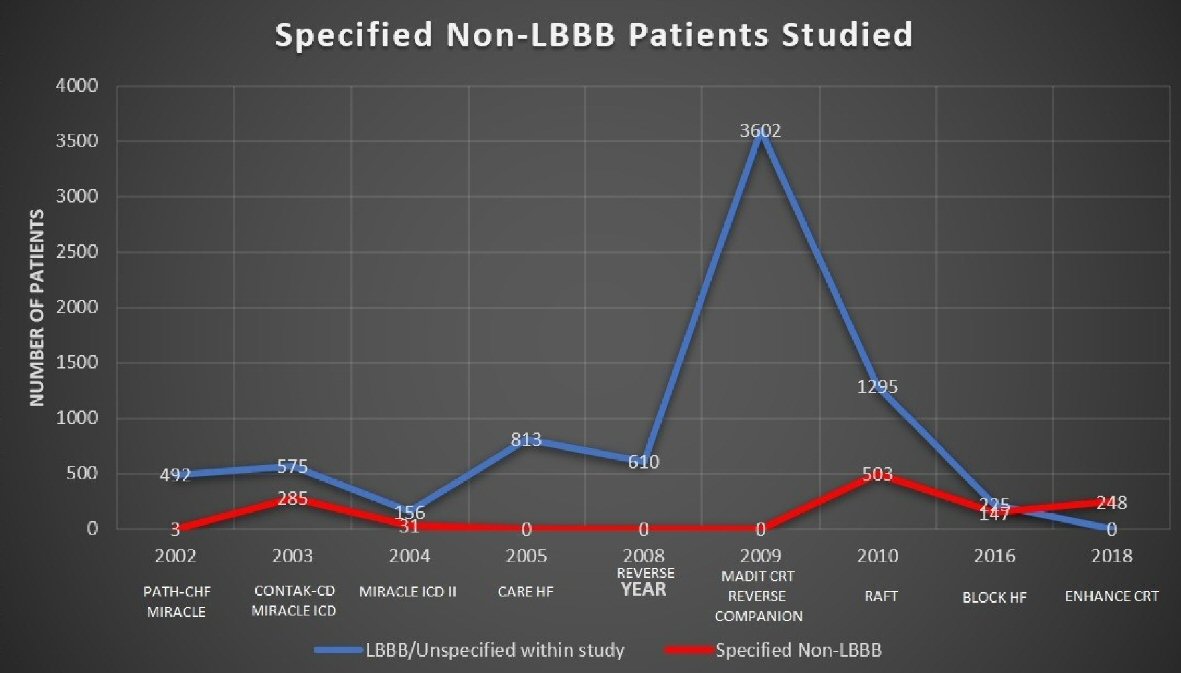
| Path CHF, Auricchio et al, 2002 [13] | Compare the short- and long-term clinical effects of atrial synchronous, pre-excitation of univentricular or biventricular therapy with cardiac CRT. | N = 42; randomized to biventricular CRT (24)/univentricular CRT (17); followed for 9 months | QRS ≥ 120 ms; LBBB, 39 (93%)/ RBBB, 3 (7%) | CRT produces a long-term improvement in the clinical symptoms of patients with HF who have significant IVCD. |
| MIRACLE, Abraham et al, 2002 [14] | Evaluate the clinical benefit of CRT in symptomatic heart failure with IVCD. | N = 453; randomized to CRT group (228)/control (225); followed for 6 months | QRS ≥ 130ms | Significant clinical improvement in moderate to severe heart failure with IVCD. |
| CONTAK CD, Higgins et al, 2003 [15] | Assess the safety and effectiveness of cardiac CRT when combined with an ICD. | N = 490; randomized to CRT (245)/control (245); followed for 6 months | QRS ≥ 120 ms; CRT group: LBBB 50%/NSIVCD 32%/RBBB 18%; non-CRT group: LBBB 54%/NSIVCD 34%/RBBB 12% | CRT implant has improved the functional status in all patients that were indicated for ICD and have HFrEF and IVCD. |
| MIRACLE ICD, Young et al, 2003 [16] | Examine the efficacy and safety of combined CRT and ICD therapy in patients with NYHA class III or IV CHF despite appropriate medical management. | N = 369; randomized to CRT on (187)/ CRT off (182); followed for 6 months | QRS ≥ 130 ms; CRT group: LBBB 87%/RBBB 13%; control group: LBBB 86%/RBBB 14% | CRT improved quality of life, functional status, and exercise capacity in patients with moderate to severe HF, a wide QRS interval, and life-threatening arrhythmias. CRT effect on QOL score and NYHA functional class was not influenced by morphology of the BBB (R vs. L) |
| MIRACLE ICD II, Abraham et al, 2004 [17] | Assess the efficacy and safety of combined CRT and ICD therapy in patients with NYHA class II CHF despite appropriate medical management. | N = 186; randomized to CRT on (86)/control (101); followed for 6 months | QRS ≥ 130 ms; CRT group: LBBB 88%/RBBB 12%; non-CRT group: LBBB 79%/RBBB 21% | Significant improvement in cardiac structure and function over 6 months. CRT did not alter exercise capacity. |
| CARE HF, Cleland et al, 2005 [18] | Evaluation of CRT on morbidity and mortality in patients with NYHA class III or IV. | N = 813; randomized to CRT group (409)/control (404); followed for 18 months | QRS ≥ 120 ms | CRT improves symptoms, the QOL and reduces complications and improves mortality. The broader the QRS in general the overall better results. |
| REVERSE, Linde et al, 2008 [19] | Assess the effects of CRT use in patients with NYHA functional class I and II. | N = 610; randomized to CRT group (419)/control (191); followed for 12 months | QRS ≥ 120 ms | CRT in combination with optimal medical therapy (+/-defibrillator), reduces the risk for HF hospitalization and improves ventricular structure and function in NYHA I and II. |
| MADIT CRT, Breithardt et al, 2009 [20] | Determine whether CRT with biventricular pacing would reduce the risk of death or HF events in patients with NYHA I or II, reduced EF of ≤ 30% and QRS duration ≥ 130 ms. | N = 1,820; randomized to CRT (CRT and ICD on) group (1,089)/control (CRT off and ICD on) (731); followed for up of 2.4 years | QRS ≥ 130 ms; CRT group: LBBB (761)/RBBB (136); control: LBBB (520)/RBBB (92) | CRT combined with ICD decreased the risk of HF events in relatively asymptomatic patients with a low ejection fraction and wide QRS complex. |
| REVERSE, Daubert et al, 2009 [21] | Evaluate the long-term effects of CRT in the European cohort of patients enrolled in the REVERSE trial. | N = 262, randomized to CRT group (ICD activated, CRT on) (180)/control (ICD activated, CRT off) (82); followed for 24 months | QRS ≥ 120 ms | Clinical functional outcomes improved and LV end systolic volume decreased by a greater mean in CRT on than CRT off. First HF hospitalization or death was significantly delayed by CRT (HR: 0.38; P = 0.003). |
| COMPANION, Anand et al, 2009 [22] | Assess the use of CRT as a treatment of CHF on mortality and hospitalization. | N = 1,520; randomized in 1:2:2 ratios for optimal medical management (308)/CRT-p (617)/CRT-d (595); followed for 15 months | QRS ≥ 120 ms | CRT pacing with or without ICD capability was associated with a significant 1-year relative risk reduction of about 20% for all-cause death or hospitalization. |
| RAFT, Tang et al, 2010 [23] | Evaluate whether CRT benefits patients with LV systolic dysfunction and a wide QRS. | N = 1,798; randomized to CRT group (ICD activated, CRT on) (894)/control (ICD activated, CRT off) (904); followed up for 40 months | QRS ≥ 120 ms; CRT group: LBBB72.9%/NIVCD 11.9%/RBBB 7.6%; control group: LBBB71.1%/NIVCD11.2%/RBBB 7.4% | The combined use of CRT with ICD has reduced the mortality and hospitalization for HF patients. |
| BLOCK HF, Curtis et al, 2016 [24] | Assess biventricular pacing against primary end points of reduce mortality, morbidity, and adverse left ventricular remodeling in patients with high grade AV block; and NYHA class I, II, or III; and a LVEF of 50% or less. | N = 691; randomized to Biventricular pacing (349)/ RV pacing (342); followed for 24 months | QRS ≥ 120 ms; biventricular pacing: 1st AV block (68)/2nd AV block (119)/3rd AV block 162/LBBB (123)/RBBB (73); RV pacing: 1st AV block (66)/2nd AV block (108)/3rd AV block (167)/LBBB (102)/RBBB (74) | Biventricular pacing was superior to conventional right ventricular pacing alone in patients with AV block and left ventricular systolic dysfunction with NYHA class I, II, or III HF. |
| ENHANCE CRT, Singh et al, 2018 [25] | Evaluate the effect of a non-traditional LV lead implant strategy on the clinical composite score in a non-LBBB patient population. | N = 248; randomized to QLV implant strategy (161)/standard of care (81); followed up for 12 months | QRS ≥ 120 ms; QLV study arm: IVCD (55)/RBBB (86)/RBBB and LAFB (15)/RBBB and LPFB (2)/others (3); standard of care study arm: IVCD (33)/RBBB (36)/RBBB and LAFB (9)/RBBB and LPFB (1)/others (2) | CRT is an effective therapy in patients with non-LBBB. No apparent variation was documented in responses by subgroups analysis (i.e. RBBB vs. IVCD, QRS interval, sex, HF cause, or LVEF). |