

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 14, Number 5, October 2023, pages 334-341

Temporal Trends in the United States Patent Landscape: Innovation in Cardiology Across Industry and Academia
Raoul R. Wadhwaa, Brenna M. McElderryb, James Yuc, Samir R. Kapadiaa, d, A. Marc Gillinova, d, Lars G. Svenssona, d, Milind Y. Desaia, d, e
aCleveland Clinic Lerner College of Medicine, Case Western Reserve University, Cleveland, OH 44195, USA
bDepartment of Internal Medicine, Cleveland Clinic, OH 44195, USA
cSchool of Medicine, Case Western Reserve University, Cleveland, OH 44195, USA
dHeart, Vascular & Thoracic Institute, Cleveland Clinic, Cleveland, OH 44195, USA
eCorresponding Author: Milind Y. Desai, Department of Cardiovascular Medicine, Heart, Vascular & Thoracic Institute, Cleveland Clinic, Cleveland, OH 44195, USA
Manuscript submitted February 5, 2023, accepted June 6, 2023, published online October 21, 2023
Short title: Temporal Trends in the US Patent Landscape
doi: https://doi.org/10.14740/cr1417
| Abstract | ▴Top |
Background: Novel approaches to diagnostics and therapeutics in medical care reflect the scientific community’s evolving understanding of disease states and their clinical implications. Marketable and valuable innovations are generally patented for protection of intellectual property. Here, we explore the landscape of cardiology-related patents in the United States.
Methods: All United States patents granted between 2005 and 2020 were included in this study. Keywords filtering was used to identify patents related to cardiovascular medicine. Statistical inference was conducted with the Mann-Kendall trend and analysis of variance tests. The results in this report are entirely reproducible with Python and R scripts available in a publicly accessible repository.
Results: Of the 4,453,733 patents issued by the USPTO between 2005 and 2020, 31,048 (0.7%) were identified as cardiology-related patents. We identified the top 10 institutions within the for-profit and not-for-profit categories that were assigned the most cardiology-related patents in this time period. Distributions of number of patents per inventor were heavily right-skewed, with a small number of inventors responsible for a large number of patents each. Patents in the cardiac imaging subgroup took the longest to gain approval after submission (median delay: 3.6 years).
Conclusions: By studying the patent universe, we are able to identify underexplored areas within cardiovascular medicine. Obstacles such as long delays between patent application and approval can hamper innovation within a field. As a next step, we aim to use these results to predict the next area within cardiovascular medicine to undergo explosive research and innovation.
Keywords: Patent; Cardiology; Innovation; Temporal trends
| Introduction | ▴Top |
Medical innovation is undoubtedly central to the treatment of disease [1, 2]. Novel approaches to diagnostics and therapeutics in medical care reflect the scientific community’s evolving understanding of disease states and their clinical implications [1-3]. As individual knowledge results in new medical ideas, academic institutions and corporations serve as a vessel to test its ability to improve health in a person who is sick [1, 4]. Once a medical technology/treatment is determined to provide substantial benefit, it is typically distributed to the medical community while still preserving the integrity of ingenuity with a patent [5, 6]. Patent applications and issuances precede implementation of new therapies, providing a glimpse into the medical community’s coming advancements in patient care [6].
While using patents as a proxy for innovation may undermine the importance of fundamental science and technology research, one can appreciate that patents reflect analyzing basic science for clinical applications [4]. Studying trends in patent development in particular fields of medicine, such as cardiology, can provide insight into our growing understanding of specific diseases states. In addition, measuring the growth of medical knowledge in the form of patent issuance at particular centers can help identify “hot spots” for innovation [4, 7]. This can lead to opportunities for intellectual partnership between universities and/or industries [4, 7].
This study analyzes United States patent issuance trends within the field of cardiology between 2005 and 2020. We use the framework that medical patents serve as a measure of innovation in clinical practice [1-4]. In addition to studying temporal trends of patents within subgroups of cardiology, we identify which individuals, corporate institutions, and academic institutions have led innovation in recent years.
| Materials and Methods | ▴Top |
The patentpy and pandas packages in the Python programming language were used to acquire patent data from the United States Patent and Trademark Office [8-10]. A list of keywords was generated to identify patents related to cardiovascular medicine, with sub-lists of keywords generated to identify patents within subgroups of cardiology (Supplementary Material 1, www.cardiologyres.org). Keyword search of titles and claims text from all patents issued in the United States from 2005 to 2020 was used to identify cardiology-related patents. One hundred patents were randomly selected and manually evaluated to determine whether they were related to cardiology (Supplementary Material 2, www.cardiologyres.org).
This study did not involve human or animal subjects; as such, it was exempt from IRB approval. The R programming language and the cowplot, gridExtra, lubridate, magrittr, tidyverse, and trend packages were used for data manipulation and subsequent visualization [11-17]. Statistical inference was conducted with the Mann-Kendall (MK) trend test [18, 19] and analysis of variance (ANOVA) [20]. All statistical tests used a two-sided alpha of 0.05. The results in this report are entirely reproducible with Python and R scripts available in a code repository [21].
| Results | ▴Top |
Of the 4,453,733 patents issued by the USPTO between 2005 and 2020, 31,048 (0.7%) were identified as cardiology-related patents. The absolute number of cardiology-related patents issued annually grew over time (Table 1; M-K test: z = 3.92; P < 0.001). After normalizing by the total number of patents issued annually, this pattern flattened (Fig. 1). Due to the breadth of clinical cardiology, patents were split into the following subgroups: aortic; electrophysiology; heart failure; imaging; infectious; interventional; oncology; surgical; valvular; and vascular. These categories were overlapping; for example, patents for surgical devices aimed at treating aortic dissection would be included in the aortic, surgical, and vascular subgroups. Within each of these subgroups, patents issued annually grew between 2005 and 2020 (Table 2), with the temporal trends of absolute patent counts visualized in Figure 2.
 Click to view | Table 1. Number of Patents Related to Cardiology That Were Issued Annually Between 2005 and 2020, Inclusive |
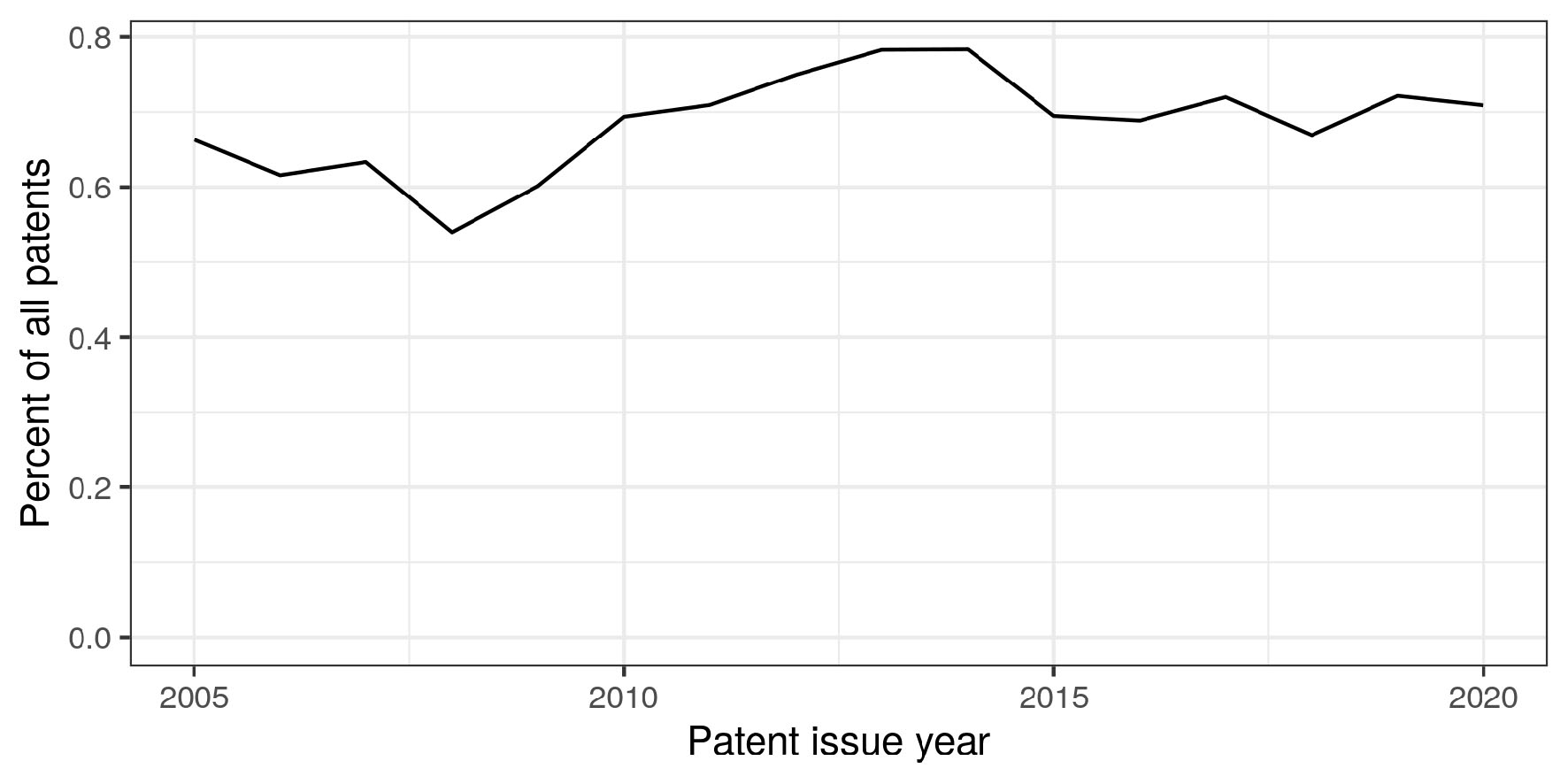 Click for large image | Figure 1. Cardiology-related patents issued between 2005 and 2020 as a percentage of all patents granted. Only patents issued within the United States are included in calculations. Horizontal axis: year in which a patent was issued; vertical axis: percent of issued patents that were related to cardiology. |
Click to view | Table 2. Temporal Trends for Growth in Number of Patents Issued Annually Within Each Subgroup in Cardiology |
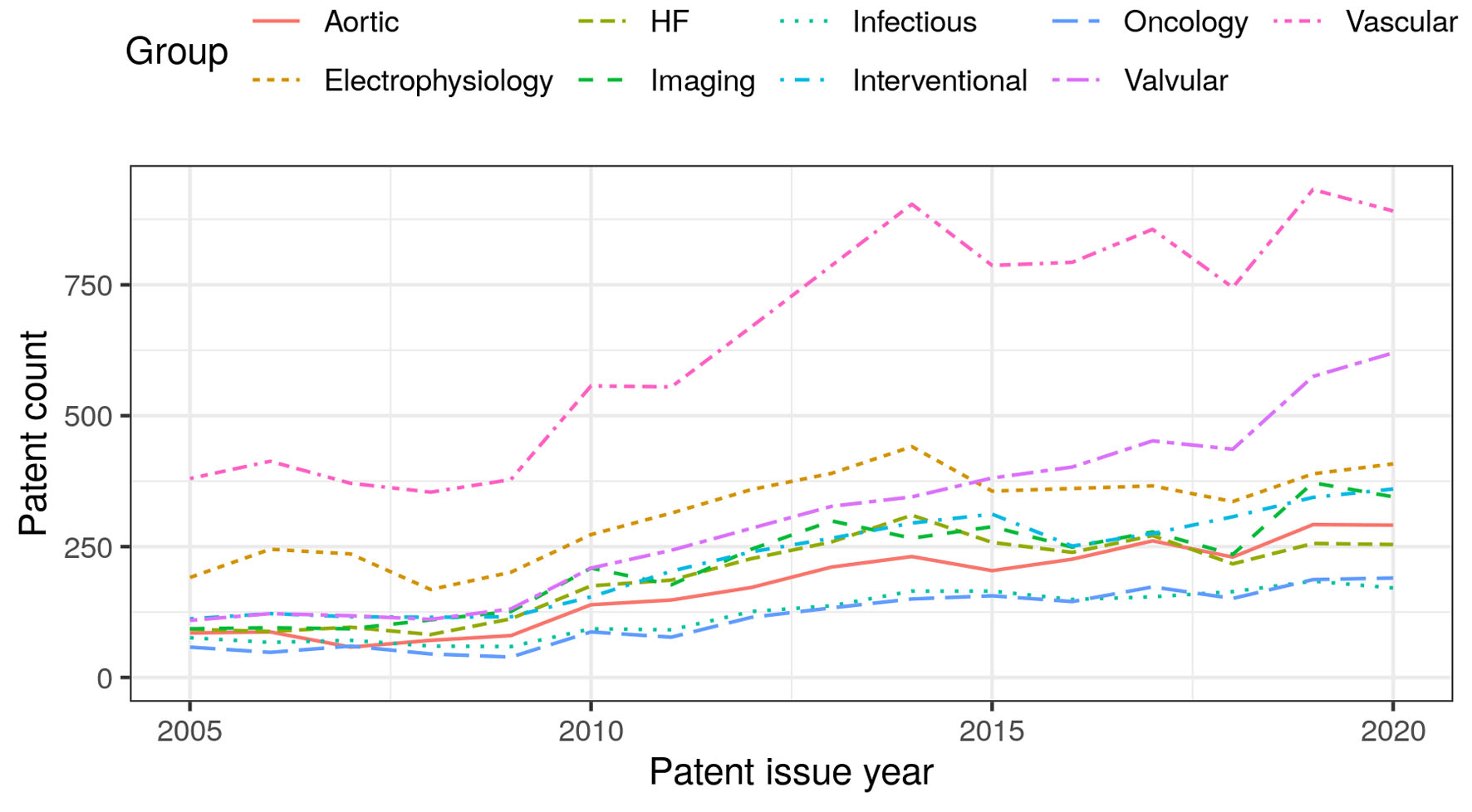 Click for large image | Figure 2. Stratified temporal trends of the number of cardiology-related patents issued annually. Horizontal axis: year in which a patent was issued; vertical axis: number of patents issued in a year within the corresponding subgroup. |
Within patent metadata, USPTO lists inventors, comprised of individuals credited with creating the innovation, and assignees, comprised of institutions that have at least partial ownership of the innovation. The institutions to which patents are assigned can be split into two major groups: 1) corporate, usually for-profit, institutions and 2) academic, usually not-for-profit, institutions. The 10 institutions of each group that have at least partial ownership in the highest number of cardiology-related patents are listed in Table 3. Also notable are patents upon which cardiology-related patents rely the most; the 10 most cited patents between 2005 and 2020 are listed in Table 4.
Click to view | Table 3. Institutions Assigned the Most Cardiology Patents Between 2005 and 2020 |
Click to view | Table 4. The Patents Most Cited By Cardiology-Related Patents Issued Between 2005 and 2020 |
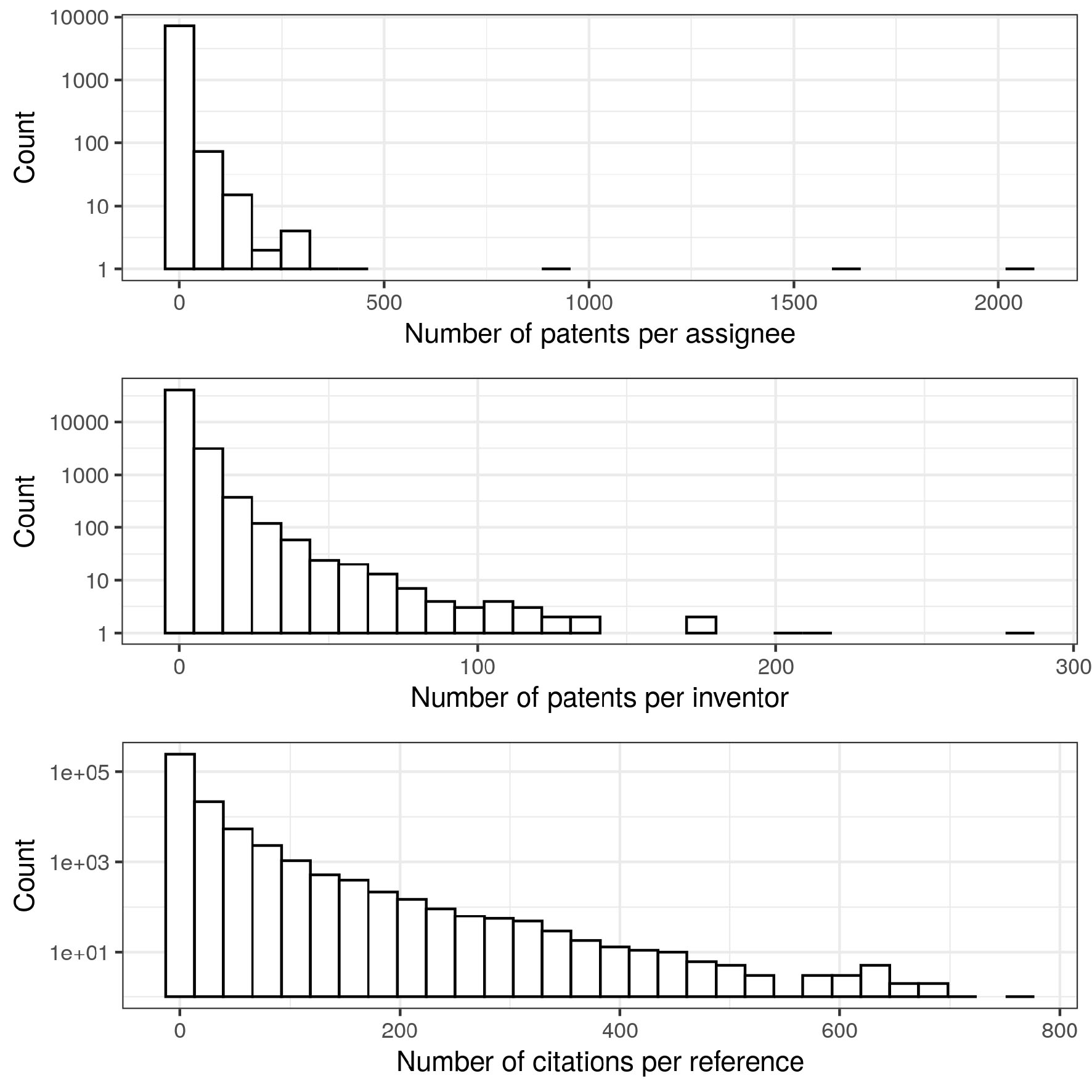
The distributions describing the number of patents belonging to each assignee and inventor were both heavily right-skewed (Fig. 3; upper and central panels, respectively). This pattern of many assignees and inventors having a small number of patents, while a small number had many patents, was repeated in the case of patent citations. Much like peer-reviewed journal articles, newly granted patents cite previously granted patents. Like the prior two distributions, the citation distribution was also right-skewed (Fig. 3; lower panel), showing that many patents were only cited a few times, while a small minority of patents were cited many times.
 Click for large image | Figure 3. Distribution of patent assignees, inventors, and references. For all panels, a right-skewed histogram is visualized using a logarithmic scale for the vertical axis. In the upper panel, the histogram visualizes the number of patents per assignee; the central panel visualizes the number of patents per inventor; and the lower panel visualizes the number of citations received by each patent that was cited at least once. |
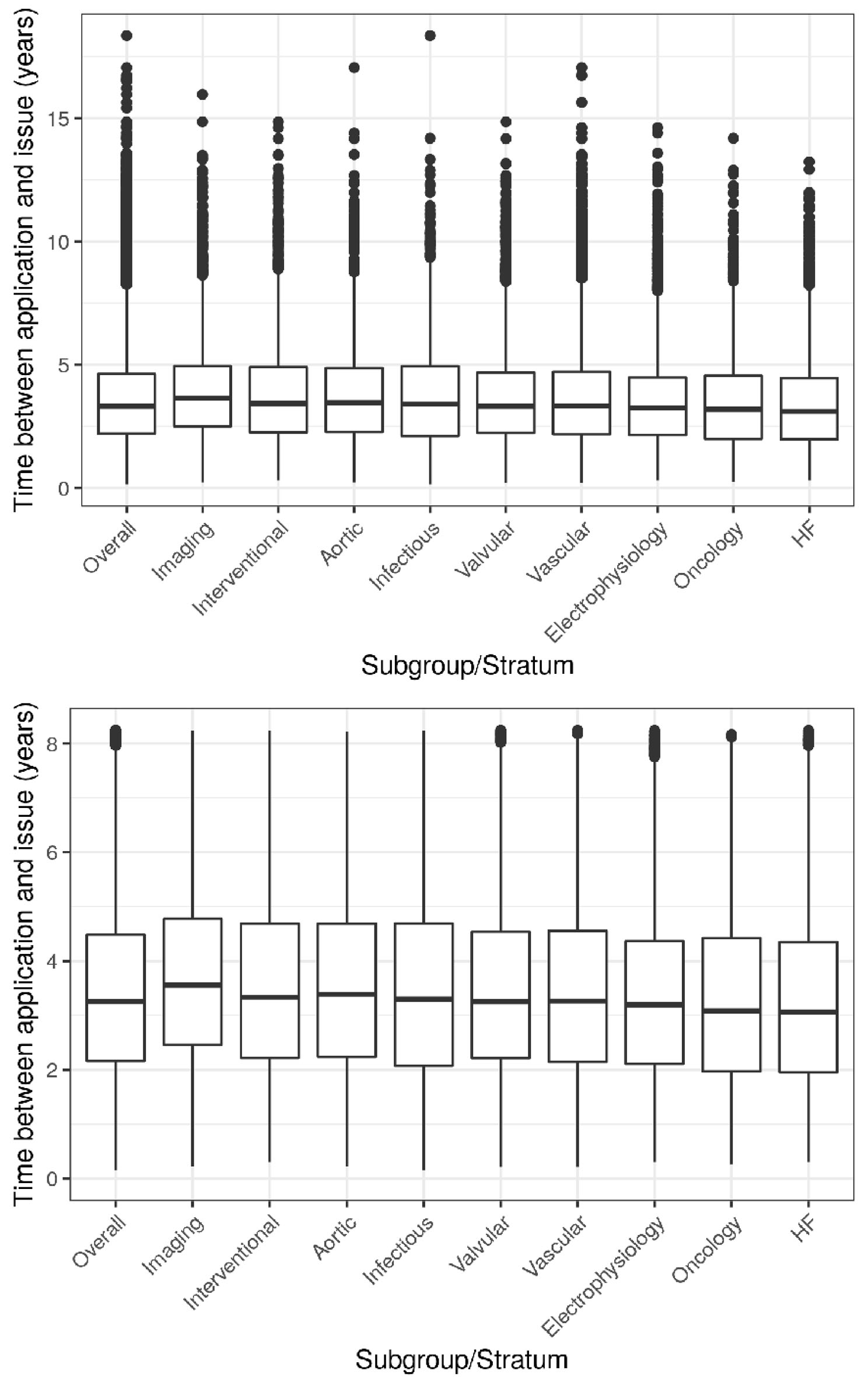
Given the large number of patents that must be processed by the USPTO, there are often years-long delays between date of patent application and date of patent issuance. For cardiology-related patents overall and for the 10 defined subgroups, the majority of patents appear to be issued within a half-decade after application (Fig. 4), with significant differences between subgroups (ANOVA: F = 20.6; df = 8; P < 0.001). Patents related to cardiac imaging take the longest (median (interquartile range (IQR)): 3.6 years (2.5 - 4.9)) and patents related to heart failure take the shortest (3.1 years (2.0 - 4.5)), with about a half year difference between the two. Overall, 80% of cardiology-related patents were issued within 5 years of application and 99% were issued within a decade of application.
 Click for large image | Figure 4. Stratified temporal lag between patent submission and issuance. Boxplots of time (years) elapsed between the date a patent was submitted to the USPTO and the date it was issued. Left panel visualizes all patents; right panel excludes outliers and allows clearer comparison between subgroups. |
| Discussion | ▴Top |
The number of cardiology-related patents issued annually in the United States nearly tripled between 2005 and 2020, with each subfield within cardiology also demonstrating an upward trend in issued patents. Of note, the aortic subgroup is a strict subset of the vascular subgroup. This diverges from their definitions as clinical practice as vascular specialists tend not to manage aortic conditions, which generally fall under the care of cardiologists or cardiac surgeons. The sharpest upward trend was noted in the valvular subfield with a majority of the most cited patents also relating to cardiac valves. The trend could be a consequence of increased interventional capabilities within recent years. This result leads to strategic insight in at least the following two forms: 1) it guides research by exposing underexplored subfields of cardiology and 2) studying the early rise of valvular patents can permit identification of the next “hot” subfield within cardiology and guide financial investment. Also noteworthy in the results is the years-long and subspecialty-dependent lag between patent application and issuance. Studying historical trends in this time lag guides planning and strategy for patentable innovations in any context, whether in academic institutions or corporations. Identifying institutions with prolific histories of granted patents helps identify hotspots of innovation within the United States. These institutions would not only have an established record of patents reflecting past innovation, but they would also likely have developed streamlined processes to integrate innovation into the workflow and culture of the institution. This is analogous to the idea that hospitals with physicians managing a high volume of rare conditions, e.g., cardiothoracic surgeons managing a high volume of aortic dissections, generally develop more efficiency and improved outcomes for those conditions.
A clear strength of this study is that every patent issued in the United States was collected; thus, if we trust the keyword filtering process, the patents analyzed in this report constitute a population and not a sample. This lends greater meaning and significance to the exploratory analysis conducted. Another strength is this study’s reproducibility. By providing a fully reproducible and publicly available software pipeline, not only can interested readers confirm and replicate results, but motivated readers can also adjust the pipeline. Adjustments can lead to deeper analysis with further inferential testing, broader analysis via inclusion of patents from other specialties of medicine, and even profitable analysis with modeling aimed at predicting revenue trends for publicly traded corporations.
Measuring patent issuance has limitations. Importantly, the number of cardiology-related patents from an academic institution or corporation does not necessarily correlate with a quantifiable impact on medical practice. This is at least partially because solely quantitative analysis does not capture the differences in patent quality. One potential measure for patent quality and impact is how often it has been cited [22]. Measuring how often a cardiology-related patent is cited could serve to improve identification of influential centers that drive innovation within cardiology. Another limitation inherent to patent data is that sufficiently protecting a single piece of intellectual property sometimes requires more than one patent, effectively increasing the number of patents without corresponding innovation. Most likely, this confounding factor differentially affects patents of different classes, e.g., patents for devices versus patents for drugs. Due to data limitations, this study could not identify whether cardiovascular patents were related to pharmaceuticals or medical devices. Specifically, due to a higher number of incremental improvements in devices versus drugs, patents in the former group likely have a higher average number of citations. This particular example is highlighted in Table 4, which lists no drug patents in the top 10 cited patents despite the monumental benefit of pharmacologic patents on cardiovascular disease. A potential solution to this scientometric issue involves standardizing the citation metric based on the class of patent. Yet, this poses a setback, i.e., creation of a new type of classification system not currently in place. Thus, the problem of measuring patent impact is analogous to the problem of measuring peer-reviewed journal article impact.
When selecting keywords to isolate cardiology-related patents, we chose to maximize specificity at the cost of sensitivity. In particular, we only selected patents that directly related to cardiovascular medicine. As an example, consider a cardiothoracic surgeon with a patent related to valve replacement and a patent related to a chest tube. Since the valve replacement patent has a direct relation to cardiovascular medicine, i.e., the patient’s care under a medical cardiologist would be directly affected by the replaced valve, the first patent would be included in our dataset. However, since the present of a chest tube placed after valve replacement surgery would not necessarily affect care under a medical cardiologist after discharge, the second patent would not be included in our dataset. Similarly, innovations with broad implications for medicine not specific to cardiology would not have been included in the dataset either. This implies that our results likely underestimate the number of cardiology-related patents that have been granted. However, we assume that we have underestimated the number of patents equally across all subspecialties, preserving the presented trends. Essentially, while the general results, such as directions of trends, are valid, the exact numbers presented should be taken with a grain of salt.
The clear right skew in the distributions visualized in Figure 3 shows that while there are many players in the patent network, a small number of players are responsible for a disproportionately large number of granted patents. For the distributions of assignees and inventors, this could represent the presence of innovation hotspots across the nation that are responsible for driving forward innovation within cardiovascular medicine. Of note, when visualized with a logarithmic vertical axis, the distributions do exhibit a degree of linearity consistent with power-law distributions. Further investigation is necessary to confirm whether these thick-tailed histograms can be considered power-law distributions. If true, this insight would have a significant impact in the sub-disciplines of scientometrics and bibliometrics that focus on patents. This would also allow taking advantage of mathematical concepts, e.g., graph theory and machine learning, to predict cardiovascular innovations using patent data [23].
Although citations to a patent may serve as a useful quantitative measure of its direct impact, the value (tangible and intangible) of a patent is more challenging to discern. If interested in the financial value, accurate estimation would require knowledge about the negative cash flows leading up to patent issuance and positive cash flows following it. Even financial statements of publicly traded and not-for-profit corporations would not include this information in detail for each patent. Estimating economic value poses a more complex challenge, requiring information about the number of patients who benefitted from the patent, the mean number of quality-adjusted life years saved per patient, and so on. Economic impact analyses of specific patents could be theoretically estimated based on need and expected market penetration; however, this would lead to a high degree of uncertainty that could only be validated years after patent issuance. While this form of economic analysis is certainly possible and could be pursued by corporations attempting to estimate revenue, it also comes with many issues that would limit utility in an academic context. It should be noted that the financial value of a patent would not necessarily serve as a useful proxy for economic value. A clear example of this would be a patent that is not marketable itself but serves as an intermediate step upon which a corporation or its competitors build in order to successfully develop a marketable innovation. Another relevant example would be a patent with a valuable innovation whose financial value drops because a competitor adds modifications to preserve function yet avoid breach of intellectual property.
Here, we explore the landscape of cardiology-related patents in the United States. Even exploratory analysis provides useful insights from this hitherto underused dataset. Further inferential and predictive analysis of the rich data should yield insight into the innovation expected within the field of cardiovascular medicine in the upcoming years. This report opens multiple avenues for next steps. In particular, retrospective analysis of the valvular subfield may lead to identifying drivers of innovation within the patent database, and permit researchers and investors to predict the next subfield within cardiology with the most rapid development. In contrast to studying the more mature valvular subfield, there is also considerable benefit in studying fields like preventive cardiology. Specifically, there remain significant unaddressed niches within preventive cardiology, scientific [24] and interpersonal [25], that have the potential to improve societal cardiovascular health. The scientific subset will certainly be addressed, not only through guidelines, but through new innovation in the area, and can thus be studied via patents. Additionally, further data enhancement to link institutions and their corporate subsidiaries would permit accurate evaluation of whether cardiovascular innovation is led by individual inventors, academic institutions, or for-profit corporations. In-depth study of the landscape of cardiovascular patents could help physicians and scientists address unmet patient need and improve long-term clinical outcomes.
| Supplementary Material | ▴Top |
Suppl 1. Keywords for cardiology-related patents.
Suppl 2. Manual evaluation of cardiology-related patents.
Acknowledgments
The authors thank the Cleveland Clinic and Case Western Reserve University. Dr. Desai acknowledges the Haslam Family Endowed Chair in Cardiovascular Medicine.
Financial Disclosure
This was a no-cost, unfunded study.
Conflict of Interest
All authors state no conflict of interest, financial or otherwise, relevant to this study.
Informed Consent
This study did not involve human subjects. As such, no informed consent procedures were necessary.
Author Contributions
RRW, JY, and MYD devised this study. RRW and MYD designed the analysis plan. RRW, JY, and MYD determined the data needs. RRW and JY collected all data. RRW, BMM, JY, SRK, AMG, LGS, and MYD validated the data (including manual review) and provided critical input for revised collection. RRW and MYD analyzed the data. RRW, BMM, JY, and MYD prepared the initial manuscript. RRW, BMM, JY, SRK, AMG, LGS, and MYD provided critical input to the manuscript. MYD supervised all steps.
Data Availability
All data are publicly available at the United States Patent and Trademark Office website.
| References | ▴Top |
- Drummond MF, Sculpher MJ, Claxton K, Stoddart GL, W TG. Methods for the economic evaluation of health care programmes. 4th ed: Oxford University Press; 2015.
- Lakdawalla D, Malani A, Reif J. The insurance value of medical innovation. Journal of Public Economics. 2017;145:94-102.
- Ramlogan R, Consoli D. Knowledge, understanding, and the dynamics of Medical Innovation. Manchester Institute of Innovation Research, Manchester Business School. 2008;539:1-20.
- Gelijns AC, Thier SO. Medical innovation and institutional interdependence: rethinking university-industry connections. JAMA. 2002;287(1):72-77.
doi pubmed - Ventose E. Medical Patent Law - the challenges of medical treatment. Edward Elgar Publishing Inc; 2011.
- Bloomberg CA, Marylander SJ, Yaeger PM. Patenting medical technology. "To promote the progress of science and useful arts". N Engl J Med. 1987;317(9):565-567.
doi pubmed - Chatterji AK, Fabrizio KR, Mitchell W, Schulman KA. Physician-industry cooperation in the medical device industry. Health Aff (Millwood). 2008;27(6):1532-1543.
doi pubmed - Yu J, Beltz H, Desai MY, Erdi P, Scott JG, Wadhwa RR. Accessing United States bulk patent data with patentpy and patentr. arXiv. 2021.
- McKinney W. Data structures for statistical computing in Python. Paper presented at: 9th Python in Science Conference. 2010.
- Foundation PS. Python language reference.2020. https://www.python.org.
- Team RC. R: A language and environment for statistical computing. In: Vienna, Austria: R Foundation for Statistical Computing. 2021. https://www.R-project.org.
- Auguie B. gridExtra: Miscellaneous Functions for “Grid” Graphics, version 2.3. Comprehensive R Archive Network. 2017. https://CRAN.R-project.org/package=gridExtra.
- Bache SM, Wickham H. magrittr: A Forward-Pipe Operator for R, version 2.0.1. Comprehensive R Archive Network. 2020. https://CRAN.R-project.org/package=magrittr.
- Grolemund G, Wickham H. Dates and times made easy with lubridate. Journal of Statistical Software. 2011;40(3):1-25.
- Pohlert T. Trend: non-parametric trend tests and change-point detection, version 1.1.4. Comprehensive R Archive Network. 2020. https://CRAN.R-project.org/package=trend.
- Wickham H, Averick M, Bryan J, et al. Welcome to the tidyverse. Journal of Open Source Software. 2019;4(43).
- Wilke CO. Cowplot: streamlined plot theme and plot annotations for ‘ggplot2’, version 1.1.1. Comprehensive R Archive Network. 2020. https://CRAN.R-project.org/package=cowplot.
- Mann HB. Nonparametric tests against trend. Econometrica. 1945;13(3):245-259.
- Kendall MG. Rank correlation methods. London, UK: Griffin. 1975.
- Fisher RA. On the “probable error” of a coefficient of correlation deduced from a small sample. Metron. 1921;1:3-32.
- Wadhwa RR, Yu J, Desai MY. Reproducible scripts for an exploratory analysis of cardiology-related patents. GitHub. https://github.com/rrrlw/patent-cardiology. 2021.
- Saha S, Saint S, Christakis DA. Impact factor: a valid measure of journal quality? J Med Libr Assoc. 2003;91(1):42-46.
pubmed pmc - Erdi P, Makovi K, Somogyvari Z, et al. Prediction of emerging technologies based on analysis of the US patent citation network. Scientometrics. 2013;95:225-242.
- Atar D, Jukema JW, Molemans B, Taub PR, Goto S, Mach F, CerezoOlmos C, et al. New cardiovascular prevention guidelines: How to optimally manage dyslipidaemia and cardiovascular risk in 2021 in patients needing secondary prevention? Atherosclerosis. 2021;319:51-61.
doi pubmed - Duffy EY, Ashen D, Blumenthal RS, Davis DM, Gulati M, Blaha MJ, Michos ED, et al. Communication approaches to enhance patient motivation and adherence in cardiovascular disease prevention. Clin Cardiol. 2021;44(9):1199-1207.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.