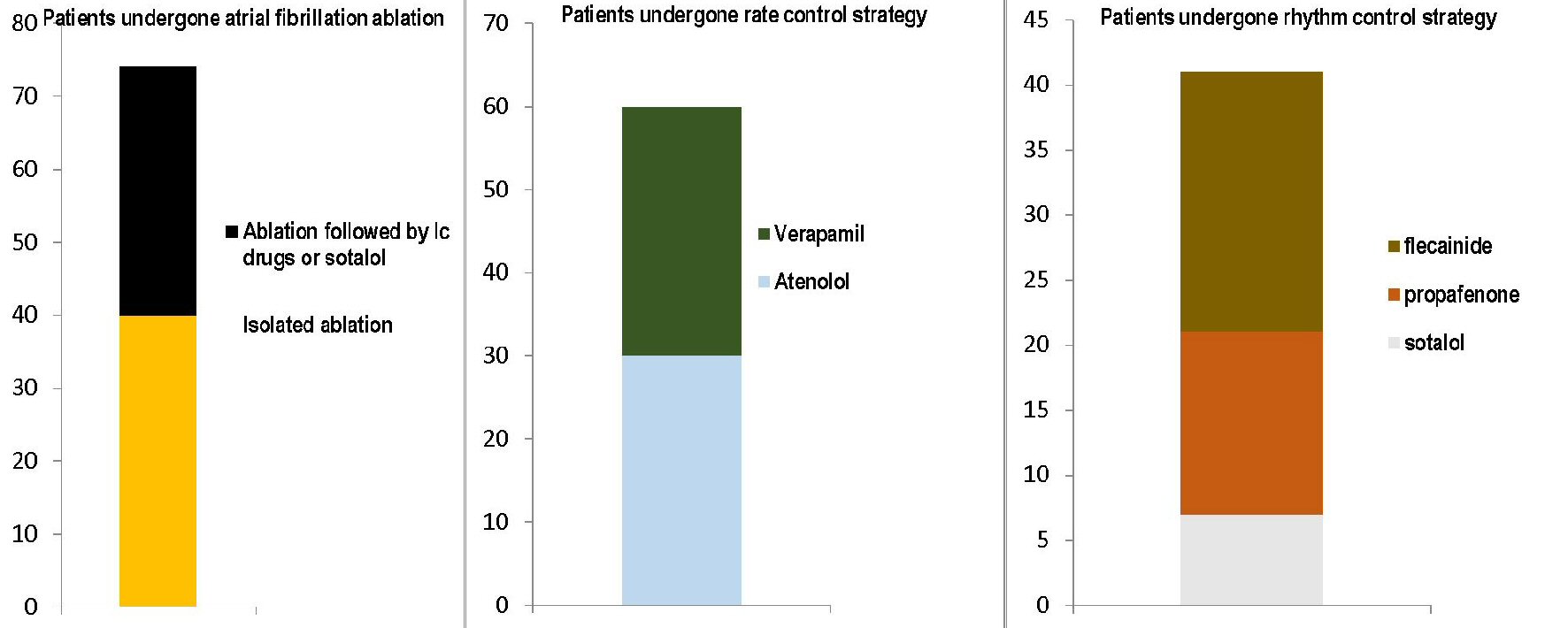
Figure 1. The figure shows the respective distributions of the three therapeutic approaches used in the series of 175 patients included in the present cohort retrospective study. The three graphs with stacked layers refer each to one of the three therapeutic modalities adopted: on the left, the transcatheter ablation, involving 74 patients, of whom 40 subjected to simple ablation and 34 with ablation followed by chronic administration of antiarrhythmics, namely IC drugs or sotalol; at the center, the rate control strategy with the use of atenolol (30 cases) or verapamil (30 cases); on the right the rhythm control strategy, with the bar consisting of three layers representing the use of sotalol (seven cases), propafenone (14 cases) and flecainide (20 cases), respectively.
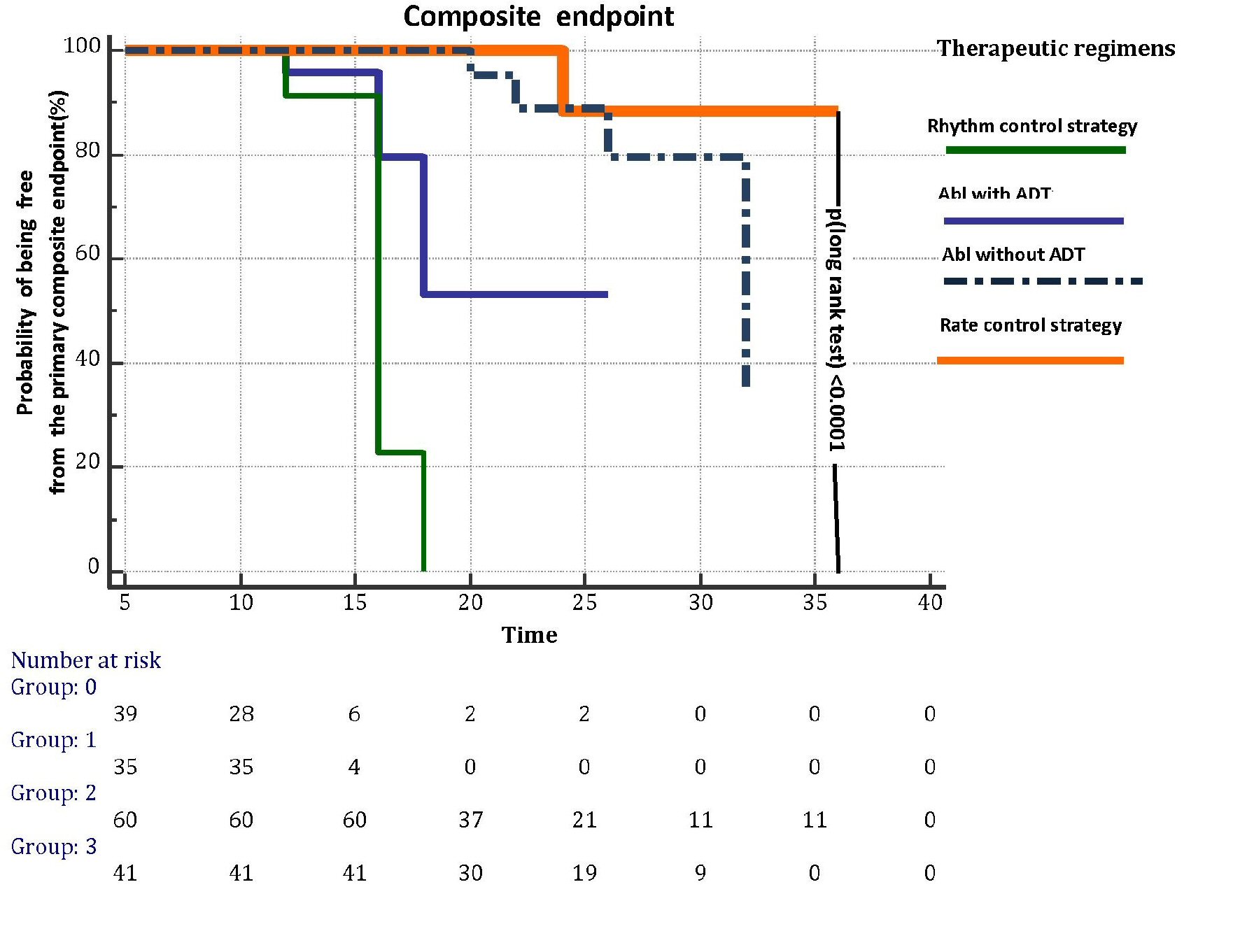
Figure 2. Kaplan-Meier curves illustrating the effects on primary composite endpoint, i.e., death, disabling stroke, major bleeding and cardiac arrest, exerted by each of the four therapeutic regimens for AF prevention (rhythm control strategy, abl with ADT, abl without ADT and rate control strategy) investigated in the retrospective study through a median follow-up of 20 months. Abl: transcatheter ablation; AF: atrial fibrillation; ADT: antiarrhythmic drug treatment.
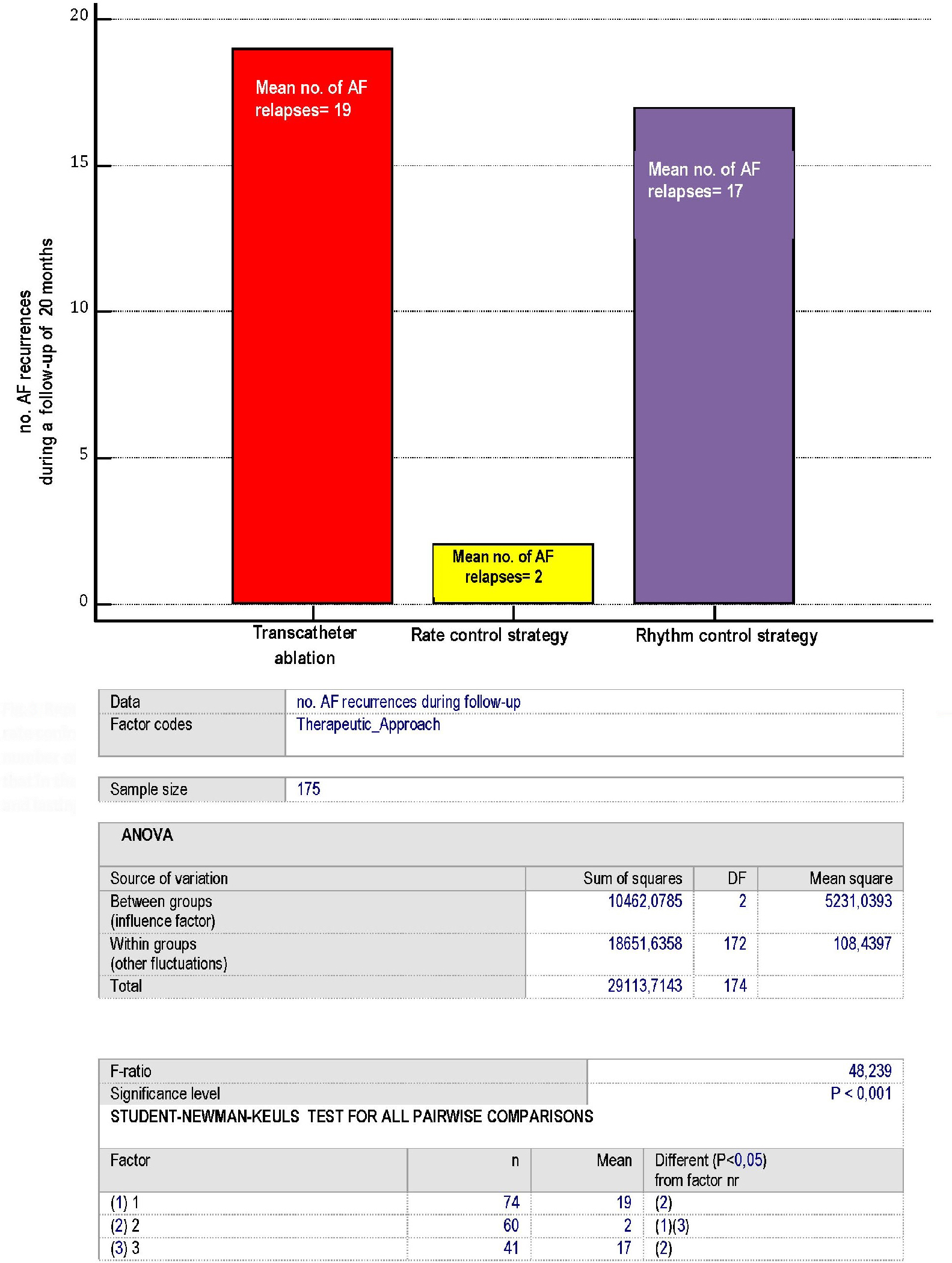
Figure 3. Representation of the AF recurrences, according to the type of therapeutic approach: whether consisting of ablation, rate control or rhythm control strategy. Please note that each of the numbers reported within the bars coincides with the mean number of AF recurrences identified for every patient of the three arms over a 20- month median follow-up. Moreover, note that in the rate control strategy group any rise in mean ventricular response occurring at rest attaining 140 beats per minute and lasting no less than 30 min was arbitrarily equated to an AF relapse. AF: atrial fibrillation.