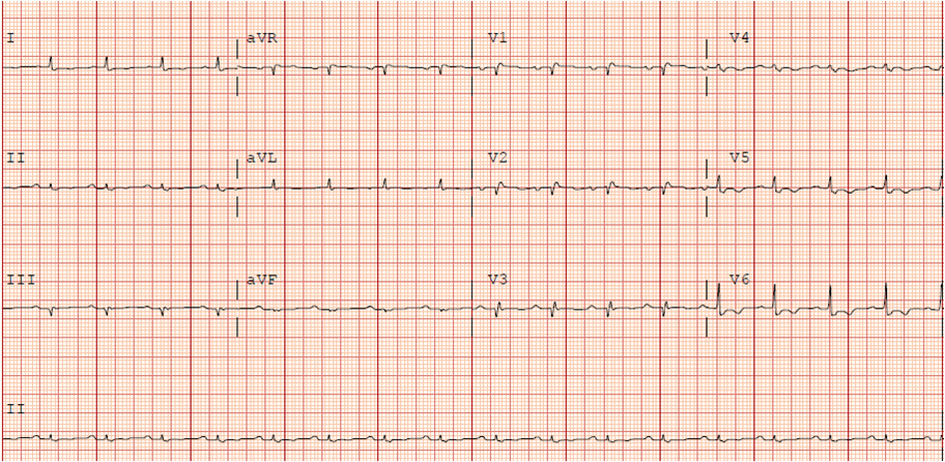
Figure 1. ECG on July 27, 2018: left axis deviation, sinus tachycardia and low voltage.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Case Report
Volume 10, Number 2, April 2019, pages 120-123
A Case of Acute Heart Failure due to Immune Checkpoint Blocker Nivolumab
Figures
Table
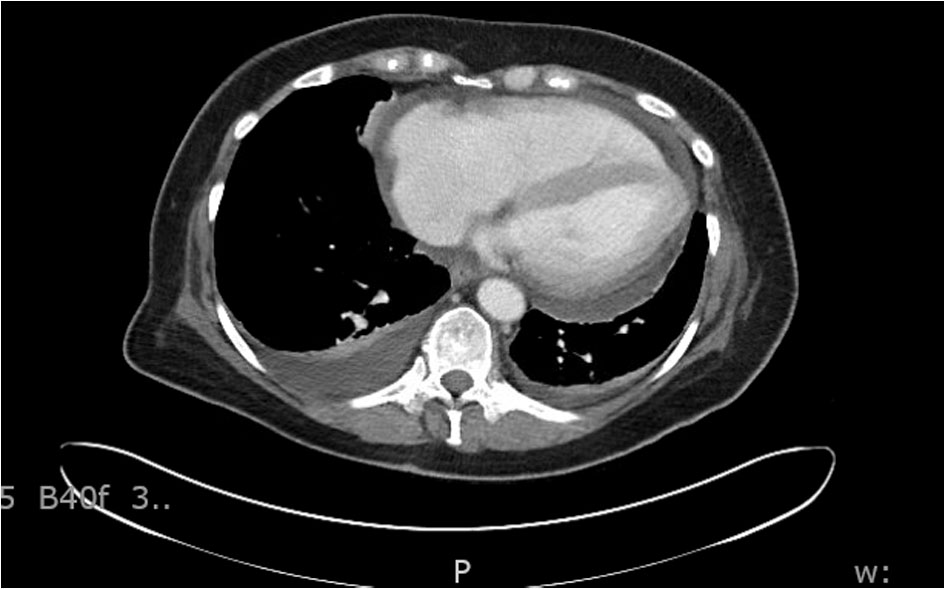
| Pericardium | Moderate pericardial effusion |
|---|---|
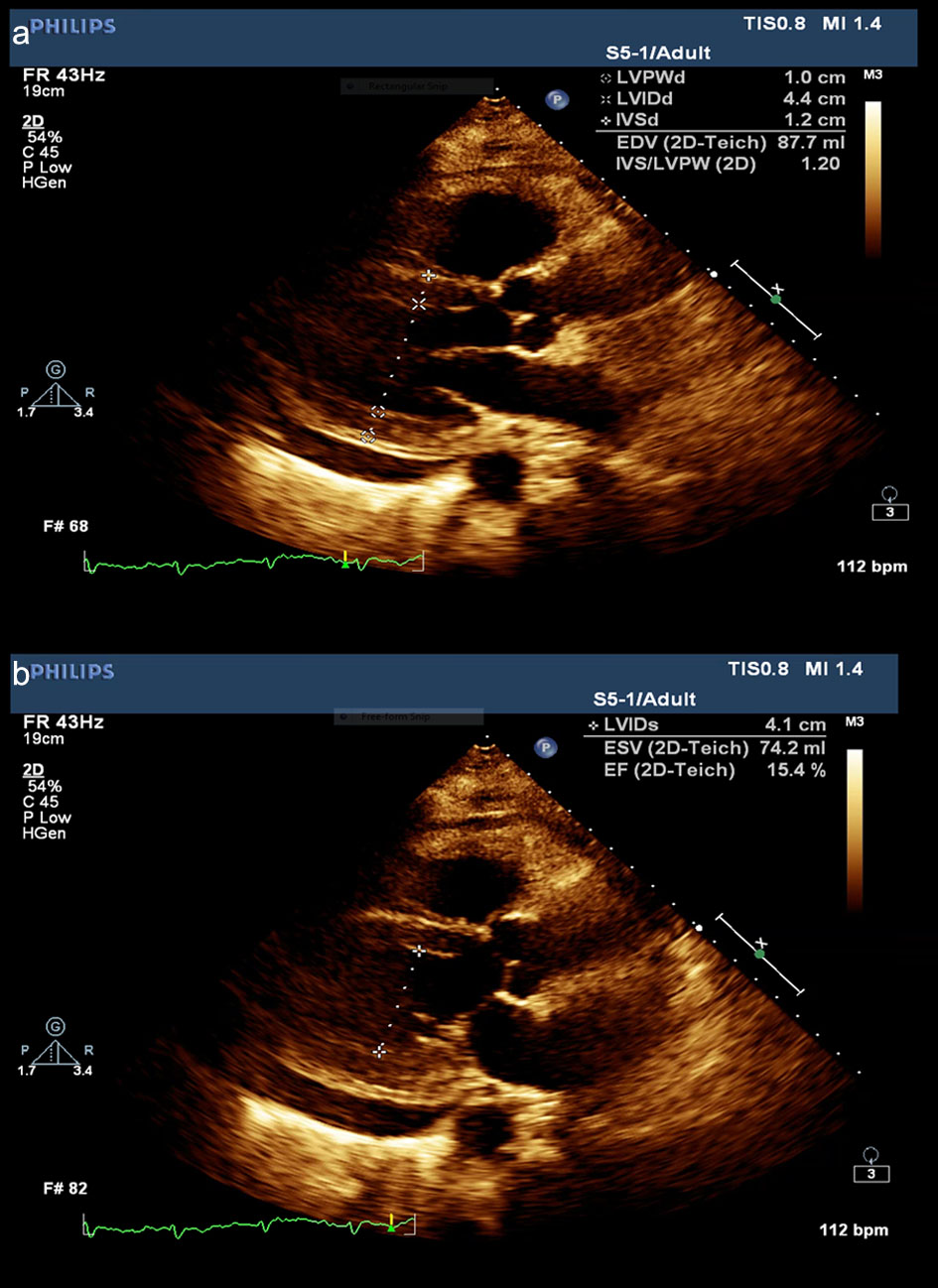
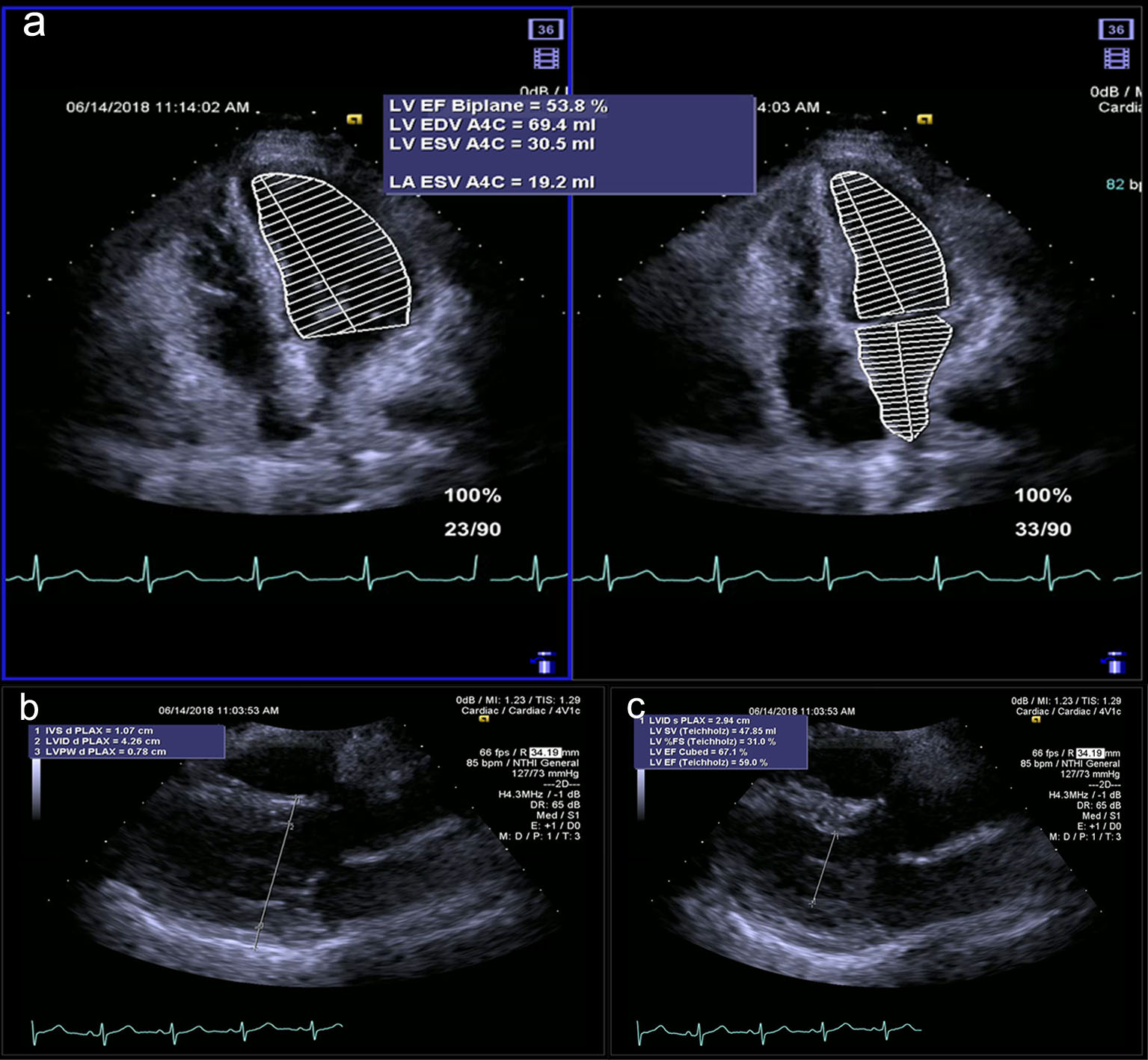
| In comparison to the previous study dated June 14, 2018, there is significant change noted (moderate pericardial effusion is seen and LVEF is severely reduced at < 20%). | |
| Left ventricle | Severely reduced systolic function, ejection fraction estimated at less than 20%, unable to assess left ventricle diastolic function (tachycardia), mild asymmetric hypertrophy |
| Right ventricle | Cavity mildly dilated |
| Right atrium | Cavity mildly dilated |
| Inferior vena cava | Dilated (> 2.1 cm) with less than 50% respiratory collapse with an estimated right atrial pressure of 15 mm Hg |
| Mitral valve | Mild to moderate regurgitation on color-flow PW Doppler |
| Tricuspid valve | Moderate to severe regurgitation on color-flow PW Doppler |
| Aortic valve | The aortic valve is sclerotic without reduced excursion, no stenosis, trace regurgitation on color-flow PW Doppler |
| Pulmonic valve | The pulmonic valve was not well visualized, trace regurgitation on color-flow PW Doppler |