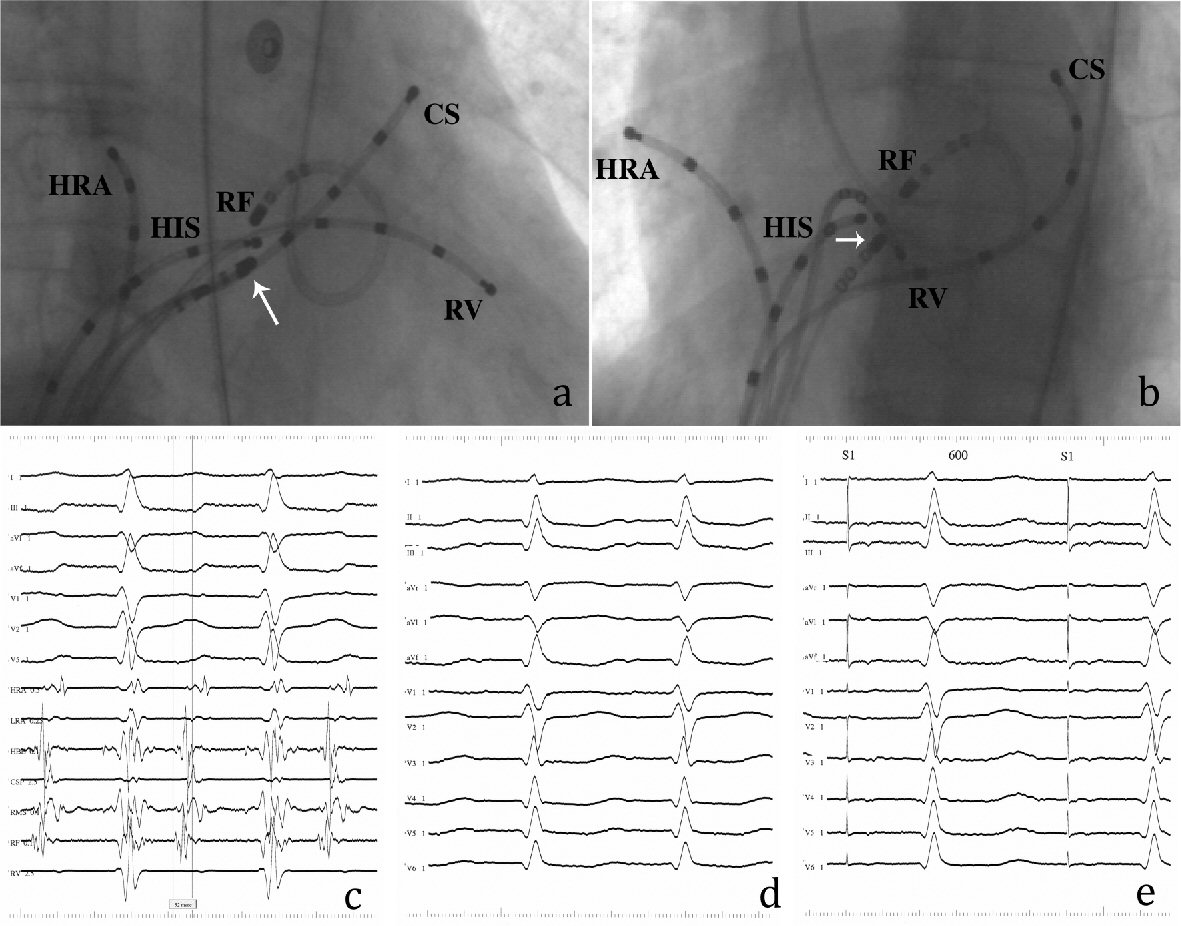
Figure 2. Findings from the retrograde transaortic/transmitral approach. (a) Right anterior oblique and (b) left anterior oblique radiographs of the RF ablation catheter positioned at the successful ablation site of left atrial septum. White arrows indicate the tip of a steerable catheter positioned in the right atrial mid-septum (RMS). (c) Bipolar electrogram from the RF catheter during tachycardia. The local atrial electrogram precedes the P wave by 52 ms without a recordable His-bundle potential. (d) Twelve-lead ECG during tachycardia. (e) Perfect pace map obtained from the successful ablation site. The other abbreviations are shown in Figure 1.