

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Original Article
Volume 11, Number 5, October 2020, pages 337-341
Correlation Between T Peak to End Interval and Left Ventricular Time to Peak Longitudinal Strain in Ischemic Cardiomyopathy Patients
Chaerul Achmada, b, c, Aditya Fahmi Priandaa, Badai Bhatara Tiksnadia, Mohammad Iqbala, Giky Karwikya, Mega Febrianoraa
aDepartment of Cardiology and Vascular Medicine, Hasan Sadikin General Hospital, Universitas Padjajaran, Bandung, Indonesia
bHasna Medika Cardiac Hospital, Cirebon, West Java, Indonesia
cCorresponding Author: Chaerul Achmad, Department of Cardiology and Vascular Medicine, Hasan Sadikin General Hospital, Jalan Eyckman 38, Bandung 40161, Indonesia
Manuscript submitted June 24, 2020, accepted July 2, 2020, published online August 1, 2020
Short title: Relation of Tpe Interval and LV Time to Peak LS
doi: https://doi.org/10.14740/cr1126
| Abstract | ▴Top |
Background: Ischemic cardiomyopathy is the most frequent etiology of heart failure with reduced ejection fraction (HFrEF) and a result of ventricular structural, functional and electrical remodeling. T peak to end (Tpe) interval is an electrocardiographic parameter that represents repolarization heterogeneity and had prognostic value for ventricular arrhythmia. Patients with ischemic cardiomyopathy face a significant burden of arrhythmias. Mechanical dispersion is a functional remodeling parameter that can be measured by time to peak longitudinal strain using speckle tracking echocardiography. This study aimed to assess the relationship between Tpe interval with time to peak longitudinal strain in ischemic cardiomyopathy patients.
Methods: This study was conducted with an observational analytical cross-sectional design. Ischemic cardiomyopathy subjects were included at Dr. Hasan Sadikin General Hospital, Bandung, from August to October 2019. Tpe interval was measured manually with the tangential method. Time to peak longitudinal strain was measured using speckle tracking echocardiography. The correlation between Tpe interval and time to peak longitudinal strain was analyzed using Pearson correlation.
Results: A total of 30 subjects were included in this study. The average age was 58 ± 8 years old, and the average left ventricular ejection fraction was 27±5.5%. The average of Tpe interval was 83.4 ± 7.62 ms, and the average time to peak longitudinal strain was 93.13 ± 34.51 ms. The Pearson correlation test showed a significant weak positive correlation (r = 0.386, 95% confidence interval: 0.029 - 0.743, P = 0.018) between Tpe interval and time to peak longitudinal strain in ischemic cardiomyopathy patients.
Conlucions: There was a significant weak positive correlation between Tpe interval and time to peak longitudinal strain in ischemic cardiomyopathy patients.
Keywords: Ischemic cardiomyopathy; Mechanical dispersion; T peak to end interval; Time to peak longitudinal strain
| Introduction | ▴Top |
Ischemic cardiomyopathy is a condition that depicts myocardial dysfunction caused by obstructive coronary artery disease [1]. It has an increasing prevalence regarding the incidence of coronary artery disease. Prevalence of coronary artery disease in Indonesia has increased from 0.5% in 2013 to 1.5% in 2018 [2]. Ischemic cardiomyopathy has a worse prognosis than non-ischemic cardiomyopathy, with a 5-year survival rate at as high as 50% while non-ischemic cardiomyopathy is 33% [3]. The most common cause of death in ischemic cardiomyopathy is progressivity of heart failure and sudden cardiac death [4]. Ischemic cardiomyopathy is the most frequent etiology of heart failure with reduced ejection fraction (HFrEF) and a result of ventricular structural, functional and electrical remodeling [5]. Ventricular arrhythmia in ischemic cardiomyopathy can be caused by multifactorial etiologies, one of which is related to electrical remodeling of ventricle. Electrical remodeling is the result of ion channel remodeling, disturbed intercellular coupling, altered calcium homeostasis and fibrosis. Electrical remodeling can cause delayed conduction velocity, prolonged potential action duration and increased repolarization heterogeneity [6]. T peak to end (Tpe) interval is an electrocardiographic parameter representing repolarization heterogeneity and had prognostic value for ventricular arrhythmia [7-9].
Advancement of heart failure is related to progressive chamber enlargement and left ventricular dysfunction [5]. Left ventricular dysfunction can be evaluated by mechanical dispersion, which is a functional remodeling parameter measured by time to peak longitudinal strain using speckle tracking echocardiography [10].
To the best of our knowledge, there has not been any study regarding the association between Tpe interval and time to peak longitudinal strain in ischemic cardiomyopathy patients.
| Materials and Methods | ▴Top |
Study design and population
Our study was a cross-sectional study with correlation analysis. Subjects were ischemic cardiomyopathy patients older than 18 years at Hasan Sadikin Hospital from August to October 2018. The exclusion criteria were poor echocardiography window, primary valvular heart disease, congenital heart disease, obesity, unmeasurable Tpe interval, hypertensive heart disease, acute coronary syndrome, cardiac channelopathy, or patients consuming drugs that can affect Tpe interval. A total of 30 patients were included. The study protocol was reviewed and approved by Research Ethics Committee, Faculty of Medicine, Universitas Padjadjaran, Bandung. In this study we did not perform animal study.
Tpe interval and time to peak longitudinal strain
A 12-lead electrocardiogram (ECG) for measurement of Tpe interval was obtained at 50 mm/s and 20 mV calibration. Tpe interval was measured manually with a tangential method using a digital caliper. Tpe interval was measured from the peak to the end of T wave. The echocardiographic examination was done using Vivid T8. Time to peak longitudinal strain was measured using speckle tracking echocardiography.
Statistical analysis
Continuous variables were expressed as mean ± standard deviations or median (range) if data were not distributed normally. The Saphiro-Wilk test was used to assess the normality of data. Categorical data are summarized as frequencies and percentages. Pearson correlation or Spearman as an alternative was used to determine the correlation coefficient. Correlation coefficient was deemed very low, low, moderate, strong and very strong according to r value (0 - 0.199, 0.2 - 0.399, 0.4 - 0.599, 0.6 - 0.799 and 0.8 - 1.0, respectively). Statistical analyses were performed with IBM SPSS, version 25.
| Results | ▴Top |
Patient characteristics
We enrolled 30 patients with an average age of 58 ± 8.5 years with predominant male patients (90%). The most common traditional cardiovascular risk factors in this study were hypertension and smoking in 22 subjects (73.3%). The majority of the patients had a history of acute coronary syndrome (83.3%), with only 16 subjects (53.3%) undergoing angiography. Revascularization was done in 15 subjects, 13 subjects underwent percutaneous coronary intervention (PCI) and two subjects underwent coronary artery bypass grafting (CABG). The average left ventricular ejection fraction was 27±5.5%. Medications given to patients are presented in Table 1.
 Click to view | Table 1. Baseline Characteristics |
Tpe interval and time to peak longitudinal strain
The average of Tpe interval was 83.40 ± 7.62 ms, and the average time to peak longitudinal strain was 93.13 ± 34.51 ms. The correlation was considered weak (r = 0.386, P = 0.018), therefore we concluded that the increased duration of Tpe interval would be accompanied by the increase of time to peak longitudinal strain (Table 2). The scatter plot is presented in Figure 1.
Click to view | Table 2. Tpe Interval and Time to Peak Longitudinal Strain |
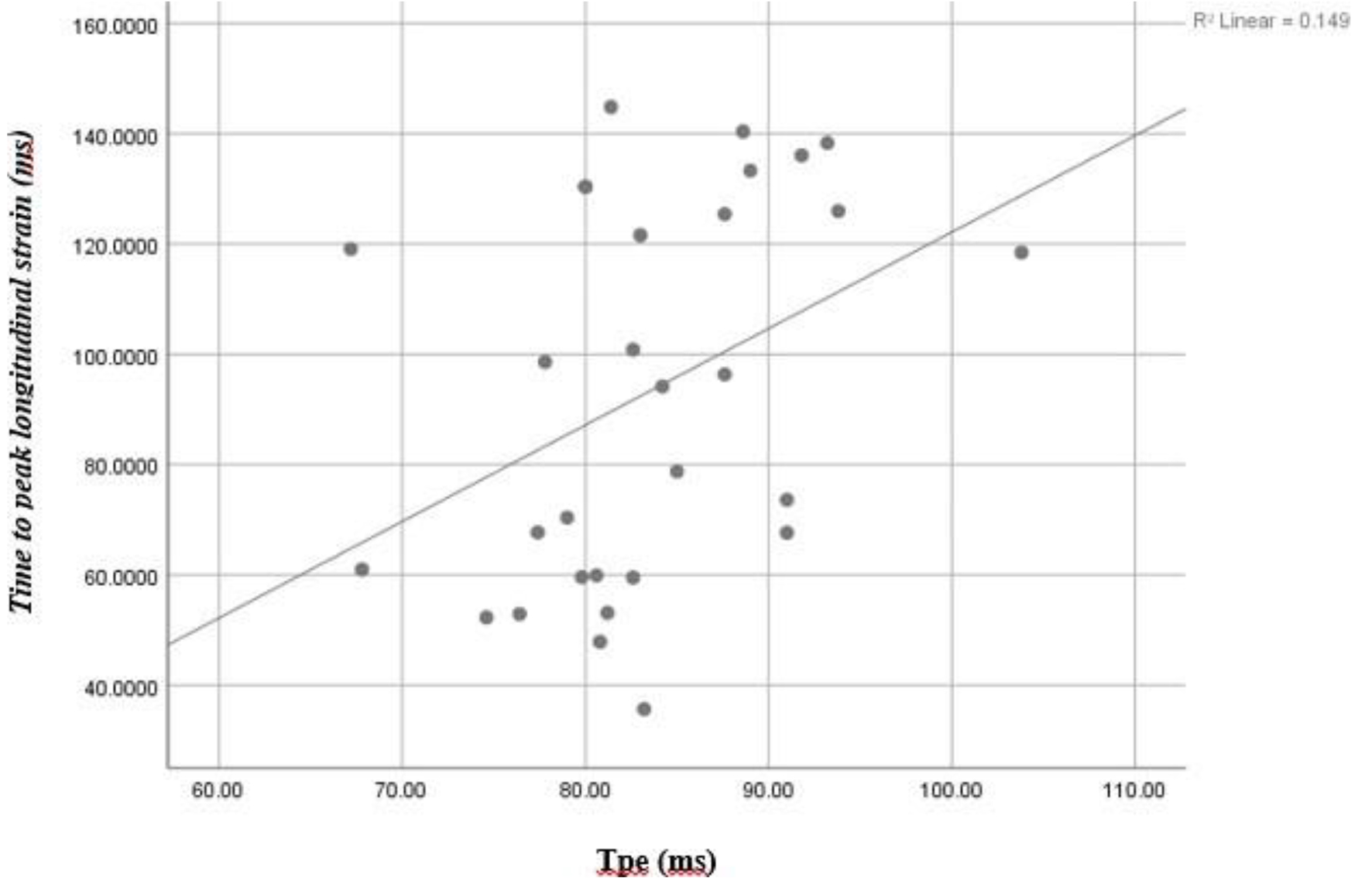 Click for large image | Figure 1. Scatter plot of T peak to end interval and time to peak longitudinal strain. |
| Discussion | ▴Top |
Ischemic cardiomyopathy was caused by structural, functional and electrical remodeling of the ventricle. The most common cause of death in ischemic cardiomyopathy patients was progressivity of heart failure and sudden cardiac death; both were related to the electrical and functional remodeling process [4, 5]. The electrical remodeling, which was assessed by Tpe interval, would also cause heterogeneity of myocardial contraction, which can be assessed by time to peak longitudinal strain [10]. Increasing of Tpe interval has been associated with arrhythmogenesis. The average Tpe interval in this study was 83.4 ± 7.6 ms. The normal range in the general population based on the study was 72.2 ± 9.8 ms, and predictor value for the risk of ventricular arrhythmia was 99.8 ± 27.6. Meanwhile, the range in HFrEF population was 107 ± 22 ms, and predictor value for the risk of ventricular arrhythmia was 106.3 ± 8.4 [11, 12]. The Tpe interval in our subjects was considered high compared to the general population but lower than HFrEF population.
The average time to peak longitudinal strain in this study was 93.13 ± 34.51 ms, consistent with the findings in other studies [13]. However, we did not analyze the effect of anti-remodeling drugs and infarct size, which may influence the time to peak longitudinal strain value. We were not able to analyze anti-remodeling drugs effects on Tpe interval and time to peak longitudinal strain changes because all subjects (100%) were administered with angiotensin converting enzyme (ACE) inhibitors/angiotensin II receptor blockers (ARBs) or angiotensin receptor-neprilysin inhibitors (ARNIs) and 96.7% of subjects with beta blockers.
Our findings showed a weak positive correlation between Tpe interval and time to peak longitudinal strain. The anti-remodeling drugs effects on Tpe interval and time to peak longitudinal strain could be considered as the cause of this weak correlation. However, the studies of anti-remodeling drugs effects on Tpe interval and time to peak longitudinal strain were limited [14, 15].
The R2 coefficient was 0.149, which explains that Tpe interval will influence time to peak longitudinal strain value as high as 14.9%, and the rest of it is influenced by other factors. Those factors would be epicardial fat thickness and genetic factors which were not analyzed in this study [16-18]. This is the first study evaluating the correlation between Tpe interval and time to peak longitudinal strain in ischemic cardiomyopathy patients.
Limitations
Analyses of anti-remodeling drugs effect, fibrosis area size, epicardial fat thickness and genetic factors were not included in this study. Cutoff point of Tpe interval and mechanical dispersion for prediction of ventricular tachyarrhythmia were not provided.
Conclusions
There was a significant weak positive correlation between Tpe interval and time to peak longitudinal strain in ischemic cardiomyopathy patients.
Acknowledgments
None to declare.
Financial Support
None to declare.
Conflict of Interest
None to declare.
Informed Consent
All patients were obtained written informed consent.
Author Contributions
CA and MF made conception and design of study, implemented the study, analyzed and interpreted the study results, drafted the manuscript and revised it. AFP, BBT, MI and GK contributed to the design of study, analysis, and interpretation of study data. They also gave final approval of the version to be published.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
HFrEF: heart failure with reduced ejection fraction; Tpe: T peak to end; ECG: electrocardiogram; CABG: coronary artery bypass grafting; ACE: angiotensin converting enzyme; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor-neprilysin inhibitor
| References | ▴Top |
- Felker GM, Shaw LK, O'Connor CM. A standardized definition of ischemic cardiomyopathy for use in clinical research. J Am Coll Cardiol. 2002;39(2):210-218.
doi - RI K. Riset kesehatan dasar. Indonesia. 2018.
- Gajanana D, Shah M, Junpapart P, Romero-Corral A, Figueredo VM, Bozorgnia B. Mortality in systolic heart failure revisited: Ischemic versus non-ischemic cardiomyopathy. Int J Cardiol. 2016;224:15-17.
doi pubmed - Pons F, Lupon J, Urrutia A, Gonzalez B, Crespo E, Diez C, Cano L, et al. Mortality and cause of death in patients with heart failure: findings at a specialist multidisciplinary heart failure unit. Rev Esp Cardiol. 2010;63(3):303-314.
doi - Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF. Braunwald's heart disease e-book: A textbook of cardiovascular medicine. Elsevier Health Sciences; 2018.
- Coronel R, Wilders R, Verkerk AO, Wiegerinck RF, Benoist D, Bernus O. Electrophysiological changes in heart failure and their implications for arrhythmogenesis. Biochim Biophys Acta. 2013;1832(12):2432-2441.
doi pubmed - Lellouche N, De Diego C, Akopyan G, Boyle NG, Mahajan A, Cesario DA, Wiener I, et al. Changes and predictive value of dispersion of repolarization parameters for appropriate therapy in patients with biventricular implantable cardioverter-defibrillators. Heart Rhythm. 2007;4(10):1274-1283.
doi pubmed - Morin DP, Saad MN, Shams OF, Owen JS, Xue JQ, Abi-Samra FM, Khatib S, et al. Relationships between the T-peak to T-end interval, ventricular tachyarrhythmia, and death in left ventricular systolic dysfunction. Europace. 2012;14(8):1172-1179.
doi pubmed - Rosenthal TM, Stahls PF, 3rd, Abi Samra FM, Bernard ML, Khatib S, Polin GM, Xue JQ, et al. T-peak to T-end interval for prediction of ventricular tachyarrhythmia and mortality in a primary prevention population with systolic cardiomyopathy. Heart Rhythm. 2015;12(8):1789-1797.
doi pubmed - Bleeker GB, Bax JJ, Steendijk P, Schalij MJ, van der Wall EE. Left ventricular dyssynchrony in patients with heart failure: pathophysiology, diagnosis and treatment. Nat Clin Pract Cardiovasc Med. 2006;3(4):213-219.
doi pubmed - Porthan K, Viitasalo M, Toivonen L, Havulinna AS, Jula A, Tikkanen JT, Vaananen H, et al. Predictive value of electrocardiographic T-wave morphology parameters and T-wave peak to T-wave end interval for sudden cardiac death in the general population. Circ Arrhythm Electrophysiol. 2013;6(4):690-696.
doi pubmed - Tse G, Gong M, Wong WT, Georgopoulos S, Letsas KP, Vassiliou VS, Chan YS, et al. The Tpeak - Tend interval as an electrocardiographic risk marker of arrhythmic and mortality outcomes: A systematic review and meta-analysis. Heart Rhythm. 2017;14(8):1131-1137.
doi pubmed - Leong DP, Hoogslag GE, Piers SR, Hoke U, Thijssen J, Marsan NA, Schalij MJ, et al. The relationship between time from myocardial infarction, left ventricular dyssynchrony, and the risk for ventricular arrhythmia: speckle-tracking echocardiographic analysis. J Am Soc Echocardiogr. 2015;28(4):470-477.
doi pubmed - Achmad C, Iqbal M, Karwiky G, Prameswari HS, Febrianora M. T-Peak to T-End improvements after beta-blocker administration in peripartum cardiomyopathy patients. Cardiol Res. 2020;11(3):185-191.
doi pubmed - Collier P, Phelan D, Klein A. A Test in Context: Myocardial Strain Measured by Speckle-Tracking Echocardiography. J Am Coll Cardiol. 2017;69(8):1043-1056.
doi pubmed - Muser D, Tioni C, Shah R, Selvanayagam JB, Nucifora G. Prevalence, correlates, and prognostic relevance of myocardial mechanical dispersion as assessed by feature-tracking cardiac magnetic resonance after a first ST-segment elevation myocardial infarction. Am J Cardiol. 2017;120(4):527-533.
doi pubmed - Kaplan O, Kurtoglu E, Nar G, Yasar E, Gozubuyuk G, Dogan C, Boz AU, et al. Evaluation of Electrocardiographic T-peak to T-end Interval in Subjects with Increased Epicardial Fat Tissue Thickness. Arq Bras Cardiol. 2015;105(6):566-572.
doi pubmed - Marjamaa A, Oikarinen L, Porthan K, Ripatti S, Peloso G, Noseworthy PA, Viitasalo M, et al. A common variant near the KCNJ2 gene is associated with T-peak to T-end interval. Heart Rhythm. 2012;9(7):1099-1103.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.