

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Review
Volume 13, Number 3, June 2022, pages 123-127

Cardiovascular Outcomes With an Early Rhythm Control Strategy in Atrial Fibrillation: A Systematic Review
Jaison J. Johna, c, Rafael J. Cabelloa, Jimmy Honga, Mohammed Falukb
aDepartment of Internal Medicine, University of Texas Medical Branch, Galveston, TX 77555, USA
bDivision of Cardiology, University of Texas Medical Branch, Galveston, TX 77555, USA
cCorresponding Author: Jaison J. John, Department of Internal Medicine, University of Texas Medical Branch, Galveston, TX 77555, USA
Manuscript submitted May 24, 2022, accepted June 6, 2022, published online June 16, 2022
Short title: CV Outcomes With an ERC Strategy in AF
doi: https://doi.org/10.14740/cr1399
| Abstract | ▴Top |
In practice, atrial fibrillation (AF) is typically managed by controlling ventricular rate given similar long-term outcomes and a more tolerable drug profile when compared to rhythm control. However, despite treatment via rate control, patients remain at increased risk for cardiovascular complications. This systematic review provides a summary of literature evaluating the effectiveness of early rhythm control (ERC, initiated within 2 years of diagnosis) in AF in reducing cardiovascular complications. A systematic review utilizing the MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews was performed to identify literature evaluating effectiveness of rhythm control strategies and cardiovascular complication reduction rates in ERC. A total of three literature articles meeting the inclusion and exclusion criteria were included for evaluating the benefit of ERC. One of these examined was a trial that directly compared antiarrhythmic drug (AAD) versus catheter ablation (CA) therapy in maintenance of sinus rhythm (SR). This systematic review shows that ERC is associated with a reduction of cardiovascular events in AF patients compared to other treatment strategies.
Keywords: Atrial fibrillation; Early rhythm control; Catheter ablation; Rate control; Antiarrhythmic drug
| Introduction | ▴Top |
Atrial fibrillation (AF) is the most common cardiac arrhythmia [1-5]. With increasing life expectancy, the incidence and prevalence of AF continue to rise with an estimated worldwide prevalence of 46.3 million. In the USA alone, the number of patients diagnosed with AF is expected to increase three-fold by 2050, placing major importance in further optimizing AF management to reduce incidence of AF-related cardiovascular complications [2, 3]. There are four pillars of AF management: risk factor reduction, stroke risk reduction, rate control, and rhythm control. Per current guidelines, rate control, which involves regulating the ventricular rate to maintain hemodynamic stability but allowing the arrhythmia to persist, remains the first-line treatment for AF. Rhythm control, which involves antiarrhythmic drugs (AADs), cardioversion (chemical or electrical), or ablation to maintain sinus rhythm (SR), is considered to be a second-line treatment for AF. When rhythm control is chosen, catheter ablation (CA) for AF is considered as a second-line treatment after failure of at least one AAD or intolerance [5-7]. Regardless of which approach is pursued, both require risk factors and stroke risk reduction evaluation. Despite guideline-based management of AF, patients remain at risk of developing cardiovascular complications such as stroke, heart failure, and acute coronary syndrome with a cardiovascular death rate of approximately 5% per year [2, 3]. Recent studies have challenged the current guidelines regarding the standard of care in AF management and have shown an association between maintenance of SR and improved cardiovascular outcomes in AF compared to standard therapy [5-12]. This may be partly due to the preservation of left atrial structure and function, thereby reducing risk of cardiovascular complications associated with AF [5, 11]. Here we review the literature evaluating the benefits of early rhythm control (ERC) in AF, which involves the initiation of rhythm control treatment within 2 years of diagnosis of AF, and analyze the effectiveness and safety of different rhythm control strategies.
| Methods | ▴Top |
This systematic review was conducted according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement 2020 [13]. MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews from 2017 to 2021 were searched for literature discussing ERC and rhythm management strategies. Keywords included “early rhythm control in atrial fibrillation” and “early diagnosis.” For the purpose of assessing the benefits of ERC, all patients with AF at high risk for cardiovascular complications (CHA2DS2VASc score of ≥ 2) who were managed with rhythm control within 2 years of diagnosis and were followed for at least 1 year were included. Studies excluded in the ERC comparison were those that initiated rhythm control after 2 years and/or provided short-term follow-up. Duplicate studies were excluded as well. In the comparison of rhythm control strategies, a major clinical trial was reviewed.
| Results | ▴Top |
The results obtained from the literature search and study selection process are outlined in the PRISMA flow chart diagram (Fig. 1). A total of 13 non-duplicate articles were retrieved. After applying the outlined inclusion and exclusion criteria, a total of three articles were included in this systematic review. Of the three articles included, two were randomized controlled trials (RCTs), and one was an observational study. The three studies evaluated the difference between rate control and rhythm control in patients diagnosed with AF within 2 years as well as comparison between AAD and CA. The first randomized control trial evaluated was the EAST-AFNET 4 trial. This was a European multicenter study of 2,789 patients with AF diagnosed in the last 1 year, which showed a statistically significant lower rate of the primary outcome examined (cardiovascular death, stroke, etc.) in patients treated with ERC [8]. The second RCT reviewed was the EARLY-AF trial, which was a Canadian multicenter study of 303 patients with AF diagnosed with in the last 2 years. Results of this study showed that those receiving CA had a lower rate of AF recurrence and burden compared to those receiving AAD as measured by an implantable cardiac monitor at 12-month follow-up [6]. The observational study included in this systematic review was a cohort study from South Korea involving 22,635 patients [10]. They found that among those with newly diagnosed AF (< 1 year), those receiving rhythm control had a statistically significant lower rate of primary outcome (cardiovascular death, stroke, etc.). However, in those with AF greater than 1 year prior to initiation of therapy, no significant difference was seen in the rate versus rhythm control groups in terms of primary outcome.
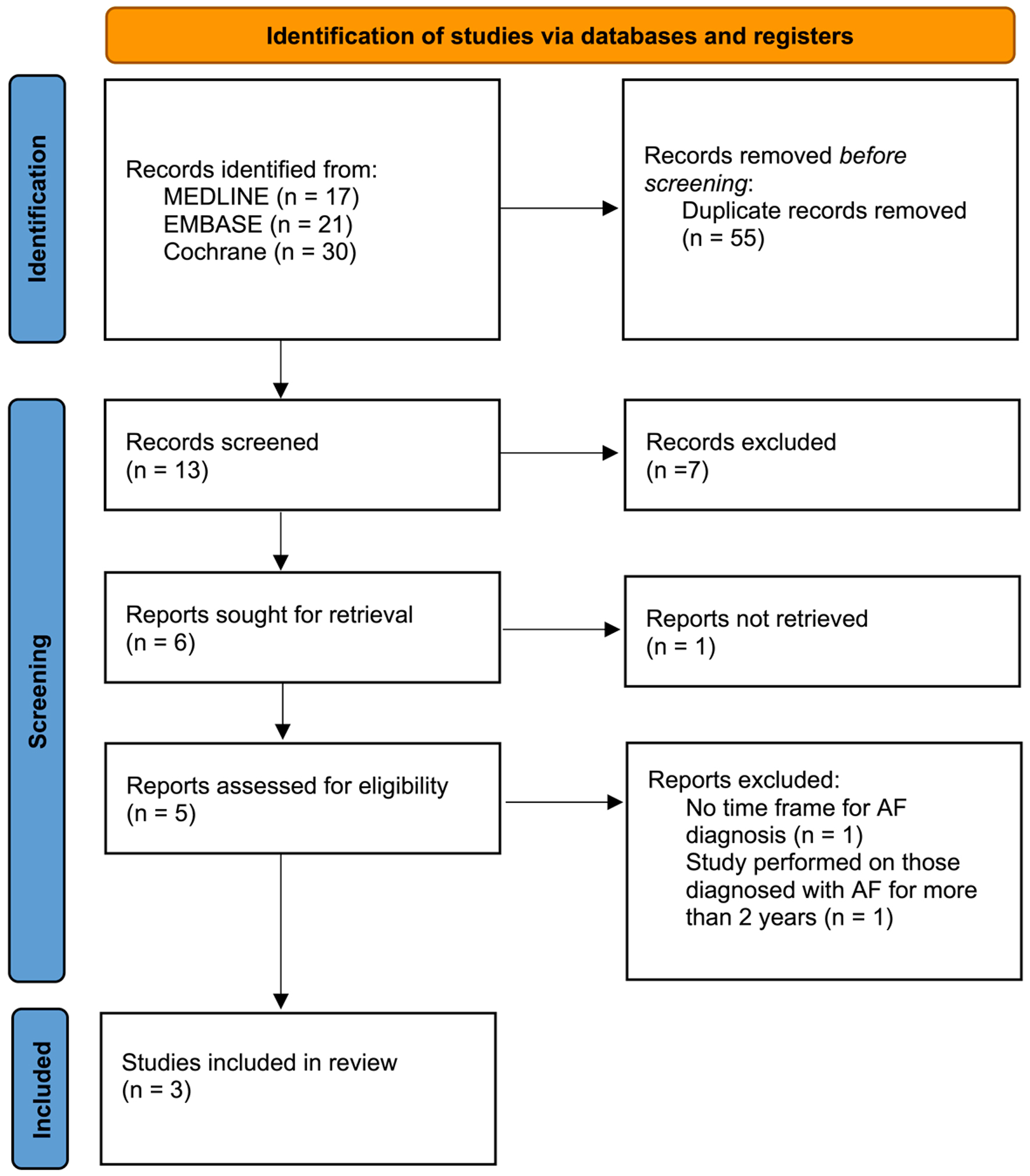 Click for large image | Figure 1. PRISMA flow diagram of study selection process. PRISMA: Preferred Reporting Items for Systematic Review and Meta-Analysis. |
| Discussion | ▴Top |
AF is the most common cardiac arrhythmia, and its prevalence increases with age. Risk factors include age, hypertension, obesity, heart failure, ischemic heart disease, smoking, and alcohol use [14]. For the past 20 years, the guidelines for the management of AF have been shaped by studies such as AFFIRM, which showed no significant difference between rate control and rhythm control when comparing rates of cardiovascular complications [1]. The RACE trial was another landmark study in which rate control was compared to a rhythm control strategy in patients with persistent AF who had undergone a prior cardioversion [15]. Results showed similar primary outcome (cardiovascular death, heart failure, bleeding, thromboembolic events, and adverse reaction to AAD) incidence in the rate and rhythm control groups. Therefore, rate control has been the standard of care in the setting of stable and asymptomatic AF given unchanged long-term outcomes, benign drug profile, cost-effectiveness, and reduced complication rates from multiple failed cardioversion procedures. However, several limitations must be noted from these convention setting trials. In both the AFFIRM and RACE trials, the mean ages in the studies were greater than 65 years, which raises questions on the external validity of these findings to a younger population. In addition, a follow-up analysis to the AFFIRM study showed that the presence of SR was associated with a risk reduction in terms of death; however, the use of AAD to maintain SR was associated with increased adverse events. This posited the idea that if one is able to maintain SR without the use of AAD, this may lead to improved outcomes and decreased cardiovascular deaths in comparison to the prevailing rate control strategy. Since these practice-setting trials, CA for AF has become increasingly utilized. The 2017 expert consensus statement on ablation recognized that CA was a reasonable first-line option for rhythm control in symptomatic AF but was generally recommended after treatment failure with an AAD [16]. A meta-analysis studying the quality of life (QOL), morbidity, and mortality of CA versus AAD in symptomatic AF showed decreased symptoms and improved QOL but no difference in morbidity and mortality in those receiving CA compared to those being treated with AAD [17]. More recently however, the CASTLE-AF trial showed that in those with heart failure with reduced ejection fraction (HFrEF), the CA group had a statistically significant reduction in mortality, AF burden, and increased QOL compared to the drug (rhythm or rate control) group [18].
AF is thought to progress through short paroxysms and can eventually become persistent or permanent. A Canadian registry study of 755 patients showed that greater than 50% of patients diagnosed with paroxysmal AF will progress to persistent AF or be deceased at 10-year follow-up [19]. Observational studies have shown that enlargement and remodeling of the left atrium (LA) is associated with progression of AF. On the microscopic level, changes in ion channels lead to impaired electrical pathways in the atria ultimately leading to fibrosis and scarring. This subsequently leads to left atrial dilation, likely further propagating and forming a substrate for foci of aberrant atrial activity [20]. In fact, recent analysis has shown that even in patients with the same CHA2DS2-VASc score, those with persistent or permanent AF are at a higher risk for stroke than those in paroxysmal AF [21]. These findings may indicate why prior studies like AFFIRM and RACE did not show a statistically significant difference in cardiovascular outcomes between rhythm and rate control. These studies included patients who had been in persistent AF and thus already had significant remodeling of their left atrial structure and electrical system. In contrast, EAST-AFNET 4 selected patients with new-onset AF (< 1 year from time of diagnosis of AF) and showed that those in the ERC group had lower rates of stroke and cardiovascular mortality compared to those in the usual care group. One hypothesis that can explain these findings is that the LA in those receiving ERC had not undergone the same degree of negative remodeling as compared to those in the usual care group. One important caveat, however, is that anticoagulation was continued in those on ERC in the EAST-AFNET 4 trial, but in the AFFIRM trial, anticoagulation was able to be discontinued after 4 weeks of maintaining SR. Although the AFFIRM trial did not show a statistically significant difference between the rhythm and rate control groups in terms of stroke, the incidence of stroke was higher in the rhythm control group (7.1%) versus rate control group (5.5%). This may be explained by the lower rates of anticoagulation in the rhythm control (70%) versus rate control group (85%) [1].
Given paucity in the literature evaluating cardiovascular complications in relation to ERC, an observational study was included in the analysis in conjunction with two RCTs. The observational cohort study by Kim et al showed that there was a statistically significant decreased rate of adverse cardiovascular outcomes in the rhythm control versus rate control group in those with new-onset AF (< 1 year from time of diagnosis of AF) [10]. In those with AF for more than 1 year, no significant difference was found in terms of adverse cardiovascular outcomes when comparing rhythm and rate control groups. These findings of lower adverse cardiovascular outcomes in ERC versus rate control parallel the results of the EAST-AFNET 4 study.
With the emergence of CA as an increasingly used tool for symptomatic AF, trials have shown improvement in mortality and QOL in those with HFrEF [18]. These findings were not seen in the larger general population in the CABANA trial, which showed that those receiving CA did not have a statistically significant mortality benefit or reduction in cardiovascular events as compared to those receiving AAD [22]. However, one factor that may partially explain the findings of this study is that a high number of patients crossed over into the CA arm from the drug treatment arm, which can confound the intention-to-treat analysis.
Building off the findings of EAST-AFNET 4, EARLY-AF showed that early CA with cryotherapy was superior to AAD in terms of preventing recurrence of atrial tachycardias in patients who were diagnosed with AF within the last 24 months [6]. As discussed earlier, AF is a progressive disease. The findings in EARLY-AF and EAST-AFNET 4 seem to indicate that intervention early in the disease course can lead to improved cardiovascular outcomes by halting pathologic and deleterious remodeling of the LA. In addition, the ATTEST trial, which showed that radiofrequency CA was superior to AAD in delaying the progression of paroxysmal AF to persistent AF at 3-year follow-up, gives further credence to the emerging role of CA [23]. It is important to note, however, that EARLY-AF study did not have the power to deduce if early CA would lead to decreased cardiovascular mortality as compared to AAD. However, it can be postulated given the findings of decreased AF burden with early CA and the aforementioned discussions. The STOP-AF trial, similar to the EARLY-AF trial, showed that cryotherapy was superior to AAD at preventing AF recurrence. This trial, however, importantly showed that cryoablation as a first-line treatment for AF was similar in safety profile to AAD [7].
In the EARLY-AF trial, the only modality of CA used was cryotherapy, thus limiting extrapolation of the results to other methods of CA. In the earlier FIRE AND ICE trial, the two most common methods of CA were compared against each other for AF in those who failed AAD therapy: radiofrequency ablation and cryoablation [24]. Results at follow-up showed that cryoablation was non-inferior to radiofrequency ablation in terms of efficacy at preventing AF recurrence with no statistically significant difference between the two groups in terms of complications or adverse events. These results are further seen in the CIRCA-DOSE trial, which showed no significant difference between cryoablation and radiofrequency ablation in terms of efficacy at 1 year as measured by AF recurrence [25]. In summary, the aforementioned trials challenge the current standard of care as established by the AFFIRM trial. ERC by CA is crucial to delay the progression of paroxysmal AF to persistent AF, thereby leading to decreased rates of adverse cardiovascular outcomes as compared to rate control.
| Conclusions | ▴Top |
This systematic review shows that an ERC strategy leads to decreased cardiovascular events when compared to rate control. In addition, CA may be considered as a first-line strategy for rhythm control; however, large randomized clinical trials are needed for further evaluation.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
All authors declare no conflict of interest.
Author Contributions
Jaison J. John: results, discussion, reviewing and editing. Rafael J. Cabello: abstract, introduction and conceptualization. Jimmy Hong: discussion, reviewing and editing. Mohammed Faluk: conceptualization, reviewing, expert opinion and editing.
Data Availability
The data supporting this review article are available within the article.
Abbreviations
AF: atrial fibrillation; ERC: early rhythm control; AAD: antiarrhythmic drug; CA: catheter ablation; SR: sinus rhythm; RCT: randomized controlled trial; QOL: quality of life; HFrEF: heart failure with reduced ejection fraction; LA: left atrium
| References | ▴Top |
- Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347(23):1825-1833.
doi pubmed - Kornej J, Borschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. 2020;127(1):4-20.
doi pubmed - Ionescu-Ittu R, Abrahamowicz M, Jackevicius CA, Essebag V, Eisenberg MJ, Wynant W, Richard H, et al. Comparative effectiveness of rhythm control vs rate control drug treatment effect on mortality in patients with atrial fibrillation. Arch Intern Med. 2012;172(13):997-1004.
doi pubmed - Kotalczyk A, Ding WY, Gupta D, Wright DJ, Lip GYH. Clinical outcomes following rhythm control for atrial fibrillation: is early better? Expert Rev Cardiovasc Ther. 2021;19(4):277-287.
doi pubmed - Grosu AI, Radulescu D, Grosu LC, Pop D. Remodelling in atrial fibrillation: the impact of amiodarone. Cardiovasc J Afr. 2019;30(3):174-180.
doi pubmed - Andrade JG, Wells GA, Deyell MW, Bennett M, Essebag V, Champagne J, Roux JF, et al. Cryoablation or drug therapy for initial treatment of atrial fibrillation. N Engl J Med. 2021;384(4):305-315.
doi pubmed - Wazni OM, Dandamudi G, Sood N, Hoyt R, Tyler J, Durrani S, Niebauer M, et al. Cryoballoon ablation as initial therapy for atrial fibrillation. N Engl J Med. 2021;384(4):316-324.
doi pubmed - Kirchhof P, Camm AJ, Goette A, Brandes A, Eckardt L, Elvan A, Fetsch T, et al. Early rhythm-control therapy in patients with atrial fibrillation. N Engl J Med. 2020;383(14):1305-1316.
doi pubmed - Corley SD, Epstein AE, DiMarco JP, Domanski MJ, Geller N, Greene HL, Josephson RA, et al. Relationships between sinus rhythm, treatment, and survival in the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Study. Circulation. 2004;109(12):1509-1513.
doi pubmed - Kim D, Yang PS, You SC, Sung JH, Jang E, Yu HT, Kim TH, et al. Treatment timing and the effects of rhythm control strategy in patients with atrial fibrillation: nationwide cohort study. BMJ. 2021;373:n991.
doi pubmed - Kirchhof P, Breithardt G, Camm AJ, Crijns HJ, Kuck KH, Vardas P, Wegscheider K. Improving outcomes in patients with atrial fibrillation: rationale and design of the Early treatment of Atrial fibrillation for Stroke prevention Trial. Am Heart J. 2013;166(3):442-448.
doi pubmed - Van Gelder IC, Haegeli LM, Brandes A, Heidbuchel H, Aliot E, Kautzner J, Szumowski L, et al. Rationale and current perspective for early rhythm control therapy in atrial fibrillation. Europace. 2011;13(11):1517-1525.
doi pubmed - Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178-189.
doi pubmed - Benjamin EJ, Levy D, Vaziri SM, D'Agostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA. 1994;271(11):840-844.
doi pubmed - Van Gelder IC, Hagens VE, Bosker HA, Kingma JH, Kamp O, Kingma T, Said SA, et al. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N Engl J Med. 2002;347(23):1834-1840.
doi pubmed - Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, Akar JG, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: Executive summary. Heart Rhythm. 2017;14(10):e445-e494.
doi pubmed - Siontis KC, Ioannidis JPA, Katritsis GD, Noseworthy PA, Packer DL, Hummel JD, Jais P, et al. Radiofrequency ablation versus antiarrhythmic drug therapy for atrial fibrillation: meta-analysis of quality of life, morbidity, and mortality. JACC Clin Electrophysiol. 2016;2(2):170-180.
doi pubmed - Marrouche NF, Brachmann J, Andresen D, Siebels J, Boersma L, Jordaens L, Merkely B, et al. Catheter ablation for atrial fibrillation with heart failure. N Engl J Med. 2018;378(5):417-427.
doi pubmed - Padfield GJ, Steinberg C, Swampillai J, Qian H, Connolly SJ, Dorian P, Green MS, et al. Progression of paroxysmal to persistent atrial fibrillation: 10-year follow-up in the Canadian Registry of Atrial Fibrillation. Heart Rhythm. 2017;14(6):801-807.
doi pubmed - Wijesurendra RS, Casadei B. Mechanisms of atrial fibrillation. Heart. 2019;105(24):1860-1867.
doi pubmed - Vanassche T, Lauw MN, Eikelboom JW, Healey JS, Hart RG, Alings M, Avezum A, et al. Risk of ischaemic stroke according to pattern of atrial fibrillation: analysis of 6563 aspirin-treated patients in ACTIVE-A and AVERROES. Eur Heart J. 2015;36(5):281-287a.
doi pubmed - Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Poole JE, Noseworthy PA, et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. 2019;321(13):1261-1274.
doi pubmed - Kuck KH, Lebedev DS, Mikhaylov EN, Romanov A, Geller L, Kalejs O, Neumann T, et al. Catheter ablation or medical therapy to delay progression of atrial fibrillation: the randomized controlled atrial fibrillation progression trial (ATTEST). Europace. 2021;23(3):362-369.
doi pubmed - Kuck KH, Brugada J, Furnkranz A, Metzner A, Ouyang F, Chun KR, Elvan A, et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med. 2016;374(23):2235-2245.
doi pubmed - Andrade JG, Champagne J, Dubuc M, Deyell MW, Verma A, Macle L, Leong-Sit P, et al. Cryoballoon or radiofrequency ablation for atrial fibrillation assessed by continuous monitoring: a randomized clinical trial. Circulation. 2019;140(22):1779-1788.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.