

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 13, Number 5, October 2022, pages 309-314

Chronic Kidney Disease Stage G4 in a Diabetic Patient Improved by Multi-Disciplinary Treatments Based Upon Literature Search for Therapeutic Evidence
Hidekatsu Yanaia, b, Naoki Yamaguchia, Hiroki Adachia
aDepartment of Diabetes, Endocrinology and Metabolism, National Center for Global Health and Medicine Kohnodai Hospital, Chiba, Japan
bCorresponding Author: Hidekatsu Yanai, Department of Diabetes, Endocrinology and Metabolism, National Center for Global Health and Medicine Kohnodai Hospital, 1-7-1 Kohnodai, Ichikawa, Chiba 272-8516, Japan
Manuscript submitted August 18, 2022, accepted September 6, 2022, published online October 25, 2022
Short title: CKD Improved by Multi-Disciplinary Treatments
doi: https://doi.org/10.14740/cr1424
| Abstract | ▴Top |
In the EMPA-REG OUTCOME trial, sodium-glucose cotransporter 2 (SGLT2) inhibitor, empagliflozin, reduced incident or worsening nephropathy. In the LEADER trial, a glucagon-like peptide 1 (GLP-1) receptor agonist, liraglutide, resulted in lower rates of the development and progression of diabetic kidney disease than placebo. Therefore, the American Diabetes Association and the European Association for the Study of Diabetes recommend the decision to treat high-risk individuals with a GLP-1 receptor agonist or SGLT2 inhibitor to reduce chronic kidney disease (CKD) progression should be considered. A 72-year-old male obese diabetic patient developed CKD stage G4 despite of use of both SGLT2 inhibitor and GLP-1 receptor agonist. We started using sodium bicarbonate because he showed metabolic acidosis due to uremia. We also started to use spherical carbonaceous adsorbent which adsorbs indole, the precursor of indoxyl sulfate, uremic toxin. We started the treatment with finerenone, a nonsteroidal, selective mineralocorticoid receptor antagonist, which has been recently shown to lower risks of CKD progression. Considering unfavorable effects of hyperuricemia on CKD, to treat his hyperuricemia, we started to use dotinurad, a novel selective urate reabsorption inhibitor, which reduces serum urate levels by selective inhibition of urate transporter 1. The improvement of CKD stage G4 in a diabetic patient was obtained by such multi-disciplinary treatments in addition to SGLT2 inhibitor and GLP-1 receptor agonist.
Keywords: Chronic kidney disease; Glucagon-like peptide 1 receptor agonist; Hyperuricemia; Sodium-glucose cotransporter 2 inhibitor; Uremic toxin
| Introduction | ▴Top |
Patients with type 2 diabetes at high risk for cardiovascular events who received sodium-glucose cotransporter 2 (SGLT2) inhibitor, empagliflozin, as compared with placebo, had a lower rate of the primary composite cardiovascular outcome and of death from any cause (EMPA-REG OUTCOME trial) [1]. Empagliflozin was also associated with slower progression of kidney disease and lower rates of clinically relevant renal events than was placebo when added to standard care such as angiotensin-converting-enzyme inhibitor or angiotensin receptor blocker (ARB) [2]. In the LEADER trial, the rate of the first occurrence of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke among patients with type 2 diabetes mellitus was lower with a glucagon-like peptide 1 (GLP-1) receptor agonist, liraglutide than with placebo [3]. Liraglutide also resulted in lower rates of the development and progression of diabetic kidney disease than placebo [4]. The American Diabetes Association and the European Association for the Study of Diabetes have briefly updated their 2018 recommendations on management of hyperglycemia, based on important research findings from large cardiovascular outcomes trials published in 2019 [5]. Important changes including the decision to treat high-risk individuals with a GLP-1 receptor agonist or SGLT2 inhibitor to reduce major adverse cardiovascular events (MACEs), hospitalization for heart failure, cardiovascular death, or chronic kidney disease (CKD) progression should be considered independently of baseline HbA1c or individualized HbA1c target [5].
Are there any treatments in a diabetic patient who developed CKD stage G4 even with the appropriate use of ARB, empagliflozin and liraglutide? We experienced the improvement of CKD stage G4 in a diabetic patient, by multi-disciplinary treatments in addition to ARB, SGLT2 inhibitor and GLP-1 receptor agonist.
| Case Report | ▴Top |
A 72-year-old male obese (body mass index: 34.2 kg/m2) diabetic patient was referred to us because of poor glucose control (HbA1c: 10.8%) in 2014, and he already showed overt proteinuria because his diabetes duration was over 20 years. We started to control glucose by basal insulin and dipeptidyl peptidase 4 inhibitor, and his glucose control was promptly improved to the level of HbA1c below 7%. His hypertension and dyslipidemia have been treated by cardiologist, with beta-blocker, carvedilol (5 mg/day), ARB, azilsartan (40 mg/day), Ca2+ channel blocker, nifedipine (40 mg/day), alpha-blocker, doxazosin (8 mg/day), and rosuvastatin (2.5 mg/day). In 2017, his serum creatinine increased to 1.25 mg/dL, and we started using empagliflozin (25 mg/day) on March 2018 (Fig. 1). Since an elevation in serum creatinine and overt proteinuria continued, we started to use liraglutide. His serum creatinine levels had been decreased and been stable until 2020. Recently, his renal function was remarkably deteriorated. Serum blood urea nitrogen (BUN) and creatinine levels increased to 40 mg/dL (normal range, 8 - 20 mg/dL) and 2.43 mg/dL (normal range, 0.65 - 1.07), respectively, and estimated glomerular filtration rate (eGFR) decreased to 22 mL/min/1.73 m2. Blood gas analysis showed blood pH was 7.33, indicating an existence of metabolic acidosis.
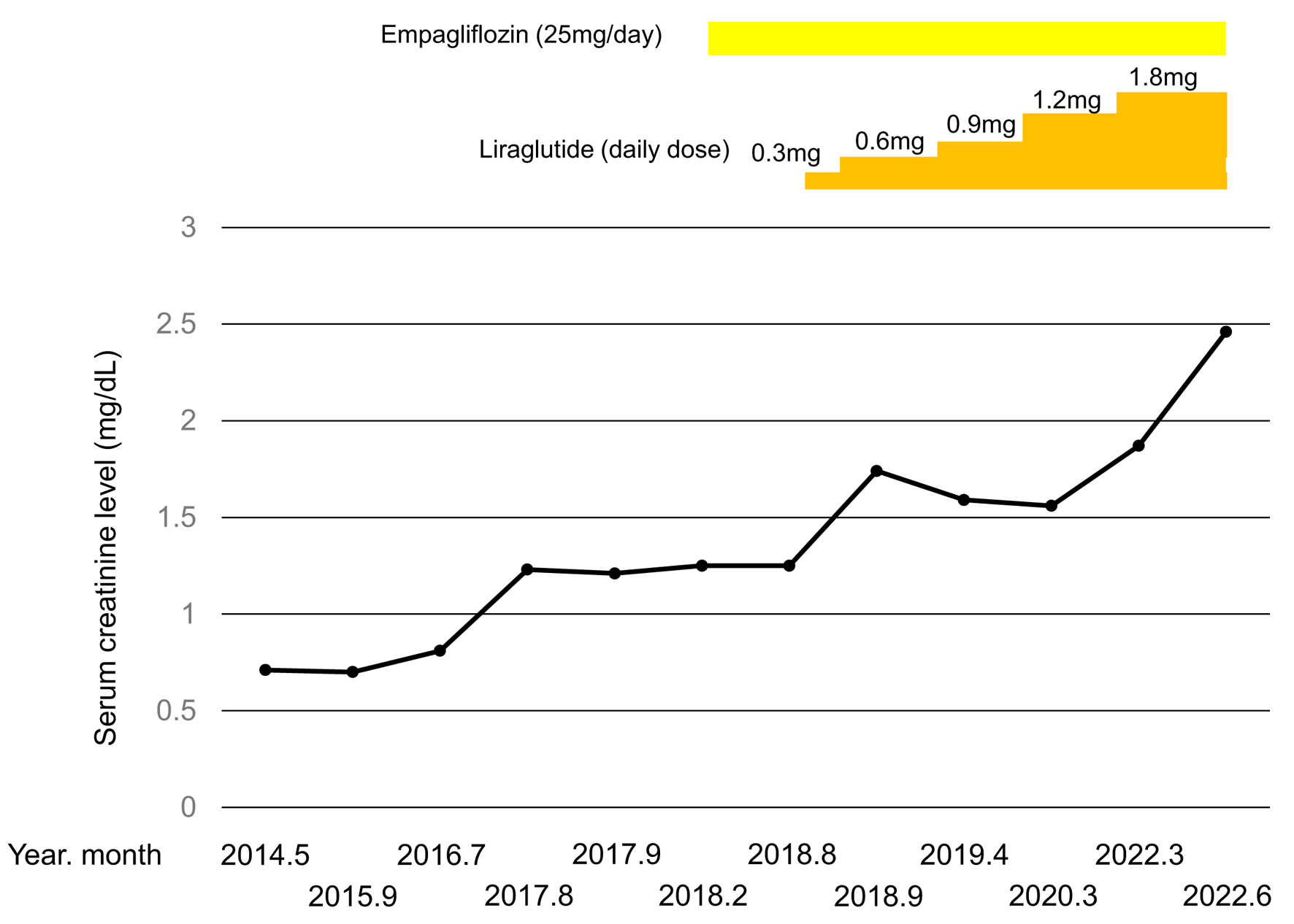 Click for large image | Figure 1. Change in serum creatinine level from May 2014 to June 2022 in a diabetic patient who developed CKD stage G4. CKD: chronic kidney disease. |
We stared to treat his renal failure by multi-disciplinary treatments based upon the therapeutic evidences for CKD.
We started to use sodium bicarbonate because he showed metabolic acidosis due to uremia. We also started to use spherical carbonaceous adsorbent which adsorbs indole, the precursor of indoxyl sulfate (IS), uremic toxin. Very recently, the treatment with finerenone, a nonsteroidal, selective mineralocorticoid receptor antagonist, has been shown to lower risks of CKD progression and cardiovascular events than placebo in patients with CKD and type 2 diabetes [6]. Therefore, we started the treatment with finerenone. He showed elevated hyperuricemia (serum uric acid (UA), 7.9 mg/dL). High-evidenced studies suggest a pathogenic role of hyperuricemia in the development of CKD [7]. To treat his hyperuricemia, we started to use dotinurad, a novel selective urate reabsorption inhibitor (SURI), which reduces serum UA levels by selective inhibition of urate transporter 1 (URAT1) [8].
Changes in eGFR, BUN and urate are shown in Figure 2. The start to use sodium bicarbonate, spherical carbonaceous adsorbent and finerenone promptly reduced BUN and increased eGFR. Dose-up of finerenone and the start of dotinurad further decreased BUN and increased eGFR. Dose-up of dotinurad further decreased BUN and increased eGFR with decreased UA.
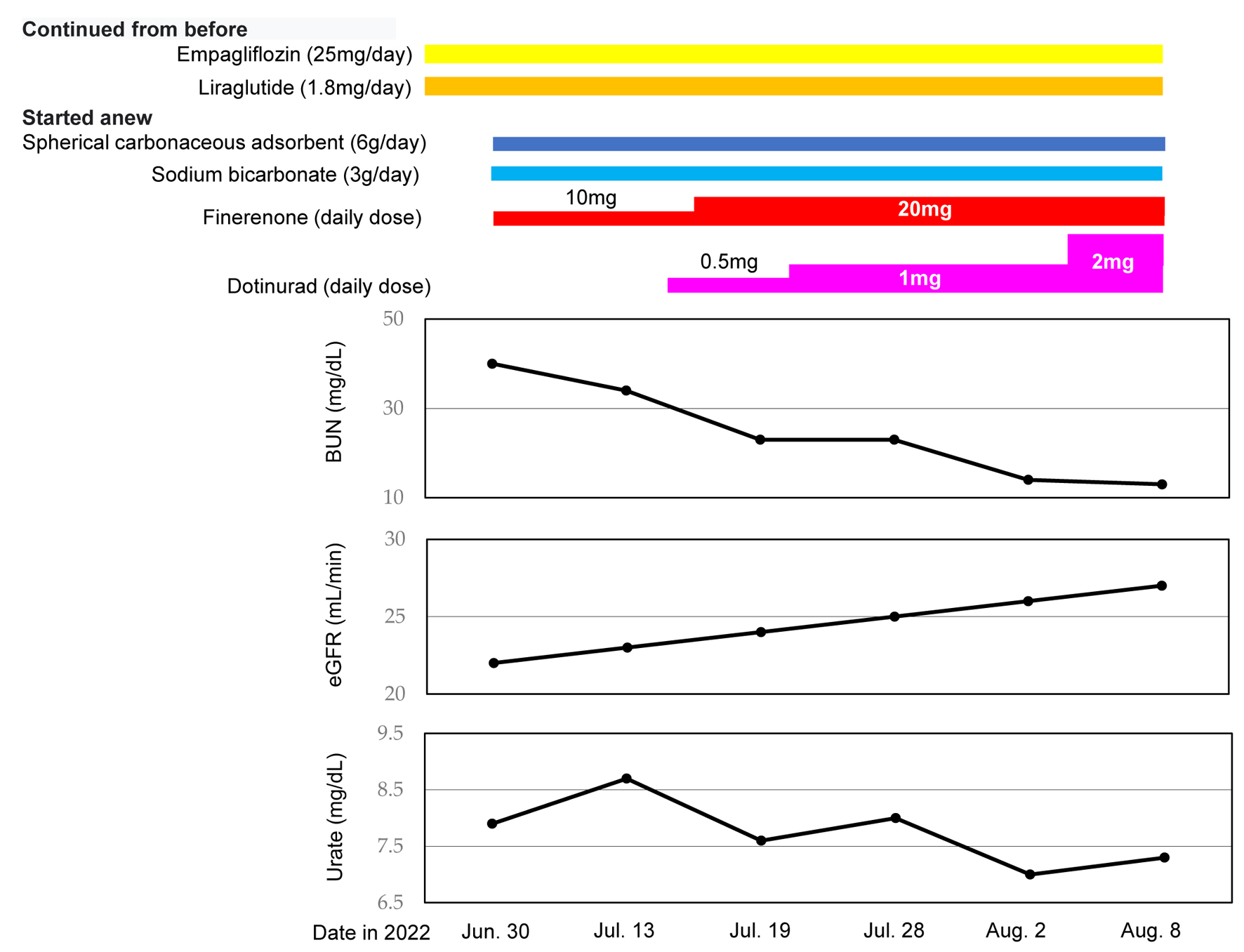 Click for large image | Figure 2. Changes in serum BUN, eGFR and urate after June 2022 in a diabetic patient who developed CKD stage G4. BUN: blood urea nitrogen; CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate. |
Change in urinary albumin/creatinine ratio is shown in Figure 3. Dose-up of liraglutide reduced urinary albumin/creatinine ratio from 4,928 to 3,935 and the start of sodium bicarbonate, spherical carbonaceous adsorbent, finerenone and dotinurad further decreased urinary albumin/creatinine ratio from 3,935 to 2,277.
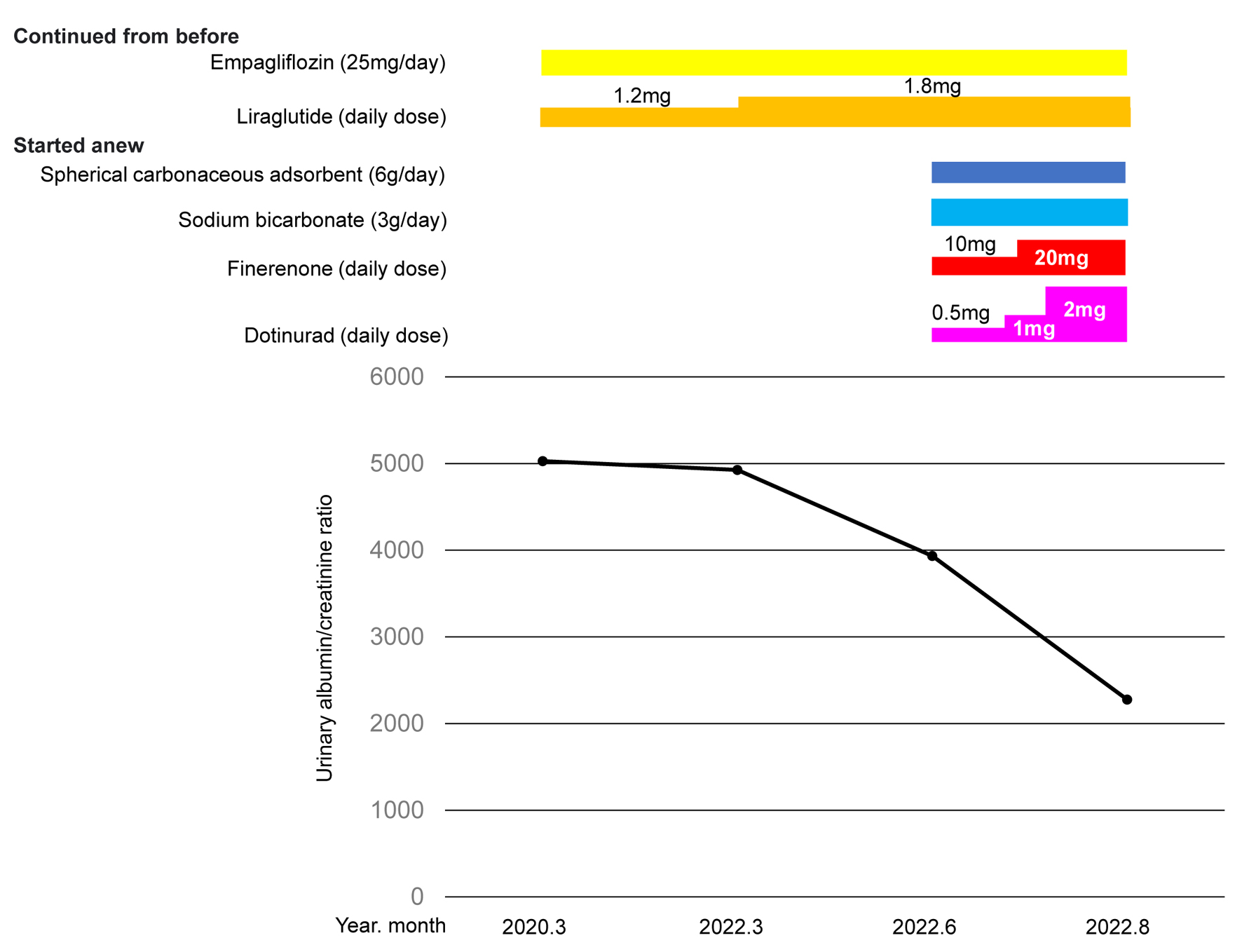 Click for large image | Figure 3. Change in urinary albumin/creatinine ratio after March 2020 in a diabetic patient who developed CKD stage G4. CKD: chronic kidney disease. |
| Discussion | ▴Top |
In the EMPA-REG OUTCOME trial, SGLT2 inhibitor, empagliflozin, reduced incident or worsening nephropathy by 39%, progression to macroalbuminuria by 38%, doubling of serum creatinine level by 44% as compared with placebo [2]. Empagliflozin might have retarded doubling of serum creatinine level, however, failed to suppress progression of CKD in our patient. In the LEADER trial, the renal outcome occurred in fewer participants in the liraglutide group than in the placebo group (hazard ratio (HR), 0.78; 95% confidence interval (CI), 0.67 to 0.92; P = 0.003). This result was driven primarily by the new onset of persistent macroalbuminuria, which occurred in fewer participants in the liraglutide group than in the placebo group (HR, 0.74; 95% CI, 0.60 to 0.91; P = 0.004) [4]. Liraglutide failed to reduce persistent doubling of serum creatinine level (HR, 0.89; 95% CI, 0.67 to 1.19; P = 0.43), renal-replacement therapy (HR, 0.87; 95% CI, 0.61 to 1.24; P = 0.44) [4]. Liraglutide reduced urinary albumin/creatinine ratio and temporarily reduced serum creatinine levels, however, could not suppress progression of CKD in our patient. Are there any treatments in a diabetic patient who developed CKD stage G4 even with the appropriate use of ARB, empagliflozin and liraglutide? We experienced the improvement of CKD stage G4 in a diabetic patient, by multi-disciplinary treatments in addition to ARB, SGLT2 inhibitor and GLP-1 receptor agonist.
Metabolic acidosis is a common complication in CKD patients, and is associated with an accelerated decline in renal function. Oral bicarbonate therapy has been used to counteract metabolic acidosis in CKD. The systematic review to summarize evidence from randomized controlled trials (RCTs) concerning the benefits and risks of bicarbonate therapy on kidney outcomes showed that compared with placebo or no study medication, sodium bicarbonate retarded the decline in kidney function (standardized mean difference (SMD), 0.26; 95% CI, 0.13 to 0.40), and reduced the risk of end-stage kidney failure (risk ratio (RR), 0.53; 95% CI, 0.32 to 0.89). Sodium bicarbonate reduced proteinuria (SMD, -0.09; 95% CI, -0.27 to 0.09). This study suggested that sodium bicarbonate may slow CKD progression [9]. Another systematic review and meta-analysis showed that oral bicarbonate supplementation resulted in a slightly higher eGFR (MD, 3.1 mL/min/1.73 m2; 95% CI, 1.3 to 4.9) at the end of follow-up compared to those given placebo or conventional CKD treatment [10].
An oral spherical carbonaceous adsorbent was approved for clinical use in Japanese CKD patients in 1991. It adsorbs indole, the precursor of IS, in the intestines and prevents IS production. IS, initially identified as a major uremic toxin that causes uremic symptoms, contributes to CKD progression. An oral spherical carbonaceous adsorbent decreases serum IS in a dose-dependent manner [11]. The uremic toxin IS accumulates in patients with CKD as a consequence of altered gut microbiota metabolism and a decline in renal excretion. IS was measured in 604 pediatric participants (mean eGFR, 27 mL/min/1.73 m2) at enrolment into the prospective Cardiovascular Comorbidity in Children with CKD study [12]. Associations with progression of CKD were analyzed by Kaplan-Meier analyses and Cox proportional hazard models. During a median follow-up time of 2.2 years, the composite renal survival endpoint, defined as 50% loss of eGFR, or eGFR < 10 mL/min/1.73 m2 or start of renal replacement therapy, was reached by 360 patients. Median survival time was shorter in patients with IS level in the highest versus lowest quartile (1.5 years; 95% CI, 1.1 to 2.0 versus 6.0 years; 95% CI, 5.0 to 8.4), suggesting the important role of uremic toxins and accentuating the unmet need of effective elimination strategies to lower the uremic toxin burden and abate progression of CKD.
Evidence supports a pathophysiological role for overactivation of the mineralocorticoid receptor in cardiorenal diseases, including CKD and diabetes, through inflammation and fibrosis that lead to progressive kidney and cardiovascular dysfunction [13]. Finerenone, a nonsteroidal, selective mineralocorticoid receptor antagonist, had more potent anti-inflammatory and anti-fibrotic effects than steroidal mineralocorticoid receptor antagonists in preclinical models [14]. Very recently, the treatment with finerenone resulted in lower risks of CKD progression than placebo in patients with CKD and type 2 diabetes [6].
In the meta-analysis including 15 cohorts, RR of CKD was 1.22 (95% CI, 1.16 to 1.28) per 1 mg/dL serum UA level increment [15]. A systematic review and meta-analysis including 13 studies showed a significant positive association between elevated serum UA levels and the new-onset CKD at follow-up (odds ratio (OR), 1.15; 95% CI, 1.05 to 1.25) [16]. Hyperuricemia was found to be an independent predictor for the development of newly diagnosed CKD in non-CKD patients (OR, 2.35; 95% CI, 1.59 to 3.46). Such high-evidenced studies suggest a pathogenic role of hyperuricemia in the development of CKD [7].
However, the meta-analyses failed to prove that UA-lowering treatments suppress the progression of CKD [17-19]. Only one recent meta-analysis showed that xanthine oxidase inhibitors (XOIs) significantly reduced the risk of end stage renal disease compared to the control (three studies; RR, 0.42; 95% CI, 0.22 to 0.80) and also improved eGFR in data pooled from RCTs with long follow-up times (> 3 months) (four studies; MD, 6.82 mL/min/1.73 m2; 95% CI, 3.50 to 10.15) and high methodological quality (blind design) (three studies; MD, 2.61 mL/min/1.73 m2; 95% CI, 0.23 to 4.99) [20].
Hyperuricemia was classified into UA overproduction type, UA underexcretion type, or their combined type. In Japan, prevalence of each type is estimated to be 10%, 60%, and 30%, respectively [21]. The second edition of the Japanese management guidelines recommends the use of XOIs, such as allopurinol, febuxostat and topiroxostat, for overproduction type, and uricosuric drugs, such as probenecid and benzbromarone, for underexcretion type [21]. In the recently revised Japanese management guidelines third edition, classification of hyperuricemia is into the three types: underexcretion type, renal load type, or combined type. The renal load type, a newly classification concept, was changed from overproduction type because it has been understood that the conventional overproduction type includes the extrarenal underexcretion type (decreased uric acid excretion from the intestine) [22]. In most Japanese patients, hyperuricemia is classified into underexcretion type. Thus, treatment with hypouricemic agents that increase urinary uric acid excretion could be useful in the majority of patients. Dotinurad, a novel SURI, reduced serum UA levels by selective inhibition of URAT1 in the treatment of hyperuricemia with or without gout [8]. ATP-binding cassette, subfamily G2 (ABCG2) has been identified as a high-capacity UA exporter that mediates renal and/or extra-renal UA excretion [23, 24]. ABCG2 is now known to be involved as well in UA excretion into the intestine [25]. ABCG2 is also a major transporter of the uremic toxin, IS. ABCG2 regulates the pathophysiological excretion of IS and strongly affects CKD survival rates. Another uricosuric drug, benzbromarone, and XOIs such as febuxostat and topiroxostat were reported to inhibit ABCG2 [26]. Inhibition of ABCG2 may induce accumulation of IS in kidney and may enhance renal UA overload by inhibiting intestinal UA excretion. Dotinurad which reduces renal UA reabsorption and does not inhibit ABCG2 might suppress progression of CKD.
Conclusion
We experienced the improvement of CKD stage G4 in a diabetic patient, by multi-disciplinary treatments such as sodium bicarbonate, spherical carbonaceous adsorbent, finerenone and dotinurad in addition to ARB, SGLT2 inhibitor and GLP-1 receptor agonist.
Acknowledgments
We thank the staffs of the Division of Research Support, National Center for Global Health and Medicine Kohnodai Hospital.
Financial Disclosure
Authors have no financial disclosures to report.
Conflict of Interest
The authors declare that they have no conflict of interest concerning this article.
Informed Consent
Patient consent for publication was obtained.
Author Contributions
HY designed the research. NY and HA collected and analyzed data. HY wrote and approved the final paper.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117-2128.
doi pubmed - Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, Johansen OE, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323-334.
doi pubmed - Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, Nissen SE, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311-322.
doi pubmed - Mann JFE, Orsted DD, Brown-Frandsen K, Marso SP, Poulter NR, Rasmussen S, Tornoe K, et al. Liraglutide and renal outcomes in type 2 diabetes. N Engl J Med. 2017;377(9):839-848.
doi pubmed - Buse JB, Wexler DJ, Tsapas A, Rossing P, Mingrone G, Mathieu C, D'Alessio DA, et al. 2019 Update to: management of hyperglycemia in type 2 diabetes, 2018. a consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2020;43(2):487-493.
doi pubmed - Bakris GL, Agarwal R, Anker SD, Pitt B, Ruilope LM, Rossing P, Kolkhof P, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020;383(23):2219-2229.
doi pubmed - Yanai H, Adachi H, Hakoshima M, Katsuyama H. Molecular biological and clinical understanding of the pathophysiology and treatments of hyperuricemia and its association with metabolic syndrome, cardiovascular diseases and chronic kidney disease. Int J Mol Sci. 2021;22(17):9221.
doi pubmed - Taniguchi T, Ashizawa N, Matsumoto K, Saito R, Motoki K, Sakai M, Chikamatsu N, et al. Pharmacological evaluation of dotinurad, a selective urate reabsorption inhibitor. J Pharmacol Exp Ther. 2019;371(1):162-170.
doi pubmed - Hultin S, Hood C, Campbell KL, Toussaint ND, Johnson DW, Badve SV. A systematic review and meta-analysis on effects of bicarbonate therapy on kidney outcomes. Kidney Int Rep. 2021;6(3):695-705.
doi pubmed - Hu MK, Witham MD, Soiza RL. Oral bicarbonate therapy in non-haemodialysis dependent chronic kidney disease patients: a systematic review and meta-analysis of randomised controlled trials. J Clin Med. 2019;8(2):208.
doi pubmed - Yamaguchi J, Tanaka T, Inagi R. Effect of AST-120 in chronic kidney disease treatment: still a controversy? Nephron. 2017;135(3):201-206.
doi pubmed - Holle J, Kirchner M, Okun J, Bayazit AK, Obrycki L, Canpolat N, Bulut IK, et al. Serum indoxyl sulfate concentrations associate with progression of chronic kidney disease in children. PLoS One. 2020;15(10):e0240446.
doi pubmed - Barrera-Chimal J, Girerd S, Jaisser F. Mineralocorticoid receptor antagonists and kidney diseases: pathophysiological basis. Kidney Int. 2019;96(2):302-319.
doi pubmed - Grune J, Beyhoff N, Smeir E, Chudek R, Blumrich A, Ban Z, Brix S, et al. Selective mineralocorticoid receptor cofactor modulation as molecular basis for Finerenone's antifibrotic activity. Hypertension. 2018;71(4):599-608.
doi pubmed - Zhu P, Liu Y, Han L, Xu G, Ran JM. Serum uric acid is associated with incident chronic kidney disease in middle-aged populations: a meta-analysis of 15 cohort studies. PLoS One. 2014;9(6):e100801.
doi pubmed - Li L, Yang C, Zhao Y, Zeng X, Liu F, Fu P. Is hyperuricemia an independent risk factor for new-onset chronic kidney disease?: A systematic review and meta-analysis based on observational cohort studies. BMC Nephrol. 2014;15:122.
doi pubmed - Kanji T, Gandhi M, Clase CM, Yang R. Urate lowering therapy to improve renal outcomes in patients with chronic kidney disease: systematic review and meta-analysis. BMC Nephrol. 2015;16:58.
doi pubmed - Fleeman N, Pilkington G, Dundar Y, Dwan K, Boland A, Dickson R, Anijeet H, et al. Allopurinol for the treatment of chronic kidney disease: a systematic review. Health Technol Assess. 2014;18(40):32014000722.
doi pubmed - Bose B, Badve SV, Hiremath SS, Boudville N, Brown FG, Cass A, de Zoysa JR, et al. Effects of uric acid-lowering therapy on renal outcomes: a systematic review and meta-analysis. Nephrol Dial Transplant. 2014;29(2):406-413.
doi pubmed - Pisano A, Cernaro V, Gembillo G, D'Arrigo G, Buemi M, Bolignano D. Xanthine oxidase inhibitors for improving renal function in chronic kidney disease patients: an updated systematic review and meta-analysis. Int J Mol Sci. 2017;18(11):2283.
doi pubmed - Yamanaka H, Japanese Society of G, Nucleic Acid M. Japanese guideline for the management of hyperuricemia and gout: second edition. Nucleosides Nucleotides Nucleic Acids. 2011;30(12):1018-1029.
doi pubmed - Japanese Society of Gout and Uric and Nucleic Acids. Guideline for the management of hyperuricemia and gout. 3rd ed. 2018. pp. 18-23, 95-8.
- Woodward OM, Kottgen A, Coresh J, Boerwinkle E, Guggino WB, Kottgen M. Identification of a urate transporter, ABCG2, with a common functional polymorphism causing gout. Proc Natl Acad Sci U S A. 2009;106(25):10338-10342.
doi pubmed - Matsuo H, Takada T, Ichida K, Nakamura T, Nakayama A, Ikebuchi Y, Ito K, et al. Common defects of ABCG2, a high-capacity urate exporter, cause gout: a function-based genetic analysis in a Japanese population. Sci Transl Med. 2009;1(5):5ra11.
doi pubmed - Takada T, Yamamoto T, Matsuo H, Tan JK, Ooyama K, Sakiyama M, Miyata H, et al. Identification of ABCG2 as an exporter of uremic toxin indoxyl sulfate in mice and as a crucial factor influencing CKD progression. Sci Rep. 2018;8(1):11147.
doi pubmed - Miyata H, Takada T, Toyoda Y, Matsuo H, Ichida K, Suzuki H. Identification of febuxostat as a new strong ABCG2 inhibitor: potential applications and risks in clinical situations. Front Pharmacol. 2016;7:518.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.