

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 13, Number 3, June 2022, pages 154-161

Noninvasive Blood Pressure Measurement Using the NICCI Monitor in Adolescents During Intraoperative Anesthetic Care
Kwaku Owusu-Bediakoa, c, Ismail Bekiroglua, Julie Rice-Weimera, Marcelino Murillo-Deluqueza, Joseph D. Tobiasa, b
aDepartment of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA
bDepartment of Anesthesiology & Pain Medicine, The Ohio State University, Columbus, OH, USA
cCorresponding Author: Kwaku Owusu-Bediako, Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH 43205, USA
Manuscript submitted April 4, 2022, accepted May 9, 2022, published online June 2, 2022
Short title: NICCI Monitor in Adolescents
doi: https://doi.org/10.14740/cr1378
| Abstract | ▴Top |
Background: The intermittent measurement of blood pressure (BP) remains the standard of care during anesthesia or procedural sedation. To improve the early identification of hemodynamic compromise, various noninvasive BP devices have been developed which provide a continuous BP reading. The current study evaluates the accuracy of a novel continuous BP device, the NICCI system, in adolescents weighing 40 - 80 kg.
Methods: During intraoperative anesthetic care, BP readings (systolic, diastolic, and mean) were captured from the arterial cannula and the NICCI device every second.
Results: The study cohort included 44 pediatric patients undergoing major orthopedic, cardiac, and neurosurgical procedures. A total of 383,126 pairs of systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial pressure (MAP) values from the arterial cannula and the NICCI device were analyzed. The absolute difference for SBP, DBP, and MAP values from the NICCI monitor and the arterial cannula were 10 ± 8, 9 ± 7, and 9 ± 7 mm Hg, respectively. The difference between the BP values from the NICCI and the arterial cannula was ≤ 10 mm Hg for 60% of the SBP readings, 67% of the DBP readings, and 56% of the MAP readings. Using Bland-Altman analysis, the bias was 2, 3, and 4 mm Hg for the SBP, DBP, and MAP.
Conclusions: Although there were technical limitations related to patient size that affected its ability to meet the strict accuracy criteria set by the American National Standards Institute/Association for the Advancement of Medical Instrumentation standards for noninvasive BP measurement (ANSI/AAMI SP10), the NICCI system provided a continuous noninvasive beat-to-beat BP measurement which was clinically relevant during a significant portion of intraoperative care.
Keywords: Continuous blood pressure monitoring; Invasive arterial pressure; Intraoperative monitoring; Pediatrics anesthesiology
| Introduction | ▴Top |
During anesthetic care, the standard of care mandates that blood pressure (BP) is measured either intermittently using an oscillometric noninvasive blood pressure monitoring (NIBP) device or continuously from an invasive intra-arterial cannula (AC). Evidence suggests that continuous BP monitoring is superior to intermittent NIBP monitoring and may improve outcomes, especially when caring for patients with severe comorbid conditions or during major surgical procedures where blood loss and hemodynamic compromise are expected [1]. It has been estimated that oscillometric NIBP devices, which may provide BP measurements every 3 - 5 min, miss up to 20% of hypotensive episodes, while an additional 20% of these episodes are only detected after a delay [2, 3]. Given the impact of hypotension on end-organ perfusion and postoperative outcomes, inaccuracies in BP readings may increase perioperative morbidity and mortality [3, 4]. Direct arterial cannulation and placement of an AC provide continuous beat-to-beat BP readings, thereby immediately demonstrating BP changes throughout the surgical procedure. However, placement of an AC may be associated with adverse effects, including bleeding, thrombophlebitis, thrombosis, embolism, ischemia, catheter-associated infection, pseudoaneurysm or fistula formation, and nerve injury [5-8].
To address and mitigate these concerns, recent advancements in monitoring technology have led to the development of noninvasive devices that provide continuous beat-to-beat BP readings with a display that resembles that seen with direct arterial cannulation. One such novel device is the NICCI BP device (Getinge/Pulsion Medical Systems, Feldkirchen, Germany) which uses infrared technology to measure BP continuously and display it in a waveform. This observational, single-center study prospectively compared systolic, diastolic, and mean arterial pressure readings from the AC with values obtained from the NICCI noninvasive continuous BP monitor during intraoperative care in adolescent patients weighing 40 - 80 kg.
| Materials and Methods | ▴Top |
The study was approved by the Institutional Review Board of Nationwide Children’s Hospital (Columbus, OH, USA), registered at Clinicaltrials.gov (NCT04373746) and was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration. After obtaining written informed consent from a parent or guardian and assent from patients ≥ 9 years of age, we enrolled patients weighing 40 - 80 kg undergoing various elective orthopedic, neurological, and cardiac surgeries requiring the placement of an AC. Patients with a history of peripheral neurologic disorders, vascular implants at the sites of NIBP measurement, patients in whom an AC could not be placed, and patients with pre-existing edema of the upper extremities were excluded.
The attending pediatric anesthesiologist determined the anesthetic induction and maintenance techniques based on the surgical procedure and the patient’s status. After the induction of anesthesia, an AC was placed in the radial artery. After positioning for the surgical procedure, the NICCI sensor device was attached to the patient, with the calibrating NIBP cuff and finger cuff placed on the side opposite the radial AC (Fig. 1). The suitable size of the finger cuff was chosen according to the finger diameter. The NICCI monitor set-up and subsequent use followed the manufacturer recommendations, with a calibration time of every 30 min. The site of BP monitoring was at the level of the heart. BP readings, including systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial pressure (MAP) were captured onto a laptop from the NICCI device and the AC for subsequent analysis. Data were downloaded from the laptop via ixTrend software to a standard Excel spreadsheet following the surgery. Data were subsequently manually reviewed, and incomplete and erroneous values such as those recorded during blood draw from the AC, AC transducer calibration, and periodic NICCI device calibration were excluded from the analysis.
 Click for large image | Figure 1. The NICCI device with the calibrating noninvasive blood pressure cuff and finger cuffs in place. The inflation of the two finger cuffs is alternated to avoid pressure injury. The external pressure required to maintain blood flow within the fingers is measured using infrared technology which is converted into a continuous waveform on the monitor. |
Statistical analysis
The absolute difference of the SBP, DBP, and MAP values from the AC and NICCI device were calculated. Instead of the directional difference (positive or negative), the absolute difference was used to avoid affecting the data when calculating the mean and standard deviation (SD) of the differences. For instance, if the reading from the NICCI device was 5 mm Hg above or below the reading from the AC, a value of 5 mm Hg was used and not -5 mm Hg or +5 mm Hg. We also calculated the percentage of BP values from the NICCI device that were ≤ 5 mm Hg, ≤ 10 mm Hg, and > 10 mm Hg from the values obtained from the AC. Pearson’s correlation coefficient was used to compare the SBP, DBP, and MAP values between the NICCI device and the AC values. Finally, Bland-Altman plots for repeated measures were used to determine the bias, precision, and 95% level of agreement between the values from the NICCI device and AC. Per standard statistical analysis practice, the actual value (-5 mm Hg or +5 mm Hg) was used to calculate the Bland-Altman analysis and develop a scatterplot of the difference between BP readings from the NICCI device and the AC. The NICCI minus the AC value was plotted on the vertical (y) axis against the average of the two BP readings (NICCI device and AC) on the horizontal (x) axis. Horizontal lines were drawn at the mean difference (blue line) and the 95% limits of agreement (mean difference ± 1.96 × SD) on either side of the mean difference line (red lines). All analyses were conducted using the Statistical Package for the Social Sciences (SPSS) software for Windows, version 26.0. Armonk, New York, IBM Corporation.
| Results | ▴Top |
A total of 50 patients were enrolled in the study, but data from six patients were excluded from the analysis due to a downloading error or defective signal acquisition from the NICCI monitor, which interfered with recording of systolic or diastolic BP readings onto the laptop device. Data from a total of 44 patients (23 females and 21 males) were included in the final analysis. The demographic and clinical characteristics of the study cohort are summarized in Table 1. The mean (SD) age was 15 (2) years, mean (SD) weight was 56 (10) kg, and mean height was 162 (9) cm. Of the 44 patients, 40 were in the prone position, three in the supine position, and one in the lateral position. In all cases, the NICCI finger cuff sensor was placed on the opposite side of the AC. We analyzed a total of 383,126 pairs of SBP, DBP, and MAP values from the NICCI device and the AC. Table 2 summarizes the absolute difference, percentage of values that were ≤ 5 mm Hg, ≤ 10 mm Hg, and more than more than 10 mm Hg from the actual BP value from the AC, and the correlation coefficients between the values. The difference between the BP values from the NICCI device and the AC was ≤ 5 mm Hg for 35% of the SBP readings, 39% of the DBP readings, and 31% of the MAP readings. The difference was ≤ 10 mm Hg for 60% of SBP readings, 67% of the DBP readings, and 56% of the MAP. Further, the difference was > 10 mm Hg for 40% of SBP readings, 33% DBP readings, and 44% of MAP. Pearson’s correlation coefficient comparing the values obtained from the NICCI device with those from the AC showed a strong correlation for all BP readings including 0.60 for SBP, 0.55 for DBP, and 0.59 for MAP. Comparison of blood pressure readings from the AC and the NICCI monitor based on weight is summarized in Table 3. Table 4 summarizes the values for SBP less than or equal to 70 mm Hg versus greater than 70 mm Hg, and MAP less than or equal to 50 mm Hg versus greater than 50 mm Hg for both the AC and NICCI monitor. Table 5 and Figures 2 - 4 display the Bland-Altman analysis with the bias, precision, and 95% limits of agreement between the NICCI device and values from the AC for SBP, DBP, and MAP. The bias and precision were 2 and 13 mm Hg for SBP, 3 and 11 mm Hg for DBP, and 4 and 12 mm Hg for MAP.
 Click to view | Table 1. Demographic and Clinical Characteristics of the Study Cohort |
Click to view | Table 2. Comparison of Blood Pressure Readings From the AC and the NICCI Monitor |
Click to view | Table 3. Comparison of Blood Pressure Readings From the AC and the NICCI Monitor Based on Weight |
Click to view | Table 4. Comparison of SBP and MAP Readings From the AC and NICCI Monitor |
Click to view | Table 5. Bland-Altman Analysis Comparing Blood Pressure Readings From the AC and NICCI Monitor |
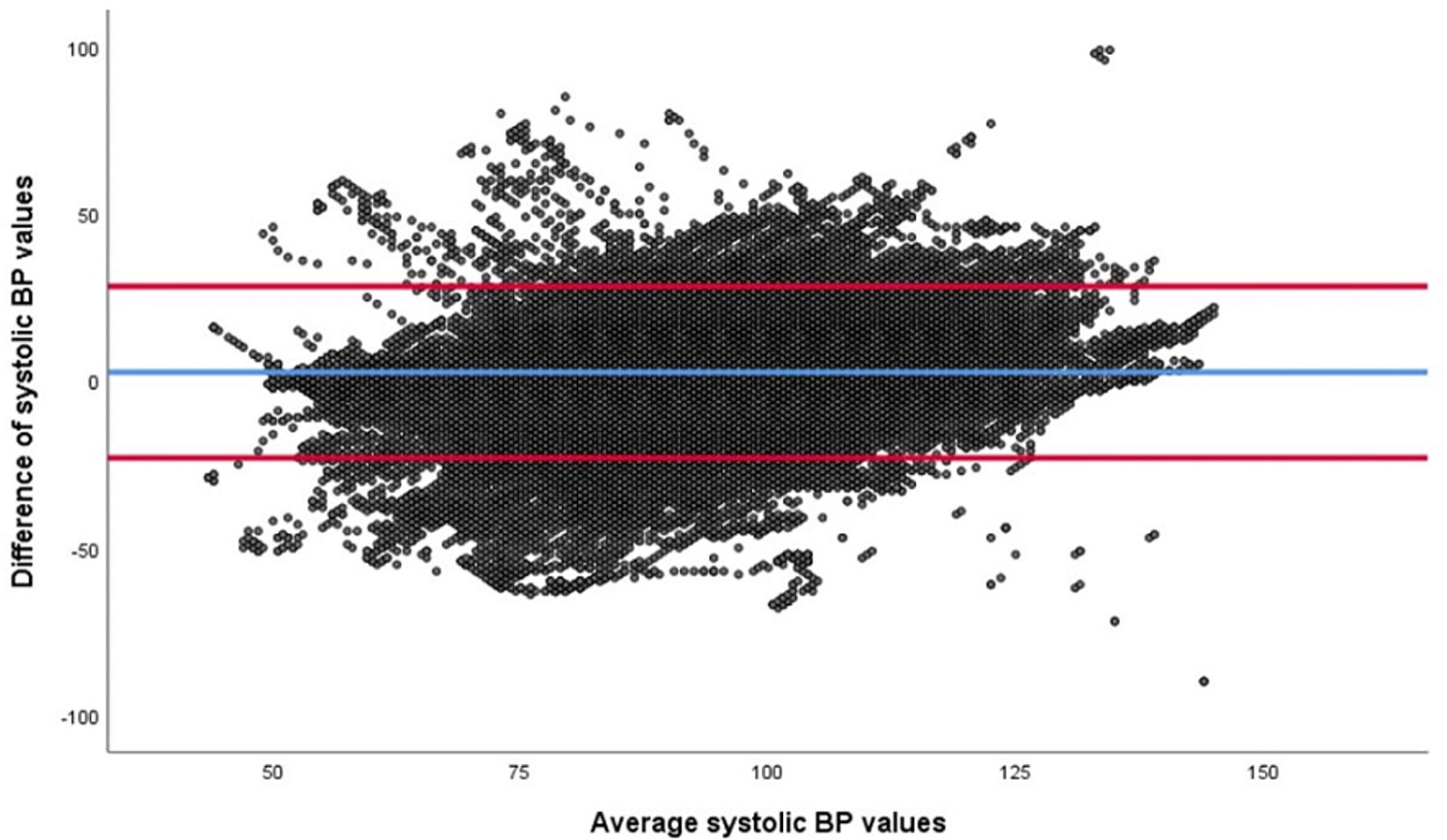 Click for large image | Figure 2. Bland-Altman analysis of the systolic blood pressure (SBP) from the arterial cannula (AC) and the NICCI device, both in mm Hg. The difference between the values (NICCI and AC) are plotted on the vertical axis and the average of the two values on the horizontal access. The red lines demonstrate the 95% limits of agreement (-23 to +31 mm Hg), and the blue line corresponds to the bias (2 mm Hg). BP: blood pressure. |
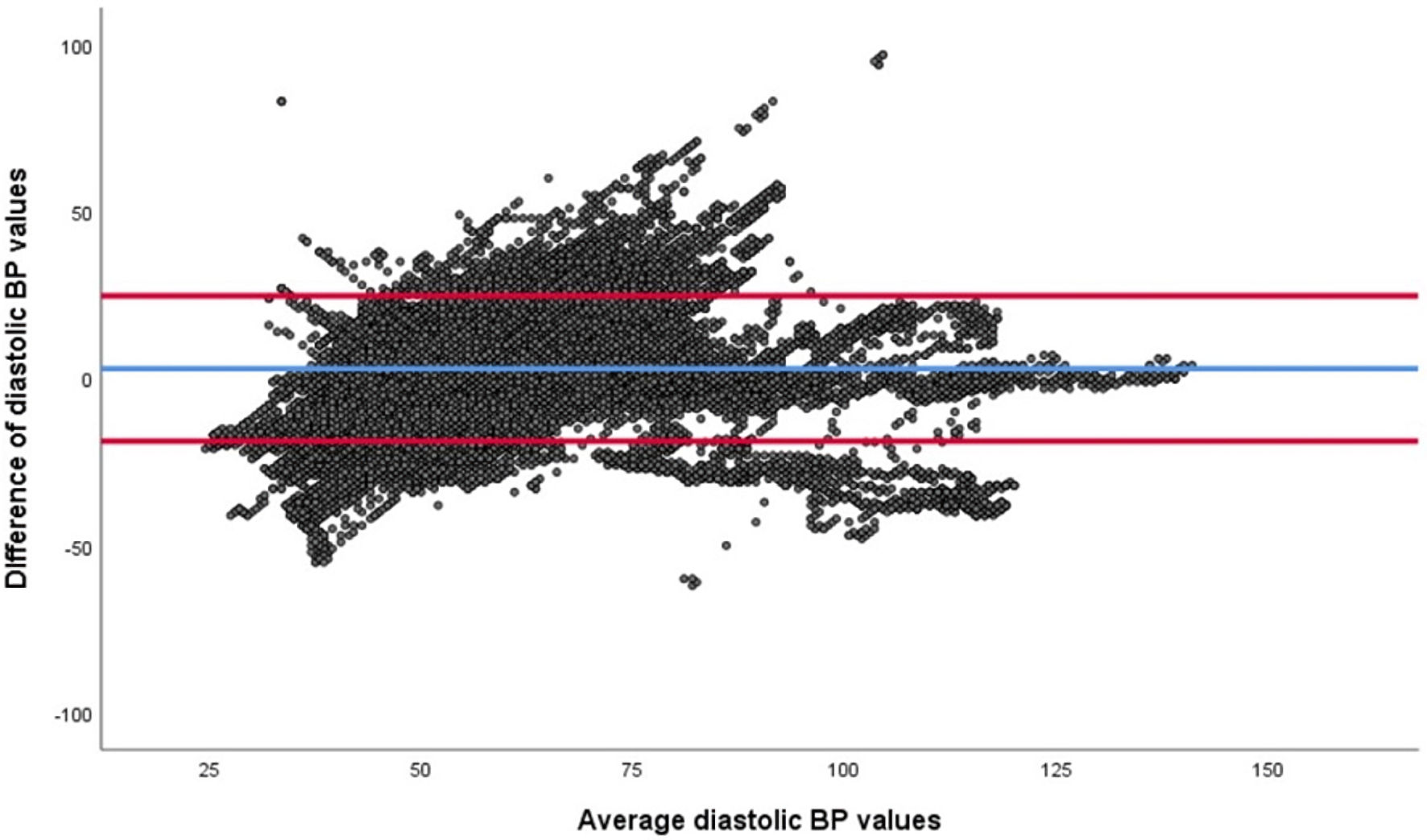 Click for large image | Figure 3. Bland-Altman analysis of the diastolic blood pressure (DBP) from the arterial cannula (AC) and the NICCI device, both in mm Hg. The difference between the values (NICCI and AC) are plotted on the vertical axis and the average of the two values on the horizontal access. The red lines demonstrate the 95% limits of agreement (-19 to +26 mm Hg), and the blue line corresponds to the bias (3 mm Hg). BP: blood pressure. |
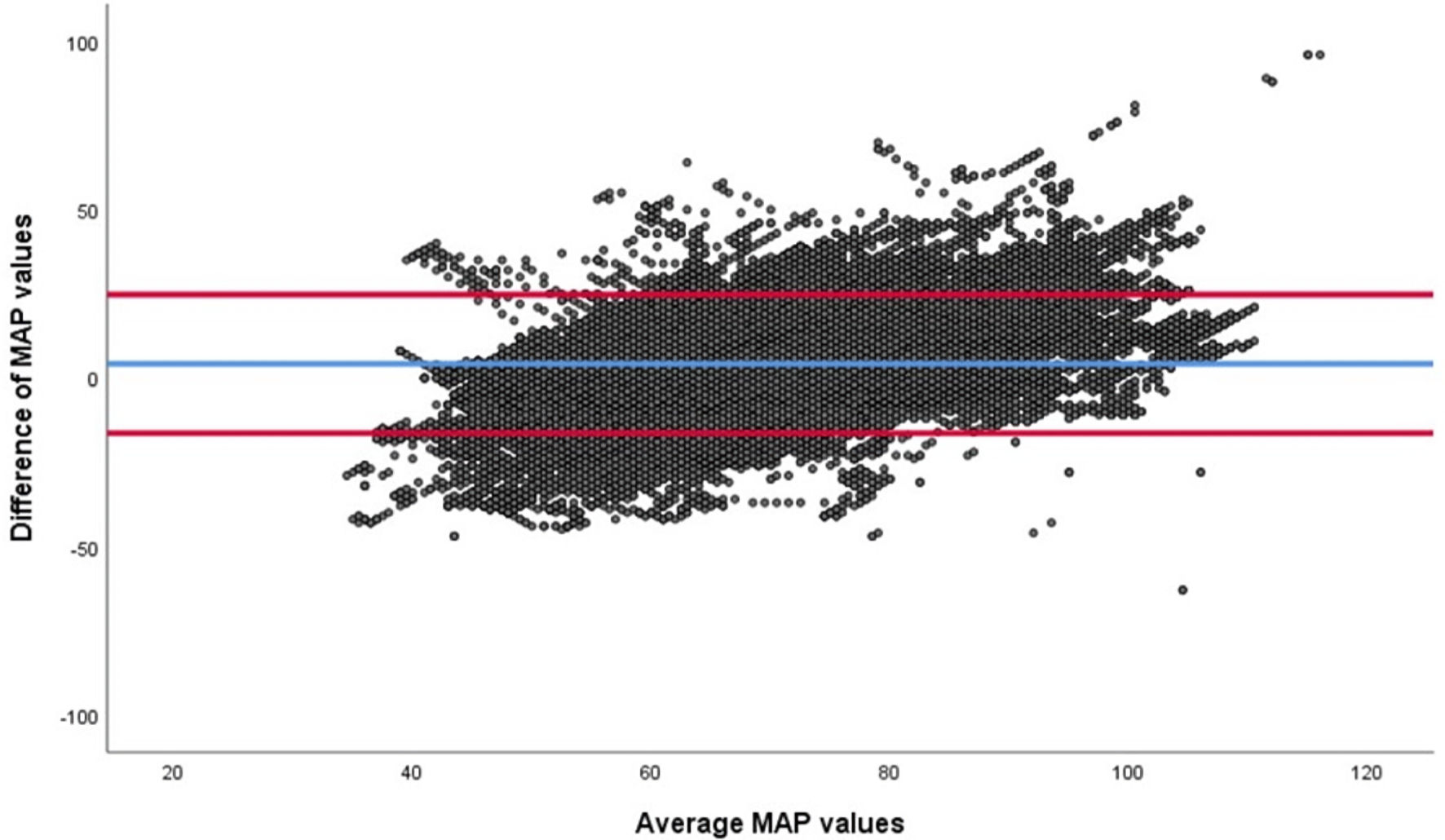 Click for large image | Figure 4. Bland-Altman analysis of the mean arterial pressure (MAP) from the arterial cannula (AC) and the NICCI device, both in mm Hg. The difference between the values (NICCI and AC) are plotted on the vertical axis and the average of the two values on the horizontal access. The red lines demonstrate the 95% limits of agreement (-16 to +25 mm Hg), and the blue line corresponds to the bias (4 mm Hg). |
| Discussion | ▴Top |
We investigated the accuracy and agreement between BP readings from the NICCI device and values obtained from a standard AC in adolescents weighing 40 - 80 kg, who were undergoing various inpatient orthopedic, cardiac, and neurological surgical procedures. To our knowledge, this study is the first to evaluate the performance of the NICCI monitor in the pediatric population. Although there were technical limitations that may have impacted accuracy, the NICCI system provided a continuous noninvasive BP reading within clinically useful parameters, defined as BP readings ≤ 10 mm Hg from the values obtained from the AC, approximately 60% of the time during intraoperative care. The NICCI technology is based on the Continuous Noninvasive Arterial Pressure (CNAP™, CNSystems, Graz, Austria) technology, which was introduced to the market in 2006 [9, 10]. The NICCI device used for this study is a CE version with an investigational device exemption and is not currently available for commercial sale. Various modifications of the NICCI device have included an improved hardware design to facilitate the initial set-up and decrease application time. For example, the design of the novel hand device simulates the design of a standard computer mouse, thereby allowing easier application of the finger cuffs than the previously used wrist mount and double finger cuff system of the CNAP™ monitor. In imitation of the CNAP™ system, the NICCI device uses vascular unloading (volume clamping) technology to provide a continuous beat-to-beat noninvasive measurement of the BP and displays it as a continuous waveform [11, 12]. The absorption of infrared light that is shined through a finger is used to estimate the arterial volume within the vascular bed of the digit. The external pressure in the finger cuff is rapidly adjusted such that the arterial volume is “clamped” or maintained constant throughout the pressure-pulse cycle. Consequently, the cuff pressure waveform closely approximates the intra-arterial pressure waveform measured by a noninvasive BP cuff at the arm. The degree of external pressure required to maintain the intra-arterial volume constant is compared to the noninvasive BP measurement at the arm (brachial artery) and is converted to a beat-to-beat BP waveform displayed on the bedside monitor. Per the Penaz principle, photoplethysmography and closed-loop control of a pneumatic cuff are used to continuously adjust the cuff pressure to track the arterial pressure [13].
The NICCI device uses two-finger cuffs that are available in three different sizes (small, medium, large) with infrared light sensors to measure the counter-pressure required to maintain a stable blood flow and constant intra-arterial volume. The cuffs are placed on the second and third digits and can fit fingers varying in diameter from 13 to 28 mm. Inflation of the two cuffs is alternated to allow continued use of the device while limiting the risk of potential ischemic injury from continuous inflation. Besides continuous BP monitoring, the NICCI monitor can be programmed to measure or calculate other hemodynamic parameters, including pulse rate, cardiac index, stroke volume index, stroke volume variation, pulse pressure variation, systemic vascular resistance, and cardiac power index.
Previous studies have demonstrated a clinically useful correlation of BP readings from the CNAP™ system in adult and pediatric patients in various clinical scenarios, including intraoperative care [3, 8-10, 14-16]. In the current study of patients weighing 40 - 80 kg, the NICCI device provided continuous noninvasive beat-to-beat BP measurements which were within clinically useful limits of values obtained from an AC during a significant portion of the intraoperative anesthetic care. However, the American National Standards Institute/Association for the Advancement of Medical Instrumentation standards for noninvasive BP measurement (ANSI/AAMI SP10) states that a clinically acceptable agreement is met by a mean difference (bias) of ± 5 mm Hg and a SD of 8 mm Hg [17]. Although the data for the current cohort of patients met these criteria for the bias for SBP, DBP, and MAP readings, the SD was well outside the recommended range.
Although the NICCI monitor functioned efficiently throughout the study, we would postulate that several factors may impact the device’s accuracy (especially the ranges or precision noted) and explain why the BP readings did not meet the strict accuracy criteria. Most importantly, for the purposes of the study, the AC was considered the gold standard and the correct measure of BP. Although not evaluated in the current cohort of patients, variations in the accuracy of the AC may result from very high dampening properties of the AC system, which can be caused by occlusion or compression of the catheter, arterial wall contact by the catheter tip, or air bubbles in the tubing system [18]. Furthermore, factors such as lack of or incorrect zero adjustments, wrong transducer position (above or below reference point), a defective transducer, and a very long or elastic tonometry tubing may result in inaccurate BP measurement from the AC [19]. Other factors that may impact the accuracy of the NICCI monitor include non-supine positioning of patients and problems with arm and finger cuffs which are not specifically manufactured for the pediatric population resulting in difficulty in creating effective fit given the varied dimensions and shape of the fingers, and minor positional changes due to movement of the patient or underlying artery in the subcutaneous space. Additionally, the placement of the NICCI monitor on the opposite arm to the AC could affect the accuracy of BP readings due to the inherent BP differences between the left and right arms. Furthermore, the NICCI value is calibrated against the arterial BP values at the brachial artery with the upper arm oscillometric measurements using a cuff placed above the elbow. In contrast, AC values represent arterial pressure values at the radial artery. As the arterial pressure measured varies based on the site along the same extremity, the values obtained from the two different sites may vary. Furthermore, the exposed hand and forearm of the study patients could be susceptible to the lower operating room temperatures compared to the core body temperature, thereby affecting the vascular tone, altering peripheral circulation, and directly affecting the NICCI sensor. The recalibration interval was 30 min according to the default settings of the NICCI device, which may have further impacted its accuracy in measuring BP. We observed that there were BP measurement inaccuracies during and immediately after recalibration of the NICCI monitor until approximately 60 - 120 s post-calibration, during which time the BP readings drift back to a better estimation of the actual BP. The optimal recalibration interval during general anesthesia has not been investigated. Incomplete data sets or erroneous values such as those recorded during AC transducer calibration, blood draws from the AC, and periodic recalibration of the NICC were excluded from the analysis and may have increased the percentage of BP readings ≤ 10 mm Hg of the AC values. In the clinical setting, it may be helpful to have the values flash from the NICCI monitor flash during recalibration periods to alert the clinician of the potential for erroneous values during this time.
As accurate BP measurements play a significant role in managing the anesthetized patient, inaccurate values can lead to inappropriate interventions, significant complications, or even death. MAP serves as an essential parameter in ensuring the perfusion of vital organs, while SBP and DBP readings are used to accurately identify hypertension or hypotension, serving as indicators of changes in peripheral vascular resistance during surgery [20, 21]. When hemodynamic instability can be predicted, and arterial access is possible, intra-arterial BP measurement with placement of an AC remains the gold standard. At this time, a noninvasive device as such as the NICCI cannot replace invasive BP monitoring. The continuous information regarding BP changes provided by the NICCI device may be clinically more relevant and valuable than intermittent BP measurements obtained from an oscillometric device. Additional technological and equipment modifications including modifications in the algorithm to improve accuracy following intermittent monitor recalibration may increase the applicability of this technology in the perioperative arena.
Acknowledgments
None to declare.
Financial Disclosure
The authors have no financial relationships relevant to this article to disclose.
Conflict of Interest
The authors have no conflict of interest relevant to this article to disclose.
Informed Consent
Written informed consent for publication was obtained from all patients.
Author Contributions
Kwaku Owusu-Bediako helped with study design/conduct, patient recruitment, statistical analysis, data interpretation, manuscript preparation and editing. Joseph D. Tobias helped with study design/conduction, patient recruitment, statistical analysis, data interpretation, manuscript preparation and editing. Ismail Bekiroglu helped with study conduct, patient recruitment and manuscript preparation. Marcelino Murillo-Deluquez helped study conduct, patient recruitment and manuscript preparation. Julie Rice-Weimer helped study conduct, patient recruitment and manuscript preparation.
Data Availability
Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
| References | ▴Top |
- Wang Z, Chen G, Lu K, Zhu Y, Chen Y. Investigation of the accuracy of a noninvasive continuous blood pressure device in different age groups and its ability in detecting hypertension and hypotension: an observational study. BMC Anesthesiol. 2019;19(1):223.
doi pubmed - Chen G, Chung E, Meng L, Alexander B, Vu T, Rinehart J, et al. Impact of non invasive and beat-to-beat arterial pressure monitoring on intraoperative hemodynamic management. J Clin Monit Comput. 2012;26(2):133-40.
doi pubmed - Ilies C, Bauer M, Berg P, Rosenberg J, Hedderich J, Bein B, et al. Investigation of the agreement of a continuous non-invasive arterial pressure device in comparison with invasive radial artery measurement. Br J Anaesth. 2012;108(2):202-10.
doi pubmed - Monk TG, Saini V, Weldon BC, Sigl JC. Anesthetic management and one-year mortality after noncardiac surgery. Anesth Analg. 2005;100(1):4-10.
doi pubmed - Weiss BM, Gattiker RI. Complications during and following radial artery cannulation: a prospective study. Intensive Care Med. 1986;12(6):424-8.
doi - Bowdle TA. Complications of invasive monitoring. Anesthesiol Clin North Am. 2002;20(3):571-88.
doi - Slogoff S, Keats AS, Arlund C. On the safety of radial artery cannulation. Anesthesiology. 1983;59(1):42-7.
doi pubmed - Furfaro S, Gauthier M, Lacroix J, Nadeau D, Lafleur L, Mathews S. Arterial catheter-related infections in children. A 1-year cohort analysis. Am J Dis Child. 1991;145(9):1037-43.
doi pubmed - Jeleazcov C, Krajinovic L, Munster T, Birkholz T, Fried R, Schuttler J, et al. Precision and accuracy of a new device (CNAPTM) for continuous non-invasive arterial pressure monitoring: assessment during general anaesthesia. Br J Anaesth. 2010;105(3):264-72.
doi pubmed - Dewhirst E, Corridore M, Klamar J, Beebe A, Rice J, Barry N, et al. Accuracy of the CNAP monitor, a noninvasive continuous blood pressure device, in providing beat-to-beat blood pressure readings in the prone position. J Clin Anesth. 2013;25(4):309-13.
doi pubmed - Kuck K, Baker PD. Perioperative noninvasive blood pressure monitoring. Anesth Analg. 2018;127(2):408-11.
doi pubmed - Geddes L. The direct and indirect measurement of blood pressure. Am Heart J. 1970;80:435-436.
doi - Penaz J, Voigt A, Teichmann W. [Contribution to the continuous indirect blood pressure measurement]. Z Gesamte Inn Med. 1976;31(24):1030-3.
- Wagner JY, Grond J, Fortin J, Negulescu I, Schofthaler M, Saugel B. Continuous noninvasive cardiac output determination using the CNAP system: evaluation of a cardiac output algorithm for the analysis of volume clamp method-derived pulse contour. J Clin Monit Comput. 2016;30(4):487-93.
doi pubmed - Biais M, Vidil L, Roullet S, Masson F, Quinart A, Revel P, et al. Continuous non-invasive arterial pressure measurement: evaluation of CNAP device during vascular surgery. Ann Fr Anesth Reanim. 2010;29(7-8):530-5.
doi pubmed - Tobias JD, McKee C, Herz D, Teich S, Sohner P, Rice J, et al. Accuracy of the CNAP monitor, a noninvasive continuous blood pressure device, in providing beat-to-beat blood pressure measurements during bariatric surgery in severely obese adolescents and young adults. J Anesth. 2014;28(6):861-5.
doi pubmed - ANSI/AAMI. American national standard for manual, electronic, or automated sphygmomanometers. Association for the Advancement of Medical Instrumentation. 2002.
- Saugel B, Dueck R, Wagner JY. Measurement of blood pressure. Best Pract Res Clin Anaesthesiol. 2014;28(4):309-22.
doi pubmed - Lambertz M, Kraft M, Boenick U. [Evaluation of possible measuring errors from overlaying pressure components in invasive blood pressure recording with external transducers]. Biomed Tech (Berl). 1997;42(9):249-55.
doi - Salmasi V, Maheshwari K, Yang D, Mascha EJ, Singh A, Sessler DI, et al. Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: a retrospective cohort analysis. Anesthesiology. 2017;126(1):47-65.
doi pubmed - Tautu OF, Darabont R, Onciul S, Deaconu A, Comanescu I, Andrei RD, et al. New cardiovascular risk factors and their use for an accurate cardiovascular risk assessment in hypertensive patients. Maedica (Bucur). 2014;9(2):127-34.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.