

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 13, Number 6, December 2022, pages 323-332

One Acute Exposure to E-Cigarette Smoke Using Various Heating Elements and Power Levels Induces Pulmonary Inflammation
Jianru Shia, b, Wangde Daia, b, Jesus Chaveza, Juan Carrenoa, Lifu Zhaoa, Michael T. Kleinmanc, d, Rebecca J. Arechavalac, Irene Hasenc, Amanda Tingc, Bishop Blissc, Jessica E. Monterrosa Menac, Robert A. Klonera, b, d
aCardiovascular Research Institute, Huntington Medical Research Institutes, Pasadena, CA 91105, USA
bDivision of Cardiovascular Medicine of the Keck School of Medicine, University of Southern California, Los Angeles, CA 90017-2395, USA
cDepartment of Environmental and Occupational Health, University of California, Irvine, CA 92717, USA
dCorresponding Author: Robert A. Kloner, Cardiovascular Research Institute, Huntington Medical Research Institutes, Pasadena, CA 91105, USA; Michael T. Kleinman, Department of Environmental and Occupational Health, University of California, Irvine, CA 92697-1830, USA
Manuscript submitted August 19, 2022, accepted October 10, 2022, published online December 16, 2022
Short title: eC Smoke Induces Pulmonary Inflammation
doi: https://doi.org/10.14740/cr1425
| Abstract | ▴Top |
Background: Electronic cigarettes (eC) may not be entirely benign. There is a lack of data on the effect of a single acute exposure of eC vapor using various heating sources and power settings upon lung injury. The purpose of this study was to determine if an acute exposure with eC vapor heated with different heating elements and power levels induced inflammatory changes in the lungs and heart.
Methods: Rats were exposed to pure air or received a single, 4-h exposure to eC vapor. The devices used either a stainless steel (SS) or nichrome (NC) heating element randomized to a low or high atomization power (45 versus 70 W). Rats were euthanized within 48 h of exposure.
Results: The eC groups showed accumulation of inflammatory cells in bronchial lumen, near the pleura, and within the alveolar spaces. The numbers of inflammatory cells per field in the lung parenchyma were significantly greater in the rats exposed to eC groups vs. the air group. There were significantly higher inflammatory gene expression changes in the lungs of animals assigned to 70 W power. We observed that eC vapor generated using burnt coils were toxic and could cause acute respiratory distress and myocarditis.
Conclusion: In conclusion, one 4-h exposure to eC vapor, in the absence of vitamin E oil or nicotine, significantly increased lung inflammation. Effects were seen after exposures to vapor generated using SS and NC heating elements at either high or low power. Vapor from devices with burnt coils can negatively affect the heart and lung.
Keywords: E-cigarette; Lung inflammation; Vaping; Burnt coil
| Introduction | ▴Top |
The use of electronic cigarettes (eC) has exploded in recent years. In 2020, it was estimated that over 3.6 million middle school and high school students had vaped; from 2017 to 2018, eC use had increased by 78% among high school seniors, from 12% to 21% in just 1 year [1, 2]. Globally, there were 7 million individuals who vaped in 2011; this number jumped to 41 million by 2018 [3]. Although vaping trends declined in 2020 [4], the authors predicted an estimated 55 million eC users by 2021 based on the data of market research group Euromonitor [3]. Of high school students, 11.3% (1.72 million) reported current eC use in 2021 [2]. A recent report by the US FDA and Centers for Disease Control and Prevention (CDC) stated that more than 2 million high school students and 470,000 middle school students used eC in the last 30 days (2021 National Youth Tobacco Survey [5]). Many smokers believe that eC are safer than combustible tobacco and eC use has been proposed as a technique to quit cigarette smoking [6]. While eC do not have some of the same toxins, such as tar, as standard tobacco cigarettes, their components, especially when heated, may not be benign. eC vapor can result in smaller particle sizes with an abundance of ultrafine particles compared to standard cigarettes, rendering them even more dangerous [7].
A new form of lung injury was described in users of eC, beginning around July 2019 and developed into a true epidemic by September 2019. The condition is now known as eC or vaping product use associated lung injury or EVALI (CDC, 2019). Since August 2019, there were more than 2,800 clinical cases of EVALI [8] reported with 68 deaths in the United States. CDC stopped collecting these data from states as of February 2020 due to the subsequent identification of the primary cause of EVALI, and the considerable decline in EVALI cases and deaths since a peak. The typical victim, who has been using eC (vaping) within days to weeks, presents with respiratory distress including shortness of breath, cough, chest pain, fever, fatigue, and gastrointestinal symptoms including nausea, vomiting and diarrhea. The patients are often hypoxic. Chest X-ray typically shows ground glass appearing bilateral pulmonary infiltrates [9, 10]. Histology has shown pneumonitis, bronchiolitis, and diffuse alveolar damage. Some reports have described infiltration of lipid-laden macrophages into the lungs [11, 12]. The phenomenon has been observed in people using a wide variety of eC liquid brands, substances and devices. The exact cause of EVALI remains to be determined.
CDC suggested that use of tetrahydrocannabinol (THC) and vitamin E acetate oil, which is often used to dilute THC, is the culprit. Although there may be an association between the presence of vitamin E acetate in the lungs of victims and the presence of EVALI [13], it is not clear that the vitamin E acetate is the true culprit. While vitamin E acetate and THC might contribute, we observed an experimental form of EVALI without either component [14]. In the present study, we determined whether an acute exposure with eC vapor heated with different heating elements and power levels causes pulmonary pathology, alters inflammatory genes in the lungs and assesses the effect of burnt coils in a rat experimental model.
| Materials and Methods | ▴Top |
The present study was approved by the Institutional Animal Care and Use Committees at Huntington Medical Research Institutes and University of California at Irvine, and was performed in accordance with the Guidelines for the Care and Use of Laboratory Animals (NIH publication No. 85-23, National Academy Press, Washington DC, revised 2011).
Experimental design
Sprague-Dawley rats (about 5 months of age; equivalent of young adults in humans) of either sex were acclimatized and received a 4-h exposure of eC vapor (50% propylene glycol, 50% vegetable glycerin; tobacco flavoring - classic tobacco flavoring, which is the lowest dose available, from VaporFi.com); they were randomized to stainless steel (SS) or nickel-chromium (NC) heating element, and to a high and low power (45 versus 70 W). There were 16 rats (eight males and eight females) in each of these four groups. As a negative control, 16 rats (eight males and eight females) were exposed to pure air.
Nose-only exposure model
Rats were exposed nose-only. In the nose-only exposure system, animals were restrained in individual holding tubes that were plugged into an exposure manifold (In-Tox Products, LLC, Clinton, MS) with just the snout exposed to the exposure atmosphere, which serves to minimize dermal exposure. The test atmosphere enters the nose-only manifold, is channeled to the individual animal ports and excess vapor exits through an exhaust port. Exhaled air from the animals is entrained and leaves with the exhaust air, which minimizes the potential for re-breathing by other animals and for CO2 buildup. eC vapor was generated using an electronically controlled, smoking machine, which was programmed to use various puff regimens and generated test aerosols with size distributions similar to those found under real-world conditions. Rats were monitored for respiratory distress (labored mouth breathing, reduced activity, and audible wheezing). We noted that after repeated use especially at the high wattage condition, some coils became “burnt”, i.e., the higher current flow burns the wick inside the coil and the burned wick does not distribute the liquid properly to the coil which causes localized overheating. This phenomenon has been documented by other investigators as well [15]. The condition of the coils and effects on experimental outcomes were tracked.
Tissue histological analysis
The rats (16 in each group, eight males and eight females) were euthanized with an overdose of barbiturates at 48 h post-exposure. The lungs were lavaged for analysis of fluid. The lungs were then removed and perfused with 10% formalin through the trachea in order to keep the alveoli from collapsing. The heart and lungs were then further fixed in 10% formalin, dissected and cut for histologic analysis. They were stained with hematoxylin and eosin (H&E). Inflammatory cells were counted from 12 random areas per section.
Bronchoalveolar lavage (BAL) and oil red O stain
A syringe was gently inserted into the trachea via a cannula. Cold saline was administered into the lung and then after 30 s was aspirated as the lavage fluid. Each aspirated lavage fluid sample was collected in a 15 mL conical tube. The lavage fluid was centrifuged at 2,000 rpm for 5 min. The cell pellet was resuspended in 1 mL of saline. Slides for cytology were prepared from the pellet suspension (40 µL). Slides were fixed and stained with H&E. Cells were differentiated by light microscopy according to their morphology. For macrophage lipid staining of the lung sections, we randomly chose five animals in each group for oil red O staining. Slides were stained with oil red O and counterstained with hematoxylin using a lipid staining kit (Sigma-Aldrich Ltd, Catalog # 0-0625). Oil red O positive macrophages were analyzed by light microscopy.
Quantitative reverse transcriptase polymerase chain reaction (qRT-PCR)
Lung tissues (n = 4 to 16 in each group) were extracted and frozen with liquid nitrogen for biochemical analysis. Total RNA was purified from T-Per lysates using Direct-zol RNA MiniPrep kit (Zymo Research #NC1047980, USA) following the manufacturer’s instructions. iScript cDNA synthesis kit (Bio-Rad #1708891) was used for cDNA synthesis and qRT-PCR was performed using a BioRad CFX connect thermocycler. Data were normalized to GAPDH levels. Primers used for qPCR include: angiotensin converting enzyme 2 (ACE2) forward 5’- GAATGCGACCATCAAGCG -3’, reverse 5’-CAAGCCCAGAGCCTACGA -3’; GAPDH forward 5’- GCAAGTTCAACGGCACAG -3’, reverse 5’- GCAAGTAGACTCCACGACAT -3’; interleukin-6 (IL-6) forward 5’- TACCACTTCACAAGTCGGAGGC -3’, reverse 5’- CTGCAAGTGCATCATCGTTGTTC -3’; tumor necrosis factor-α (TNF-α) forward 5’- ATACACTGGCCCGAGGCAAC -3’, reverse 5’- CCACATCTCGGATCATGCTTTC -3’; interleukin-1β (IL-1β) forward 5’- AATCTATACCTGTCCTGTGTGATGAAA -3’, reverse 5’- CTTTGGGTATTGTTTGGGATCC -3’; interleukin-10 (IL-10) forward 5’- AGGAGCATTTGAATTCCCTGG -3’, reverse 5’- AAATCGATGACAGCGTCGC -3’; vascular cell adhesion protein 1 (VCAM-1) forward 5’- GTGGGTGTTGAGGATGAGCA -3’, reverse 5’- ACAGTGACAGGTCTCCCGTGTA -3’; interferon gamma (IFN-γ) forward 5’- ACACTCATTGAAAGCCTACAAAGTCTG -3’, reverse 5’- ATTCTTCTTATTGGCACACTCTCTACC -3’; endothelin-1 forward 5’- GCCAAGCAGACAAAGAACTCCGAG -3’, reverse 5’- GCTCTGTAGTCAATGTGCTCGGTT -3’.
Statistical analysis
All results are expressed as means ± standard error of the mean (SEM) and analyzed using Student’s t-test or one-way analysis of variance (ANOVA) (Tukey test) as appropriate. Statistically significant differences were established at P < 0.05.
| Results | ▴Top |
Histological analysis of lung and heart
Rats were euthanized 48 h after their 4-h exposures, lungs were removed and formalin-fixed at constant pressure and 5 µm sections were cut and stained and prepared for light microscopy analyses. H&E-stained lung sections showed that the lung alveoli appeared normal in the air group (Fig. 1a); the eC groups using the SS or NC heating element with high or low power showed accumulation of inflammatory cells (mainly macrophages) in bronchial lumen (Fig. 1b), near the pleura (Fig. 1c), and within the alveolar spaces (Fig. 1d-f). We also observed intra-alveolar fluid in eC exposed rat (Fig. 1e, f). The numbers of inflammatory cells per field in the lung parenchyma were significantly greater in the rats exposed to eC using SS or NC heating element compared to the air control group (P < 0.05, one-way ANOVA, Tukey multiple comparison test; Fig. 1g). There were no differences among eC groups. There were no statistical gender differences. Therefore, the data by gender were pooled for analysis.
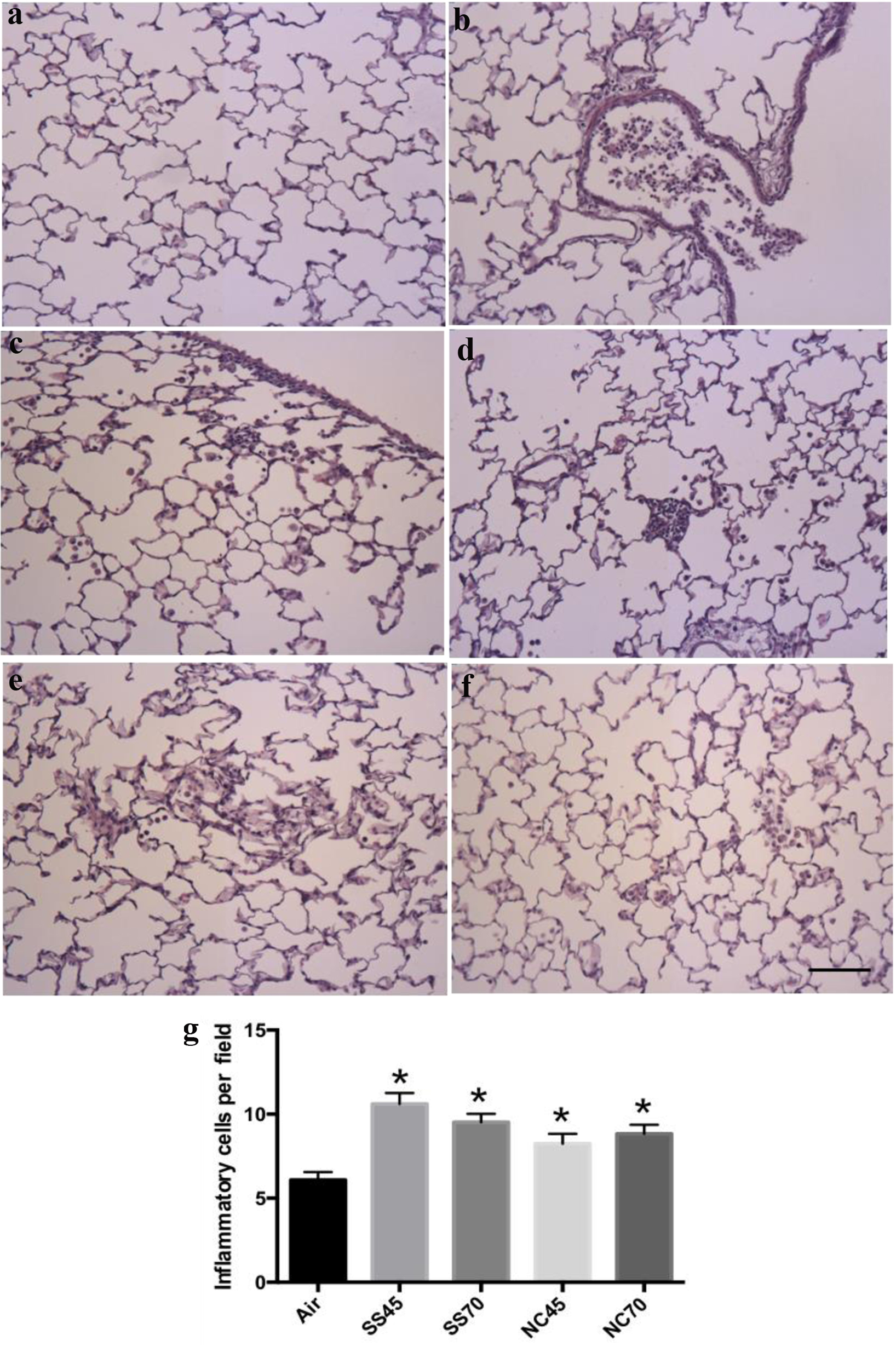 Click for large image | Figure 1. H&E staining of lung sections of rat models. (a) Alveoli from air rat, showing intact epithelial cells and thin alveolar walls. (b) Bronchus from eC exposed rats (SS45) shows accumulation of inflammatory cells in lumen. (c) Alveolar region of eC exposed rats (SS45) shows large accumulation of inflammatory cells near the pleura. (d) Alveolar region of eC exposed rats (SS70) shows accumulation of inflammatory cells. (e) Alveolar region of eC exposed rats (NC45) shows infiltration of inflammatory cells and intra-alveolar fluid. (f) Alveolar region of eC exposed rats (NC70) shows infiltration of inflammatory cells and intra-alveolar fluid (scale bar = 100 µm). (g) The numbers of inflammatory cells per field were significantly greater in the rats exposed to eC using NC or SS heating element compared to the air group (n = 16 in each group, P < 0.05, one-way ANOVA, Tukey test). The result was expressed as means ± SEM. H&E: hematoxylin and eosin; eC: electronic cigarette; SS: stainless steel; NC: nickel-chromium; ANOVA: analysis of variance; SEM: standard error of the mean. *P < 0.05 vs. air. |
Cardiac tissue appeared normal (Fig. 2). There were no architectural changes, inflammation, fibrosis, or necrosis in H&E-stained hearts in any of the groups.
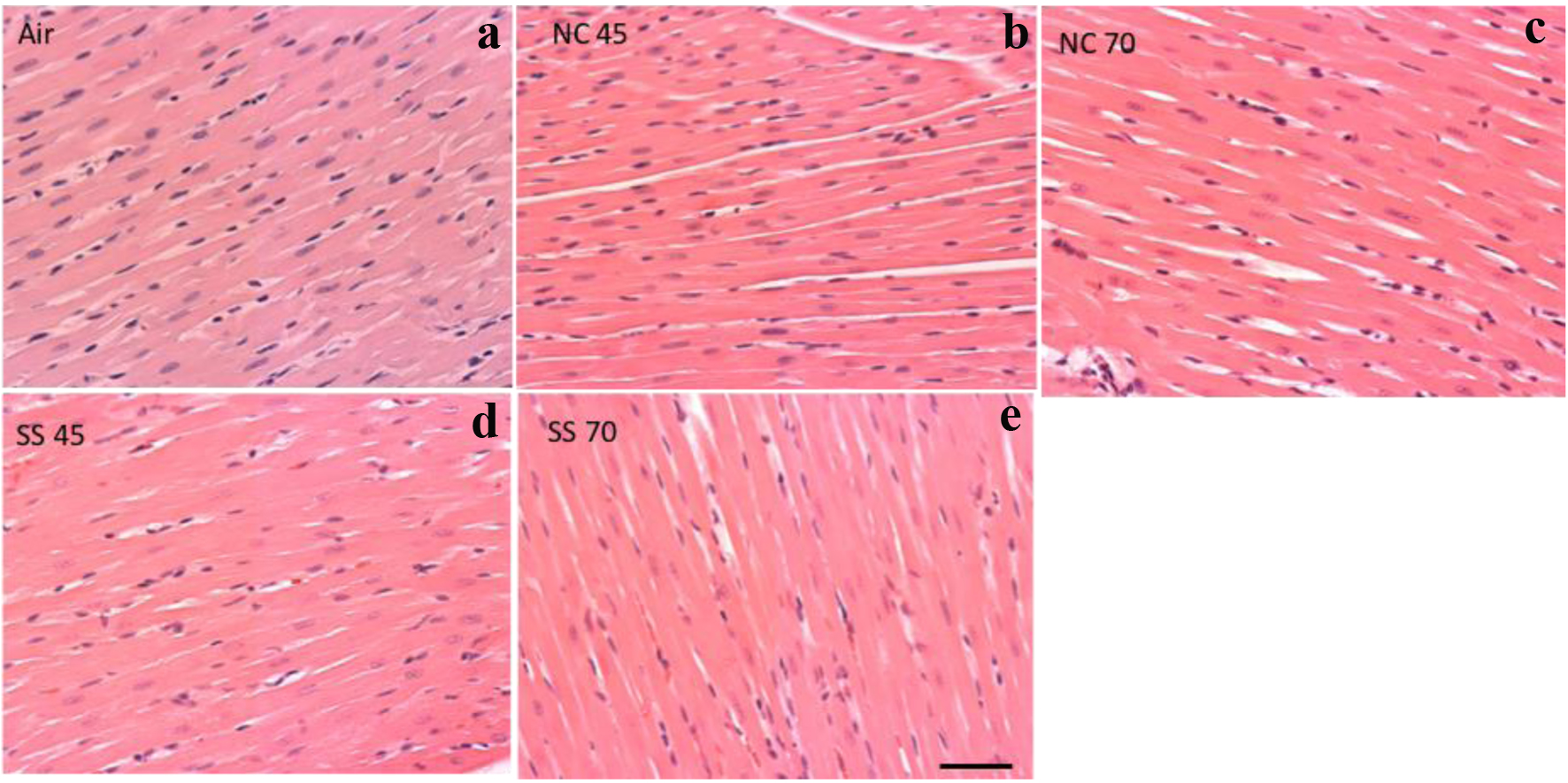 Click for large image | Figure 2. Cardiac tissue in H&E-stained hearts. Representative images of heart in air group (a), NC45 group (b), NC70 group (c), SS45 group (d), and SS70 group (e, scale bar = 50 µm). The heart tissue appears normal in all of these groups. H&E: hematoxylin and eosin; SS: stainless steel; NC: nickel-chromium. |
Lipid-laden macrophage in the lung
We did not detect differences in the presence of lipid-laden macrophages in the lung tissue with oil red O stain among any of the groups (Fig. 3).
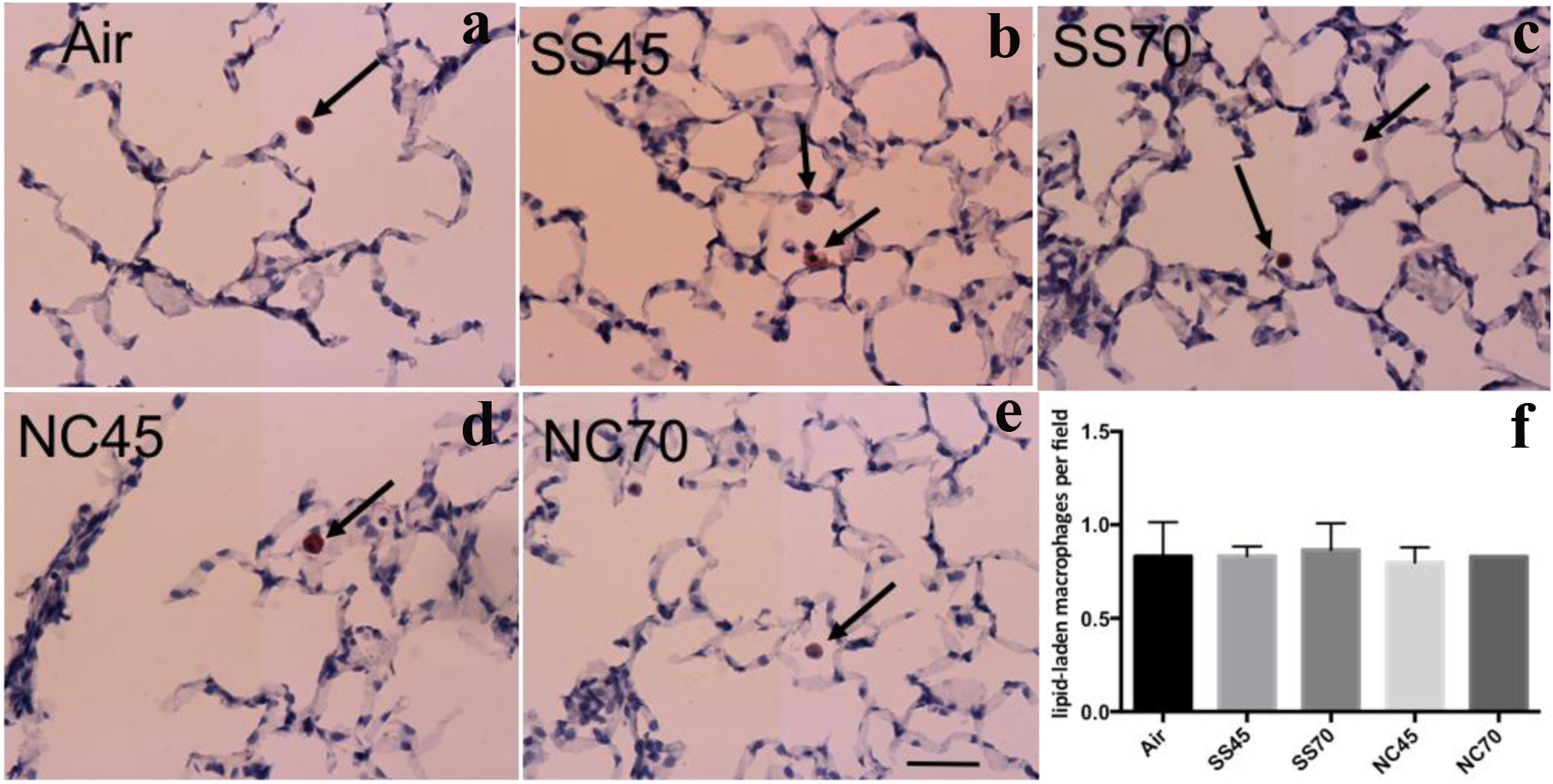 Click for large image | Figure 3. Lipid-laden macrophage in oil red O-stained lung. Representative images of lung: (a) air group, (b) SS45 group, (c) SS70 group, (d) NC45 group, (e) NC70 group and (f) the numbers of lipid-laden macrophage per field. Only occasional scattered, lipid-laden macrophages (red stain) were observed in these groups. There were no differences in the number of lipid-laden macrophage among any of the groups (n = 5 in each group). The result was expressed as means ± SEM. Scale bar = 50 µm. SS: stainless steel; NC: nickel-chromium; SEM: standard error of the mean. |
Inflammatory gene expression
Inflammatory gene expression changes were observed in the lungs of rats assigned to 70 W power (Fig. 4). IL-1β, IL-6, IL-10, IFN-γ and endothelin-1 gene expression were significantly increased in SS70 group versus air group. In NC70 group, IL-6, endothelin-1 and ACE2 gene expression were significantly upregulated compared to the air group. eC exposure had little effect on TNF-α and VCAM-1 expression, but showed a trend toward an increase in the NC70 group versus air. There was no significant difference on gene expression between SS70 and NC70. No significant difference was recorded in rats at the 45 W power.
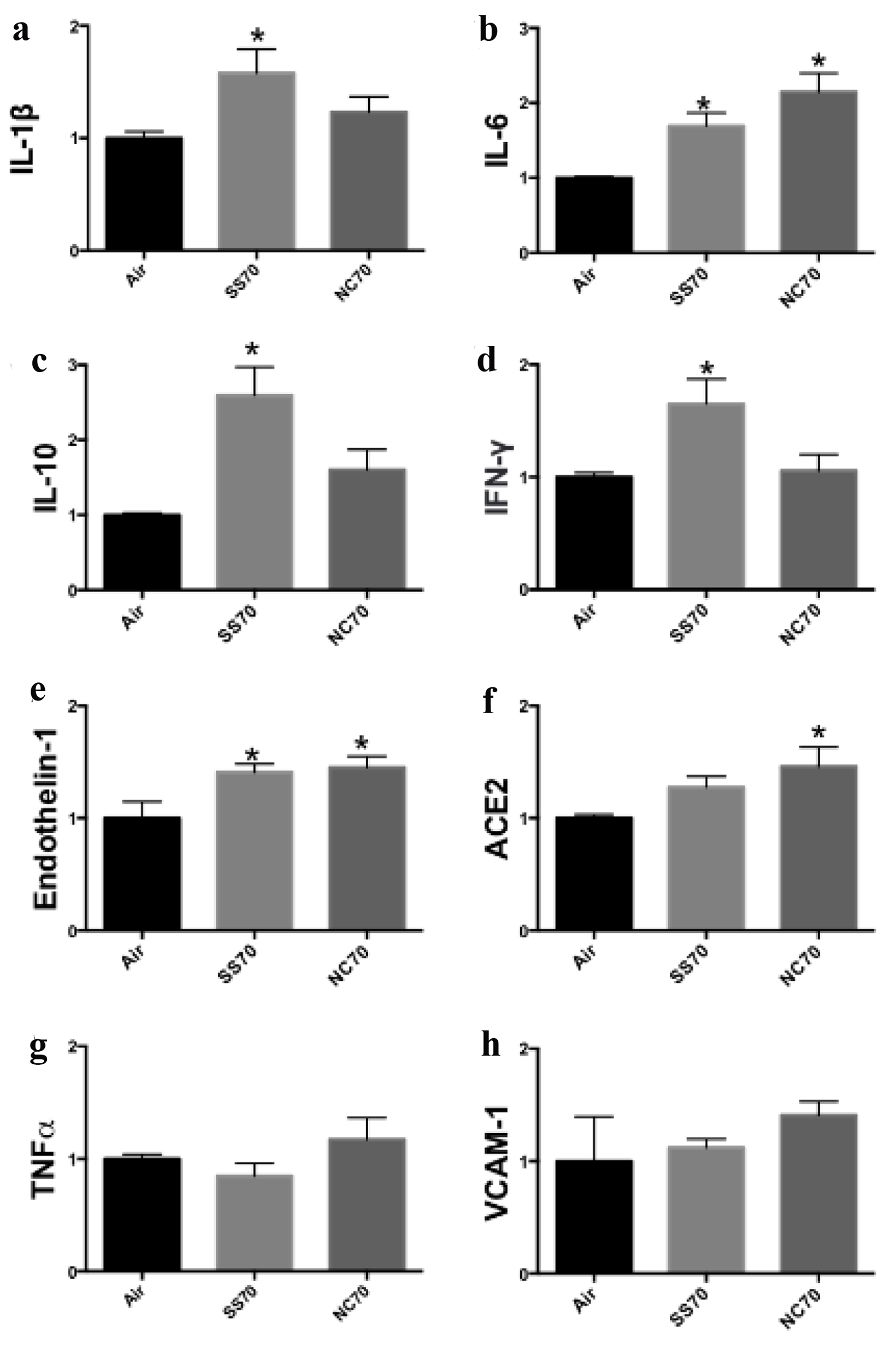 Click for large image | Figure 4. Gene analysis within lung tissue. qRT-PCR analysis (n = 4 to 16 in each group) for (a) IL-1β, (b) IL-6, (c) IL-10, (d) IFN-γ, (e) endothelin-1, (f) ACE2, (g) TNF-α and (h) VCAM-1 inflammatory gene expression in rats assigned to 70 W power. *P < 0.05 vs. air group. All data were normalized to GAPDH. qRT-PCR: quantitative reverse transcriptase polymerase chain reaction; IL: interleukin; IFN-γ: interferon gamma; ACE2: angiotensin converting enzyme 2; TNF-α: tumor necrosis factor-α; VCAM-1: vascular cell adhesion protein-1. |
The effect of burnt coils
Vaping with a burnt coil is reported by some users to be unpleasant and seems to be fairly common [15]. A coil can go bad for a number of reasons, such as, low level of e-liquid in the chamber, high power setting, e-liquid type, manufacture coil defect, frequency of use, and maintenance [7]. We found that the coils aged and oxidized (became burnt) with repeated use.
During the months of March to April 2020, additional rats demonstrated EVALI when exposed to vapor associated with burnt coils. Sixteen rats (these are 16 additional rats) received a nose-only, eC exposure for 4 h (SS heating element, 70 W). The atomizer was found burnt post-exposure. All rats developed clinical acute respiratory distress, characterized by labored mouth breathing, lack of activity and squinted eyes. Eight rats had to be euthanized as per the veterinary staff. Histology was available in two rats exposed to air at the same time and 12 rats exposed using the SS heating element under burnt coil conditions. H&E staining of respiratory system sections is shown in Figure 5a-c. Inflammatory cells were significantly greater in SS heating element with burnt coil compared to the air group (Fig. 5d).
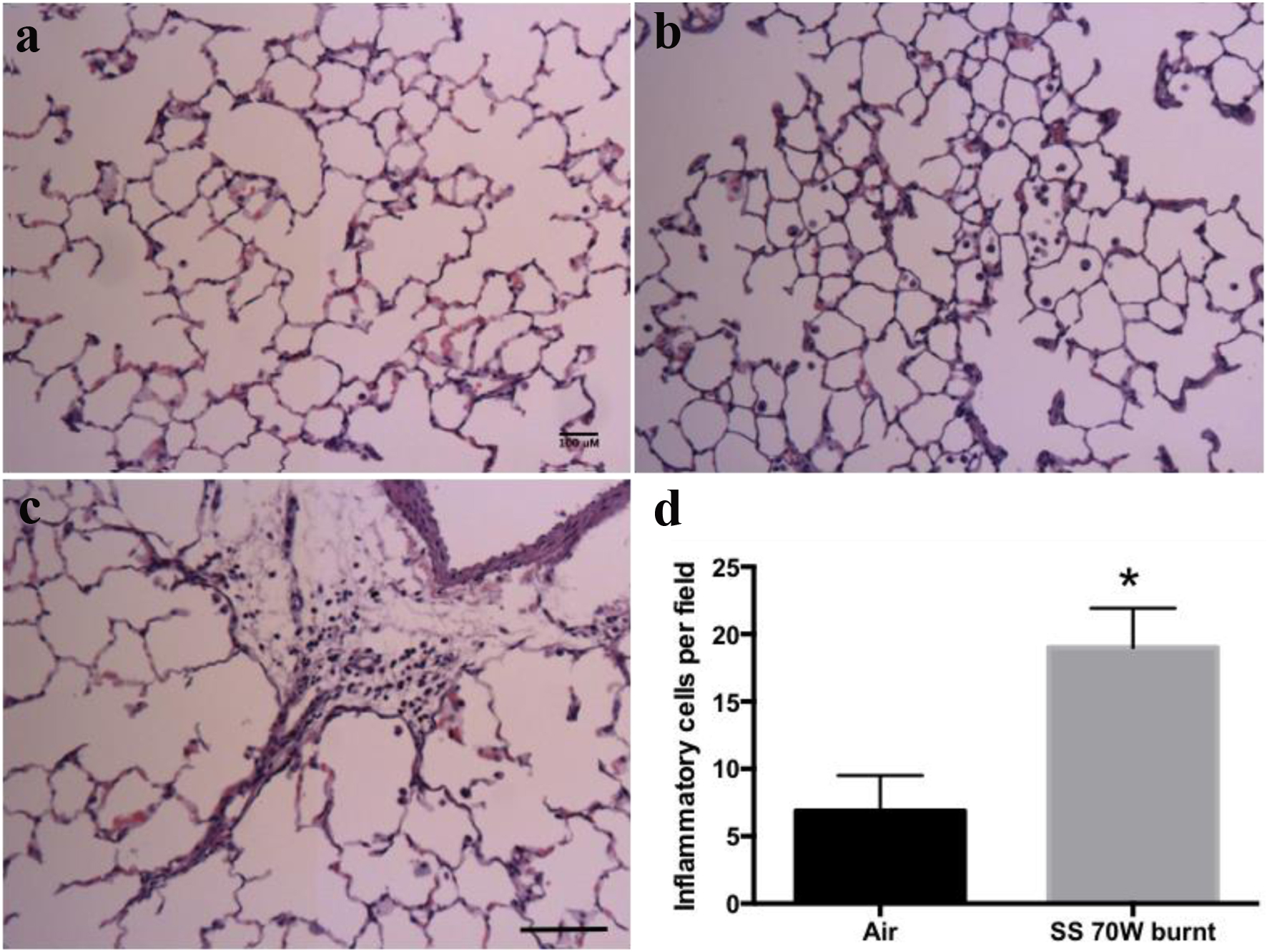 Click for large image | Figure 5. H&E staining of respiratory system sections of burnt coil rat models. (a) Alveoli from air control rat, showing intact epithelial cells and thin alveolar walls. (b) Alveolar region of an eC exposed rat using the SS heating element with a burnt coil showing infiltration of inflammatory cells inside alveoli. (c) An eC exposed rat using the SS heating element with burnt coil showing foci of inflammatory cell including neutrophil infiltration (scale bar = 100 µm). (d) The numbers of inflammatory cells per high power field in the lung parenchyma were significantly greater in the rats exposed to eC using SS heating element with burnt coil (19 ± 2.9, n = 4, randomly chosen) compared to the air group (6.9 ± 3.7, n = 2; P < 0.047). H&E: hematoxylin and eosin; eC: electronic cigarette; SS: stainless steel. |
BAL was performed to collect a fluid sample from these burnt coil rat lungs. Cytology of the BAL was characterized by the predominance of neutrophils in rats exposed to burnt coils, which suggests severe inflammation and active alveolitis (Fig. 6b). Almost all of the cells were macrophages in the air group (Fig. 6a).
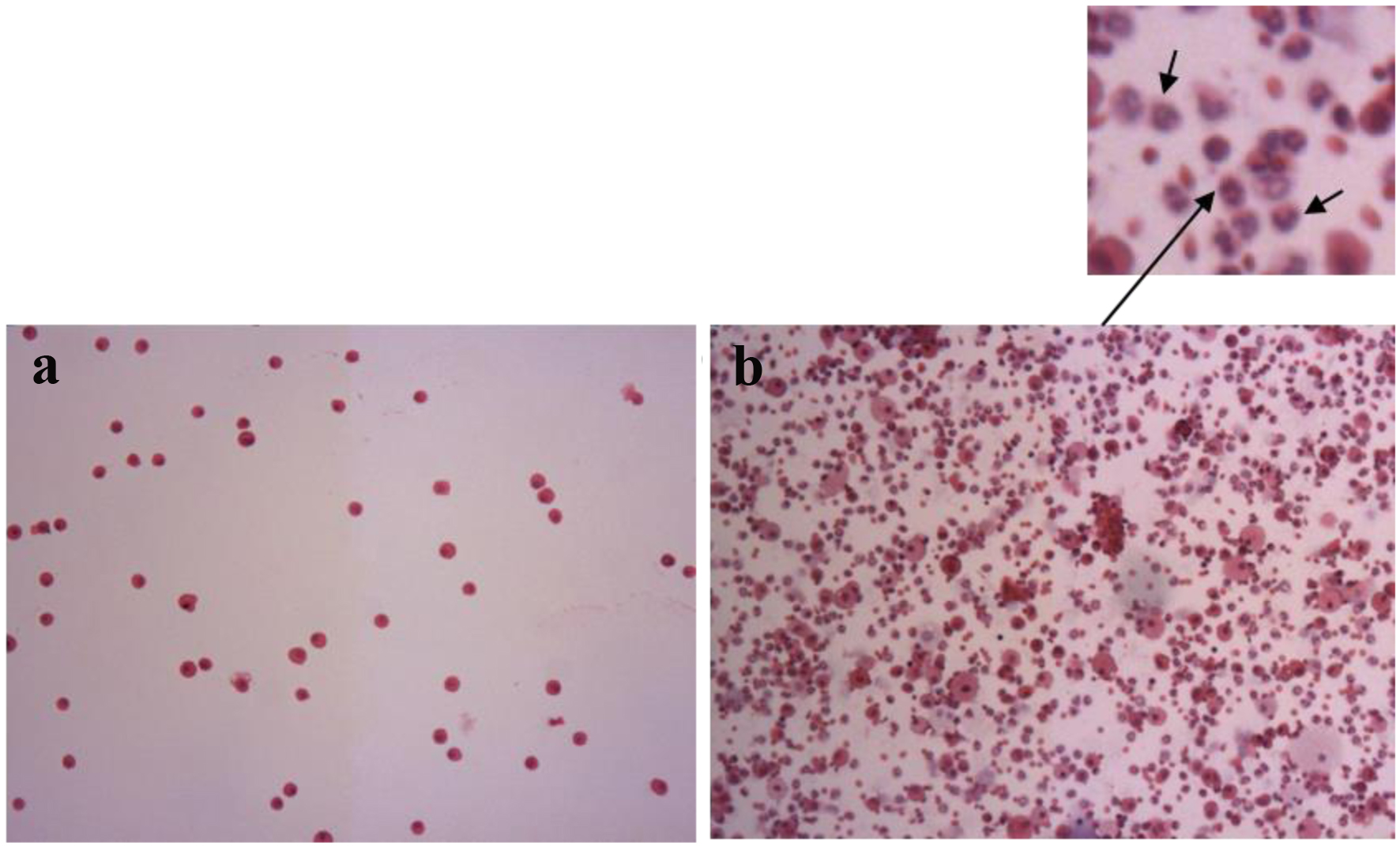 Click for large image | Figure 6. Cytology of bronchoalveolar lavage. Majority of the cells were macrophages in air group (a). The predominance of neutrophils (arrows) was observed in burnt coil rats (b). |
In cardiac tissue of rat from the burnt coil group, foci of inflammatory cellular infiltration and loss of the normal myocardial architecture with marked cellular inflammation were observed (Fig. 7).
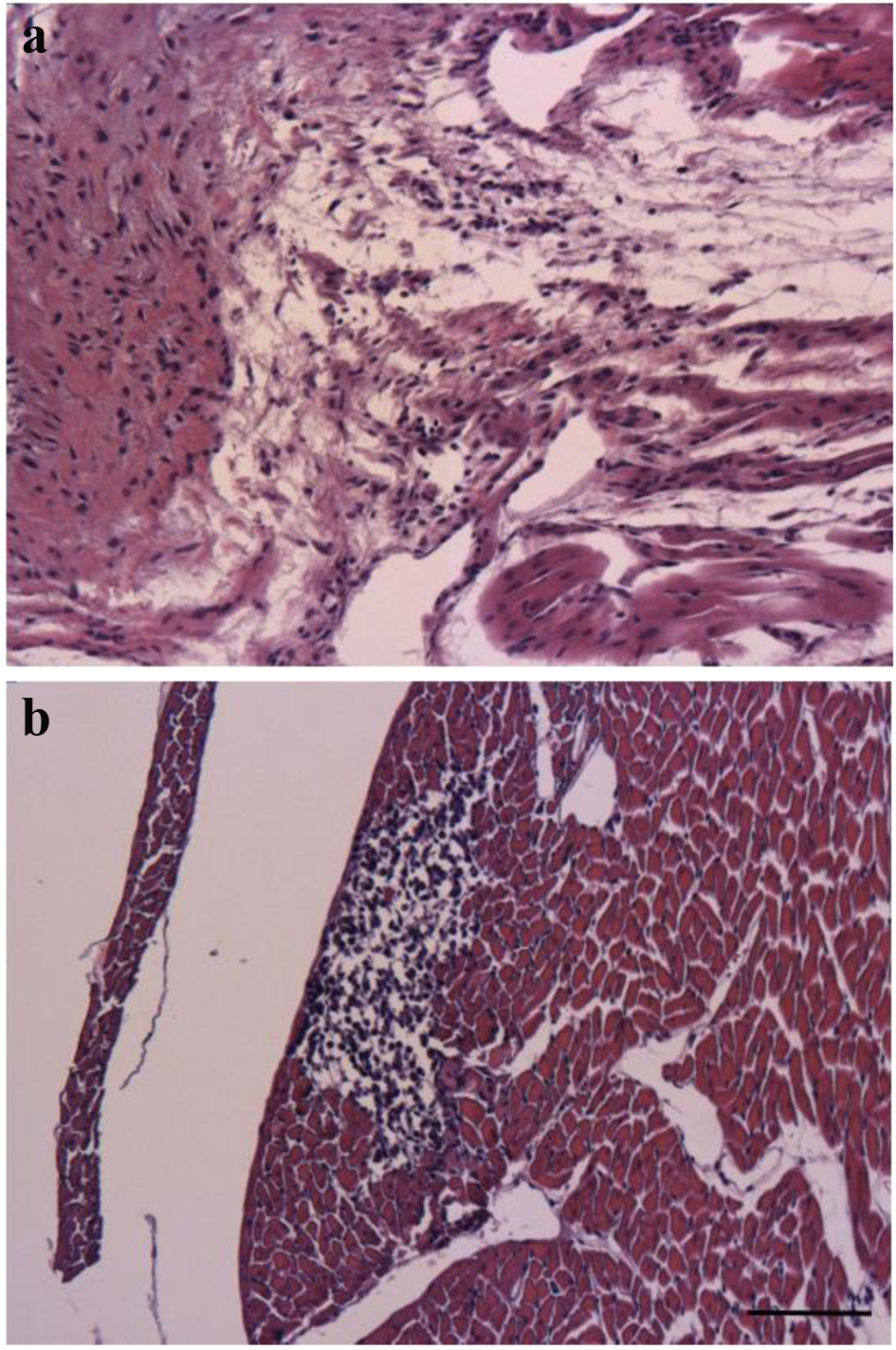 Click for large image | Figure 7. Representative images for the H&E-stained cardiac tissue. (a) Loss of the normal myocardial architecture and inflammatory cellular infiltration. (b) Focal inflammatory area (scale bar = 100 µm). H&E: hematoxylin and eosin. |
| Discussion | ▴Top |
The main finding of the present study was that vaping for only one time (one 4-h exposure to eC vapor) significantly increased the number of inflammatory cells in the lung using SS and NC heating elements at either high or low power, without tetrahydrocannabinol, vitamin E or nicotine. The inflammatory gene expression changes were also identified, but were commonly seen at high power. The burnt coil rats developed acute respiratory distress with significantly greater numbers of inflammatory cells in lung parenchyma and marked cellular inflammation in cardiac tissue.
Other studies have shown that eC aerosol exposure with or without vitamin E, flavoring or nicotine, results in the increased neutrophils, macrophages, lymphocytes, pro-inflammatory cytokines and chemokine secretion, but few have examined the effect of a single exposure in an in vivo model. One study of human tracheobronchial epithelial cells revealed that e-liquid without nicotine increased IL-6 protein levels in a dose-dependent manner at both 24 and 48 h [16]. Leigh et al [17] reported that pro-inflammatory cytokine levels were significantly increased by exposing human bronchial epithelial cells to various eC flavorings. In a murine study [18], vapors produced by eC with flavoring induced inflammatory response in lung epithelial cells and in mouse lung. Cirillo et al reported that heating elements at higher wattage induced a much more robust inflammatory response in rats compared to the heating element at lower wattage [19]. Our finding is in line with these studies and demonstrates that the inflammatory response occurs even after vaping for only one time. Both SS and NC heating elements at high 70 W without flavoring additives elevated inflammatory gene expression.
Recently we reported that some rats exposed using NC heating at high power for 2 h developed clinical acute respiratory distress (labored mouth breathing, lack of activity and audible wheezing) and lung lesion included accumulation of inflammatory cells, red blood cell congestion, obliteration of alveoli and pneumonitis after use of an NC heating element at high power, without the use of vitamin E or nicotine [14]. However, in the present study, none of the rats exposed using SS or NC heating element at low or high power (without burnt coil) developed clinical respiratory distress. Lung inflammatory cells were increased in both SS and NC heating elements at either high or low power. The actual devices used in this study were similar, but not identical to the ones used in our earlier report with respect to manufacture, composition and length of service. These device differences could relate to the “burnt” phenomenon and the differences in outcome severity [15]. Heterogeneity in the manufacturing of these devices, including various designs with little standardization, makes it difficult to predict generation of metal concentrations or other harmful substances even from the same manufacture and the same brand [20]. Heating elements are usually made of SS or NC. Gray et al reported Ni and Cr are present in eC aerosols [21]. Inhalation of these metals can cause chronic bronchitis and lung dysfunction [22]. Elevated levels of metals in these devices may be due to different design or extent of contact between the liquid and metal components. In addition, the liquid levels change over time as substances in the liquid are heated and oxidized and as metal device components in contact with liquid degrade. Heating elements should be monitored throughout the lots as device and liquid changes can affect toxic metal level.
Burnt coils regularly occur while people are vaping [23]. It changes the taste of the vapor, making it taste burnt, and this is often how users know when to replace their atomizers. The atomizers are consumable parts which need to be regularly replaced. The most frequent cause of coil “burn” is when the liquid level is allowed to drop below the wick “window” on the atomizer. It is also possible for the coils to burn even when there is enough liquid in the tank. The coils can run dry when the eC is operated at higher wattages because e-liquid vaporizes faster than the wick can move liquid from the tank to wet the coils. Depending on how severely the coil is burnt and what kind of coil was used can result in the creation of some particles suspended in the vapor that end up being inhaled by the user when they are burned dry. These small particles can be toxic. To our knowledge, this is the first study indicating that the burnt coil caused clinical acute respiratory distress, lung inflammatory cellular infiltration and myocarditis in rats.
A limitation of this study was that we were only able to look at one time point post eC exposure, in part due to funds and manpower available, especially during COVID-19, when labs were partially shuttered. The other limitations were that we do not have an analysis of the chemical composition of the vapor generated by these devices and we have limited resource to run all the studies on every animal.
Conclusion
One 4-h exposure to eC vapor significantly increased the presence of inflammatory cells in the lungs and induced upregulation of inflammatory genes in the lungs. Inflammatory gene stimulation was more prominent at high wattage. Exposure to burnt coils caused respiratory distress and inflammation in both the lung and heart. These findings will guide eC users to be aware that adverse effects can occur even after a one-time vaping episode and cautions about the problems associated with burnt coils.
Acknowledgments
None to declare.
Financial Disclosure
This study was support by NHLBI (R01HL144258 and 3RO1HL-144258-02S1). The effect of electronic cigarettes on young versus old normal hearts and pathologic hearts.
Conflict of Interest
None to declare.
Informed Consent
Informed consents were obtained.
Author Contributions
All authors reviewed the final manuscript. JS conducted the experiments and wrote the manuscript. RAK and MTK designed study and edited manuscript. WD, LZ and JC performed the animal surgery. JC performed the histology staining. RJA, IH, AT, BB and JEMM conducted the experiments and collected animal samples.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Wang TW, Gentzke AS, Neff LJ, Glidden EV, Jamal A, Park-Lee E, Ren C, et al. Characteristics of e-cigarette use behaviors among US youth, 2020. JAMA Netw Open. 2021;4(6):e2111336.
doi pubmed - Park-Lee E, Ren C, Sawdey MD, Gentzke AS, Cornelius M, Jamal A, Cullen KA. Notes from the field: e-cigarette use among middle and high school students - national youth tobacco survey, United States, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(39):1387-1389.
doi pubmed - Jones L. Vaping: how popular are e-cigarettes? In: BBC News. 2019.
- CDC, Youth e-cigarette use is down, but 3.6 million still use e-cigarettes. 2020. https://www.cdc.gov/media/releases/2020/p0909-youth-e-cigarette-use-down.html.
- Results from the Annual National Youth Tobacco Survey/FDA. 2021 Findings on Youth Tobacco Use. https://www.fda.gov/tobacco-products/youth-and-tobacco/results-annual-national-youth-tobacco-survey.
- Caraballo RS, Shafer PR, Patel D, Davis KC, McAfee TA. Quit methods used by US adult cigarette smokers, 2014-2016. Prev Chronic Dis. 2017;14:E32.
doi pubmed - Stratton K, Kwan LY, Eaton DL, editors. National Academies of Sciences Engineering and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on the Review of the Health Effects of Electronic Nicotine Delivery Systems and L.Y.K. Public Health Consequences of E-Cigarettes. Washington (DC): National Academies Press (US); 2018.
doi - Heinzerling A, Armatas C, Karmarkar E, Attfield K, Guo W, Wang Y, Vrdoljak G, et al. Severe lung injury associated with use of e-cigarette, or vaping, products-California, 2019. JAMA Intern Med. 2020;180(6):861-869.
doi pubmed - Salzman GA, Alqawasma M, Asad H. Vaping Associated Lung Injury (EVALI): an explosive United States epidemic. Mo Med. 2019;116(6):492-496.
- Belok SH, Parikh R, Bernardo J, Kathuria H. E-cigarette, or vaping, product use-associated lung injury: a review. Pneumonia (Nathan). 2020;12:12.
doi pubmed - Guerrini V, Panettieri RA, Jr., Gennaro ML. Lipid-laden macrophages as biomarkers of vaping-associated lung injury. Lancet Respir Med. 2020;8(2):e6.
doi - Maddock SD, Cirulis MM, Callahan SJ, Keenan LM, Pirozzi CS, Raman SM, Aberegg SK. Pulmonary lipid-laden macrophages and vaping. N Engl J Med. 2019;381(15):1488-1489.
doi pubmed - Blount BC, Karwowski MP, Shields PG, Morel-Espinosa M, Valentin-Blasini L, Gardner M, Braselton M, et al. Vitamin E acetate in bronchoalveolar-lavage fluid associated with EVALI. N Engl J Med. 2020;382(8):697-705.
doi pubmed - Kleinman MT, Arechavala RJ, Herman D, Shi J, Hasen I, Ting A, Dai W, et al. E-cigarette or vaping product use-associated lung injury produced in an animal model from electronic cigarette vapor exposure without tetrahydrocannabinol or vitamin E oil. J Am Heart Assoc. 2020;9(18):e017368.
doi pubmed - Wagner J, Chen W, Vrdoljak G. Vaping cartridge heating element compositions and evidence of high temperatures. PLoS One. 2020;15(10):e0240613.
doi pubmed - Wu Q, Jiang D, Minor M, Chu HW. Electronic cigarette liquid increases inflammation and virus infection in primary human airway epithelial cells. PLoS One. 2014;9(9):e108342.
doi pubmed - Leigh NJ, Lawton RI, Hershberger PA, Goniewicz ML. Flavourings significantly affect inhalation toxicity of aerosol generated from electronic nicotine delivery systems (ENDS). Tob Control. 2016;25(Suppl 2):ii81-ii87.
doi pubmed - Lerner CA, Sundar IK, Yao H, Gerloff J, Ossip DJ, McIntosh S, Robinson R, et al. Vapors produced by electronic cigarettes and e-juices with flavorings induce toxicity, oxidative stress, and inflammatory response in lung epithelial cells and in mouse lung. PLoS One. 2015;10(2):e0116732.
doi pubmed - Cirillo S, Vivarelli F, Turrini E, Fimognari C, Burattini S, Falcieri E, Rocchi MBL, et al. The customizable e-cigarette resistance influences toxicological outcomes: lung degeneration, inflammation and oxidative stress-induced in a rat model. Toxicol Sci. 2019;172(1):132-145.
doi pubmed - Papaefstathiou E, Stylianou M, Agapiou A. Main and side stream effects of electronic cigarettes. J Environ Manage. 2019;238:10-17.
doi pubmed - Gray N, Halstead M, Gonzalez-Jimenez N, Valentin-Blasini L, Watson C, Pappas RS. Analysis of toxic metals in liquid from electronic cigarettes. Int J Environ Res Public Health. 2019;16(22):4450.
doi pubmed - Traboulsi H, Cherian M, Abou Rjeili M, Preteroti M, Bourbeau J, Smith BM, Eidelman DH, et al. Inhalation toxicology of vaping products and implications for pulmonary health. Int J Mol Sci. 2020;21(10):3495.
doi pubmed - Visser WF, Krusemann EJZ, Klerx WNM, Boer K, Weibolt N, Talhout R. Improving the analysis of E-cigarette emissions: detecting human "Dry Puff" conditions in a laboratory as validated by a panel of experienced vapers. Int J Environ Res Public Health. 2021;18(21):11520.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.