

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 13, Number 6, December 2022, pages 357-371

High Prevalence of Cardiac Amyloidosis in Clinically Significant Aortic Stenosis: A Meta-Analysis
Samiullah Arshada, f ![]() , Ythan H. Goldbergb, Huzefa Bhopalwalac, Nakeya Dewaswalad, Nicholas S. Micelie, Emma J. Birksd, Gaurang N. Vaidyad
, Ythan H. Goldbergb, Huzefa Bhopalwalac, Nakeya Dewaswalad, Nicholas S. Micelie, Emma J. Birksd, Gaurang N. Vaidyad
aDepartment of Medicine, University of Kentucky, Lexington, KY, USA
bDivision of Cardiology, Montefiore Medical Center, Bronx, NY, USA
cDepartment of Medicine, Appalachian Regional Healthcare, Whitesburg, KY, USA
dDivision of Cardiology (Advanced Heart Failure and Transplantation), Gill Heart and Vascular Institute, University of Kentucky, Lexington KY, USA
eCollege of Management, School of Business, Park University, Parkville, MO, USA
fCorresponding Author: Samiullah Arshad, Department of Medicine, University of Kentucky, Lexington, KY, USA
Manuscript submitted September 11, 2022, accepted October 28, 2022, published online December 1, 2022
Short title: AS-CA Prevalence and Mortality
doi: https://doi.org/10.14740/cr1436
| Abstract | ▴Top |
Background: There is growing evidence of coexistence of aortic stenosis (AS) and transthyretin cardiac amyloidosis (CA). Not screening AS patients at the time of hospital/clinic visit for CA represents a lost opportunity.
Methods: We surveyed studies that reported the prevalence of CA among AS patients. Studies that compared patients with aortic stenosis with cardiac amyloidosis (AS-CA) and AS alone were further analyzed, and meta-regression was performed.
Results: We identified nine studies with 1,321 patients of AS, of which 131 patients had concomitant CA, with a prevalence of 11%. When compared to AS-alone, the patients with AS-CA were older, more likely to be males, had higher prevalence of carpal tunnel syndrome, right bundle branch block. On echocardiogram, patients with AS-CA had thicker interventricular septum, higher left ventricular mass index (LVMI), lower myocardial contraction fraction, and lower stroke volume index. Classical low-flow low-gradient (LFLG) physiology was more common among patients with AS-CA. Patients with AS-CA had higher all-cause mortality than patients with AS alone (33% vs. 22%, P = 0.02) in a follow-up period of at least 1 year.
Conclusions: CA has a high prevalence in patients with AS and is associated with worse clinical, imaging, and biochemical parameters than patients with AS alone.
Keywords: Aortic stenosis; Cardiac amyloidosis; Prevalence; Mortality; Imaging characteristics; Clinical features
| Introduction | ▴Top |
Cardiac amyloidosis (CA) is characterized by infiltrative restrictive cardiomyopathy which is associated with a high mortality [1]. It can most commonly be present in the setting of plasma cell disorders (light chain or AL amyloidosis), or due to a genetic or translational defect in transthyretin gene (mutant or wild type, respectively), resulting in deposition of fibrils composed predominantly of misfolded transthyretin (ATTR) monomers in the cardiac tissue. The recent advancement and relatively wider availability in diagnostic techniques have resulted in greater identification of underlying amyloidosis as the etiology of heart failure, especially among patients with heart failure with preserved ejection fraction (HFpEF). The ATTR-ACT trial showed treatment of ATTR amyloid cardiomyopathy with tafamidis results in lower all-cause mortality as well as cardiovascular related complications and improvement in functional status [2]. This is in addition to other Food and Drug Administration (FDA)-approved medications such as patisiran and inotersen for hereditary ATTR amyloidosis with polyneuropathy [3, 4]. The availability of effective treatment options makes screening high-risk patients imperative.
One such high-risk cohort is patients with significant aortic stenosis (AS), who are increasingly recognized to have underlying transthyretin cardiac amyloidosis (ATTR-CA). Coincident ATTR-CA in patients with significant AS (AS-CA) could potentially interfere with long-term prognosis of the planned intervention for AS. The patients with AS often come in contact with medical care while undergoing evaluations for transcatheter aortic valve replacement (TAVR) or surgical aortic valve replacement (SAVR). Not screening them for ATTR-CA during this time could represent a lost opportunity to identify a potentially fatal disease, which possibly portends a worse prognosis independent of the underlying AS.
We sought to analyze literature for the prevalence of ATTR-CA among patients with clinically significant AS referred for TAVR/SAVR and support a routine screening protocol to identify AS patients at high-risk for underlying CA.
| Materials and Methods | ▴Top |
Data source and search strategy
A review of literature was performed in accordance with the preferred reporting items for systematic reviews and meta-analyses guidelines. No ethical approval was obtained, as data were retrieved from already published literature. A search was performed in PubMed, EMBASE, Cochrane Central and clinicaltrials.gov, without any language restrictions, from inception to November 2021. Two authors (SA, NM) independently reviewed each article for eligibility for inclusion in the review. The two above authors extracted data from the studies selected for the review. Disagreements were resolved by senior author (GV). The study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration.
A literature search was conducted using terms “cardiac amyloidosis”, “ATTR-CA”, “ATTR-wt”, “wild type transthyretin”, “aortic stenosis” and “AS”. Search terms were devised using wildcards to account for variation in the spellings. Retrieved articles were screened to identify CA cohort. References in the review articles were screened for potential articles with the above cohort. Criteria for inclusion included: studies with cohort of patients with AS and CA, and AS alone, and comparison of the two cohorts in the study.
Data extraction
Two investigators (SA, NM) reviewed and extracted prevalence of AS-CA in each study. Among the studies that compared AS-CA with AS-alone cohorts, demographic data, electrocardiogram findings, echocardiographic features were extracted for both patients with AS-CA and AS alone. An attempt was also made to gather the non-reported data by contacting the corresponding authors via email, however no response was obtained.
Quality assessment and risk of bias in studies
The quality of the studies was independently assessed by two authors (SA, GV) using the Newcastle Ottawa quality assessment scale for cohort studies [5]. Each study was judged based on 1) patient selection; 2) comparability; and 3) outcomes. Studies were appraised by adding stars in each domain: three or four stars for selection, one or two stars for comparability, and two or three stars for the outcome domain signified “good” quality; two stars for selection, one or two stars for comparability, and two or three stars for outcomes reflected “fair” quality; and zero or one star for selection, or zero star for comparability, or zero or one stars for the outcome domain denoted “poor” quality. Risk of bias was assessed by Robvis tool [6].
Statistical analysis
A meta-analysis was performed for the primary and secondary outcomes using the Review Manager (RevMan) software, Version 5.4, The Cochrane Collaboration, 2020. Dichotomous variables were assessed using the Mantel-Haenszel statistical method and measured in odds ratios (ORs). The difference in continuous variables was evaluated by the inverse variance (IV) statistical method and measured in mean difference (MD) and standard mean difference (SMD). When means and standard deviation were not provided, medians and interquartile range were converted to mean and standard deviation [7]. The random-effects model was preferred over the fixed-effects model as we suspected that clinical heterogeneity might be present due to the variability across the included studies regarding differences in patient population characteristics and diagnosis of CA. Statistical heterogeneity among studies was assessed using the I2 statistic. I2 statistics greater than 50% were considered indicative of the presence of substantial heterogeneity. A P value of < 0.05 was considered statistically significant. A meta-regression analysis was conducted to further assess parameters that signified the diagnosis of CA in patients with AS. Publication bias was assessed using funnel plots and Egger’s test. The rank correlation test and the regression test, using the standard error of the observed outcomes as predictor, were used to check for funnel plot asymmetry.
| Results | ▴Top |
Initial search yielded 304 manuscripts. After reviewing their abstracts, 22 manuscripts were reviewed in full text (Fig. 1). From them, we identified nine studies [8-16] with a total of 1,321 patients with AS, of which 139 patients had concomitant CA (AS-CA), yielding a pooled prevalence of 11% (Table 1) [8-16]. Five studies [8-12] that compared the AS-CA patients with AS alone patients were selected for the meta-analysis to compare the two cohorts. Six studies [8, 9, 11-14] were used to compare all-cause mortality. Remaining studies were excluded from analysis as comparison between the study cohorts was not provided or there was inconsistent reporting of data.
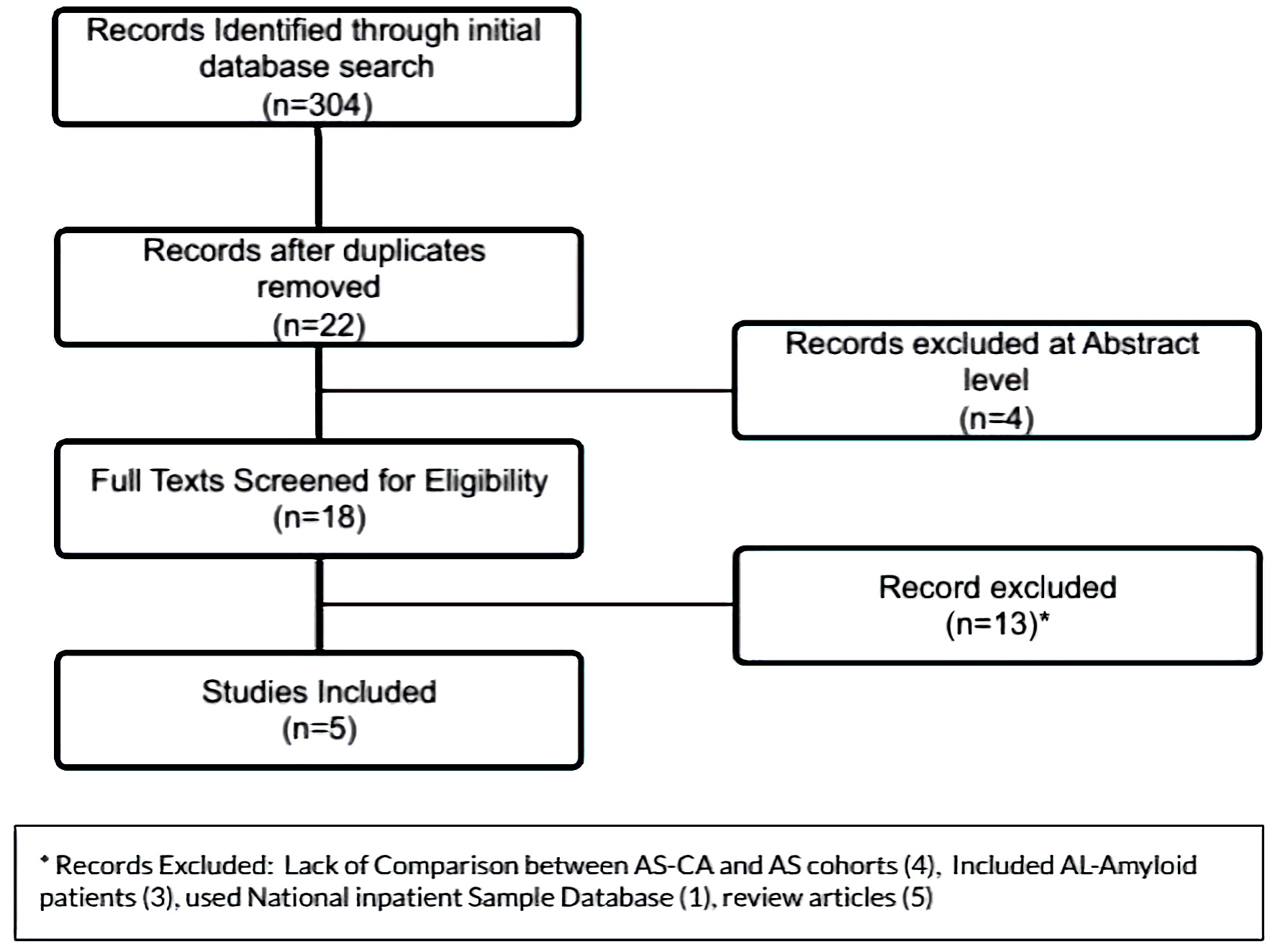 Click for large image | Figure 1. PRISMA flowsheet for inclusion of manuscripts in the meta-analysis. PRISMA: the preferred reporting items for systematic reviews and meta-analyses. |
 Click to view | Table 1. Prevalence of Cardiac Amyloidosis in Patients With Aortic Stenosis Reported in Nine Studies |
Characteristics of studies are highlighted in Table 2 [8-12]. Four prospective cohort studies [8-11] and one retrospective study [12] was included in the meta-analysis. These studies were conducted in USA, UK, Vienna, and India. The quality of these studies was judged to be fair (Table 3) [8-12], but there was significant heterogeneity in the report data among the studies. The risk of bias among the studies was low to moderate (Fig. 2).
Click to view | Table 2. Characteristics of Studies Included in the Review |
Click to view | Table 3. Quality Assessment of Studies by the Newcastle Ottawa Scale for Cohort Studies |
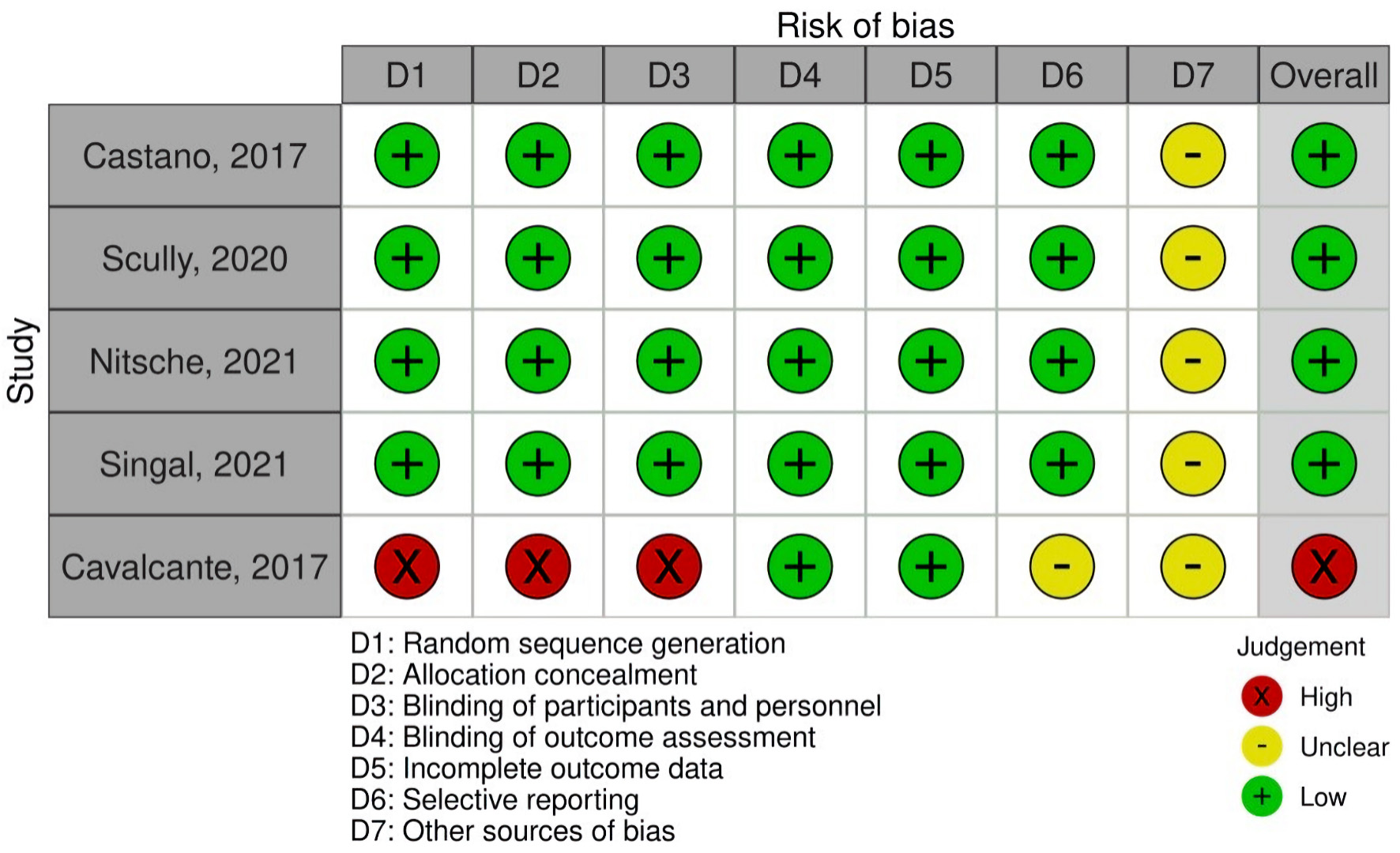 Click for large image | Figure 2. Risk of bias assessment with Robvis tool. |
Clinical characteristics
Demographics of patients are summarized in Table 4 [8-12]. The patients with AS-CA were older (mean 84.4 years vs. 77.7 years, MD 6.53 (2.3 - 10.7), P < 0.0001) (Fig. 3a) and predominantly males (72.3% vs. 52.4%, OR 2.2 (1 - 4.84), P = 0.05) (Fig. 3b) compared to patients with AS alone. Patients with AS-CA had higher prevalence of carpal tunnel syndrome (CTS) (17.8% vs. 2.2%, OR 8.36 (1.42 - 49.26), P = 0.02) and right bundle branch block (RBBB) (27.1% vs. 10.4%, OR 3 (1.74, 5.17), P < 0.001) (Fig. 3c). Patients with AS-CA had worse performance on the 6-min walk test (6MWT) (mean distance 127 m vs. 171 m, MD -48.71 (-87.71, -9.32), P = 0.02) (Fig. 3d). No statistical difference in pacemaker requirement, or presence of atrial fibrillation/flutter was observed between the two groups.
Click to view | Table 4. Patient Demographics |
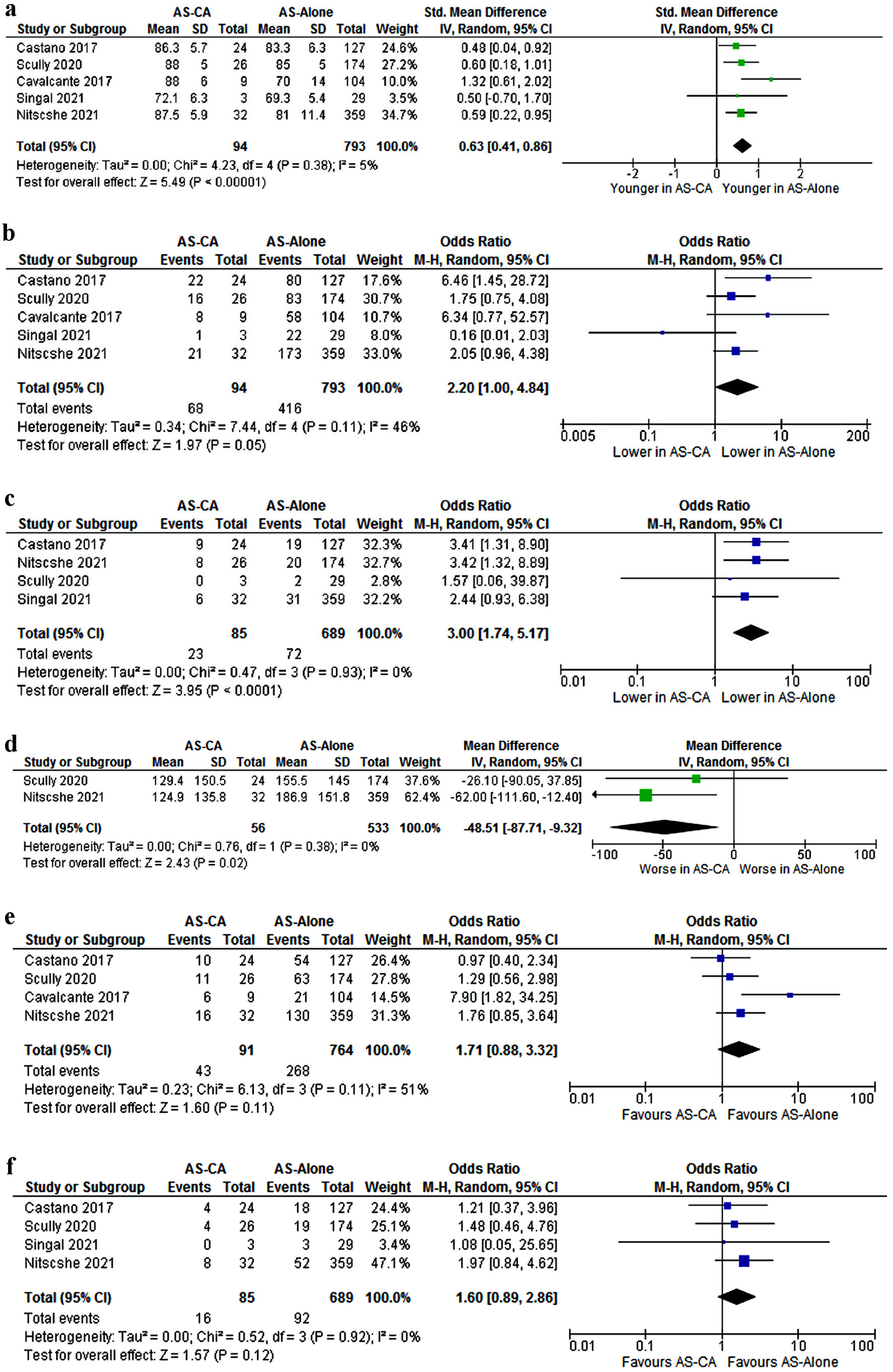 Click for large image | Figure 3. Comparison of (a) Age; (b) Males; (c) RBBB; (d) 6MWT; (e) Atrial fibrillation/flutter; (f) Pacemaker requirement. CI: confidence interval; AS-CA: aortic stenosis with cardiac amyloidosis; AS-alone: aortic stenosis. |
Imaging characteristics
Myocardial contraction fraction (MCF) was lower in patients with AS-CA compared to AS-alone (mean 21.15% vs. 32.5%, MD -10.38 (-15.7, -5.04), P < 0.001) (Fig. 4a). Similarly, the stroke volume index (SVI) was lower in patients with AS-CA (mean 33.1 vs. 39.3, MD -5.4 (-7.9, -2.9) P < 0.001) (Fig. 4b). Among patients with AS-CA, the interventricular septum (IVS) was thicker (1.5 vs. 1.3 cm, MD = 0.16 (0.06, 0.26), P = 0.002), left atrial (LA) diameter was larger (4.9 vs. 4.5 cm, MD 0.42 (0.22, 0.62), P < 0.0001), left ventricular mass index (LVMI) was higher (129.8 vs. 103.8 g/m2, MD 25.8 (18.1, 33.6), P < 0.001) (Fig. 4c) compared to patients with AS alone.
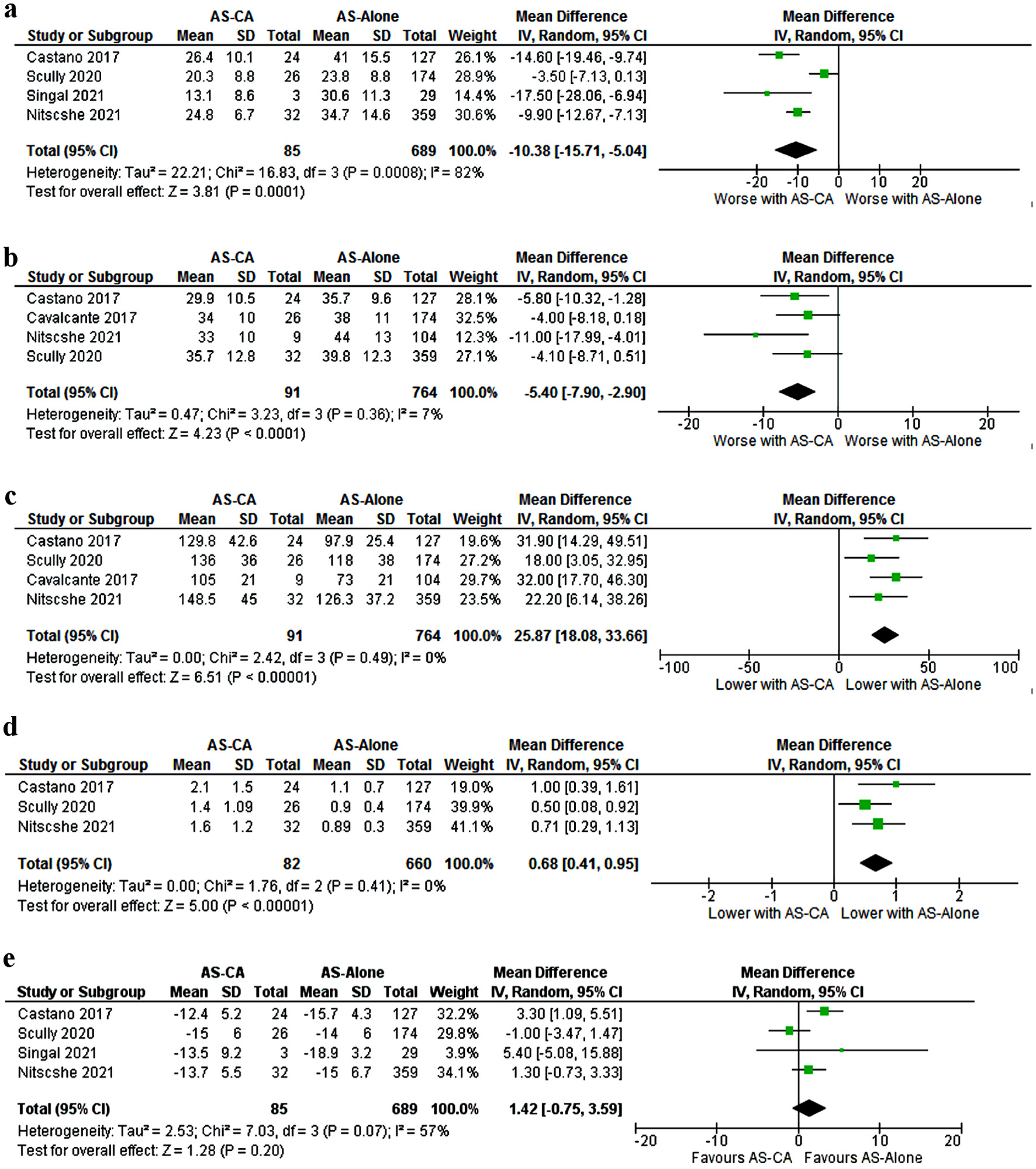 Click for large image | Figure 4. Comparison of: (a) MCF; (b) SVI; (c) LVMI; (d) E/A ratio; (e) Global longitudinal strain. MCF: myocardial contraction fraction; SVI: stroke volume index; LVMI: left ventricular mass index; CI: confidence interval; AS-CA: aortic stenosis with cardiac amyloidosis; AS-alone: aortic stenosis. |
Patients with AS-CA had a higher E/A ratio compared to AS-alone patients (mean 1.7 vs. 0.9, MD 0.68 (0.4, 0.9), P < 0.00001) (Fig. 4d). Mitral annular S’ was consistently < 6 among patients with AS-CA compared to patients with AS alone (mean 4.5 vs. 6.3 cm/s, MD -1.8 (-3.3, -0.23), P = 0.02).
Among patients with AS-CA, aortic valve peak velocity was lower (mean 3.9 vs. 4.2 m/s, MD -0.26 (-0.45, -0.07), P = 0.006) and the mean pressure gradient was lower (mean 38.2 vs. 42.8 mm Hg, MD -4 (-7.28, -0.72), P = 0.02) (Fig. 5a) compared to AS-alone. Classical low-flow low-gradient (LFLG) physiology was seen more commonly among patients with AS-CA (23.5% vs. 12.8%, OR 2.44 (1.2, 4.94) P = 0.01) (Fig. 5b). No significant difference was found in the left ventricular ejection fraction (LVEF), global longitudinal strain, and paradoxical LFLG physiology. Publication bias was only significant for E/A ratio and LVMI (Fig. 6).
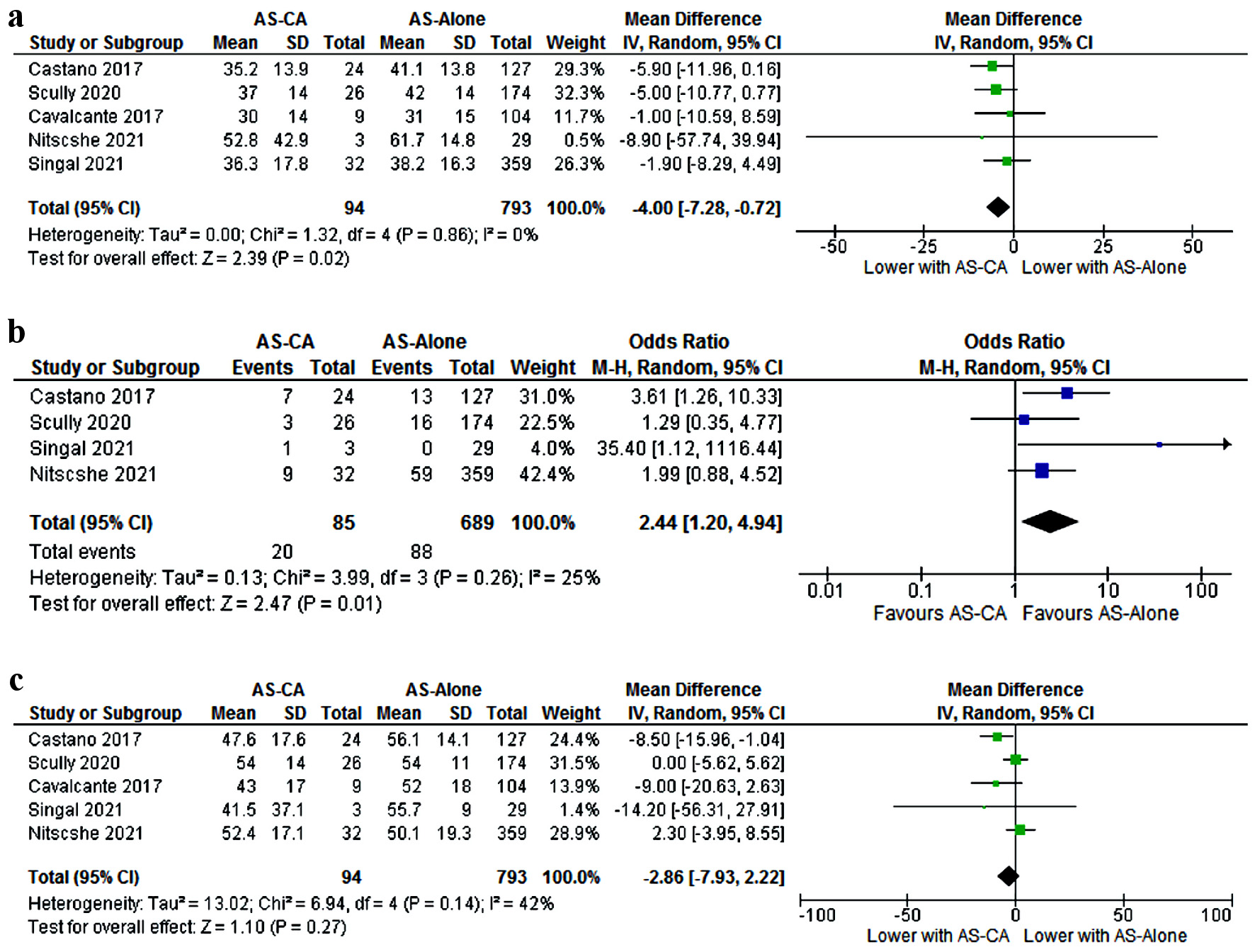 Click for large image | Figure 5. Comparison of: (a) Aortic valve (AV) mean pressure gradient; (b) Low-flow low-gradient (LFLG) physiology; (c) Left ventricular ejection fraction. CI: confidence interval; AS-CA: aortic stenosis with cardiac amyloidosis; AS-alone: aortic stenosis. |
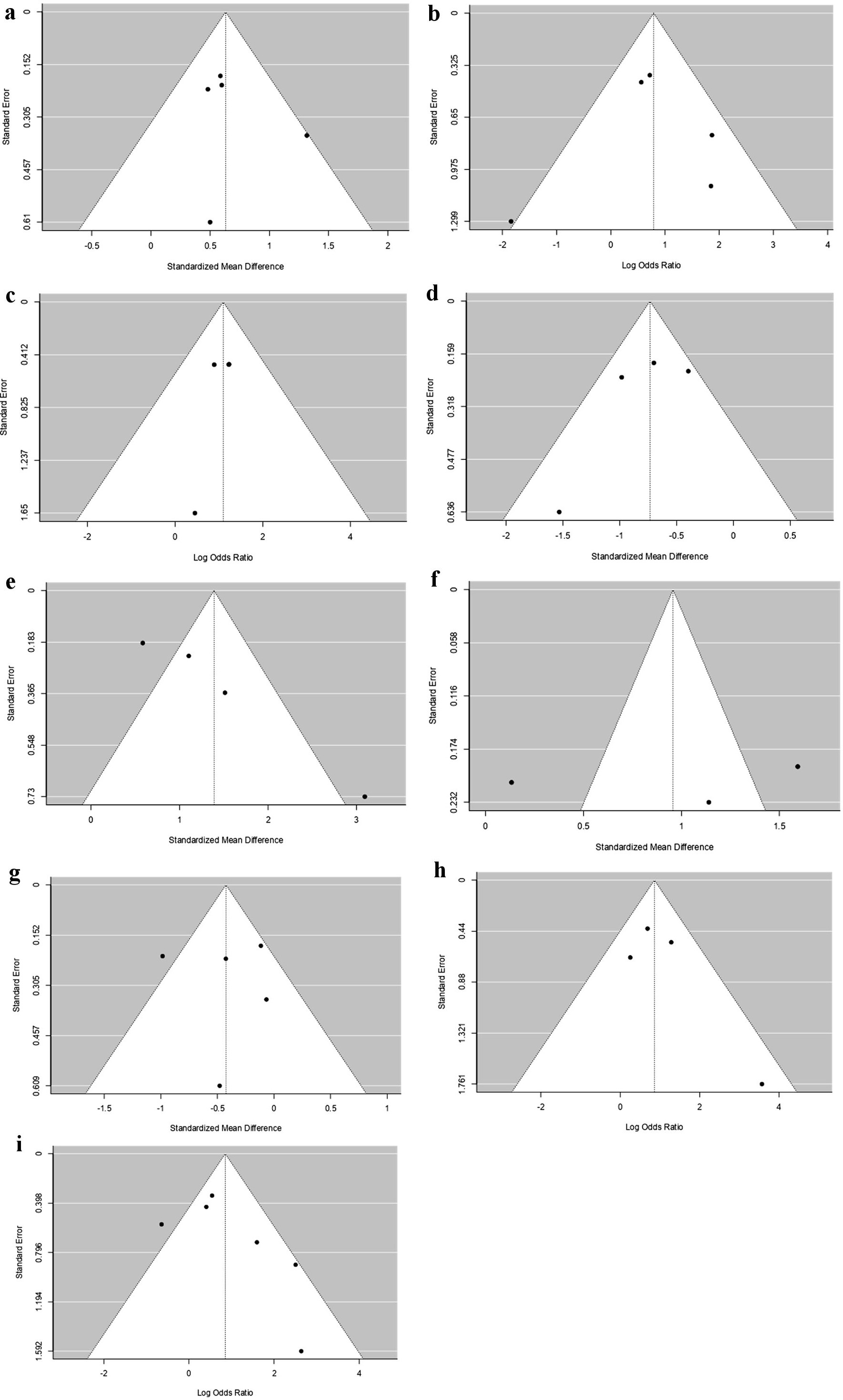 Click for large image | Figure 6. Funnel plots for analysis of publication bias: (a) Age; (b) Males; (c) RBBB; (d) MCF; (e) LVMI; (f) E/A ratio; (g) Aortic valve (AV) mean pressure gradient; (h) LFLG; (i) All-cause mortality. (a) Age. Neither the rank correlation nor the regression test indicated any funnel plot asymmetry (P = 0.8167, and P = 0.4964, respectively). (b) Males. Neither the rank correlation nor the regression test indicated any funnel plot asymmetry (P = 0.8167, and P = 0.6694, respectively). (c) RBBB. Neither the rank correlation nor the regression test indicated any funnel plot asymmetry (P = 0.3333, and P = 0.6889, respectively). (d) MCF. Neither the rank correlation nor the regression test indicated any funnel plot asymmetry (P = 0.7500, and P = 0.1826, respectively). (e) LVMI. The regression test indicated funnel plot asymmetry (P = 0.0002) but not the rank correlation test (P = 0.0833). (f) E/A ratio. Neither the rank correlation nor the regression test indicated any funnel plot asymmetry (P = 1.0000 and P = 0.8009, respectively). (g) AV mean pressure gradient. Neither the rank correlation nor the regression test indicated any funnel plot asymmetry (P = 0.8167 and P = 0.8845, respectively). (h) LFLG. Neither the rank correlation nor the regression test indicated any funnel plot asymmetry (P = 0.7500 and P = 0.1948, respectively). (i) All-cause mortality. Neither the rank correlation nor the regression test indicated any funnel plot asymmetry (P = 0.4694 and P = 0.0654, respectively). NT-proBNP: N-terminal pro-brain natriuretic peptide; LVMI: left ventricular mass index; LFLG: low-flow low-gradient; RBBB: right bundle branch block; MCF: myocardial contraction fraction. |
Cardiac biomarkers
Patients with AS-CA had higher levels of high-sensitivity cardiac troponin (hsTNT) (mean 53.7 vs. 24.6 ng/L, MD 29.4 (18.1 - 40.7), P < 0.0001) (Fig. 7a) and higher N-terminal pro-brain natriuretic peptide (NT-proBNP) levels (mean 4,047.4 vs 1,803.5 ng/L, MD 2,185.3 (1,148.6, 3,221.9), P < 0.0001) (Fig. 7b) than patients with AS alone.
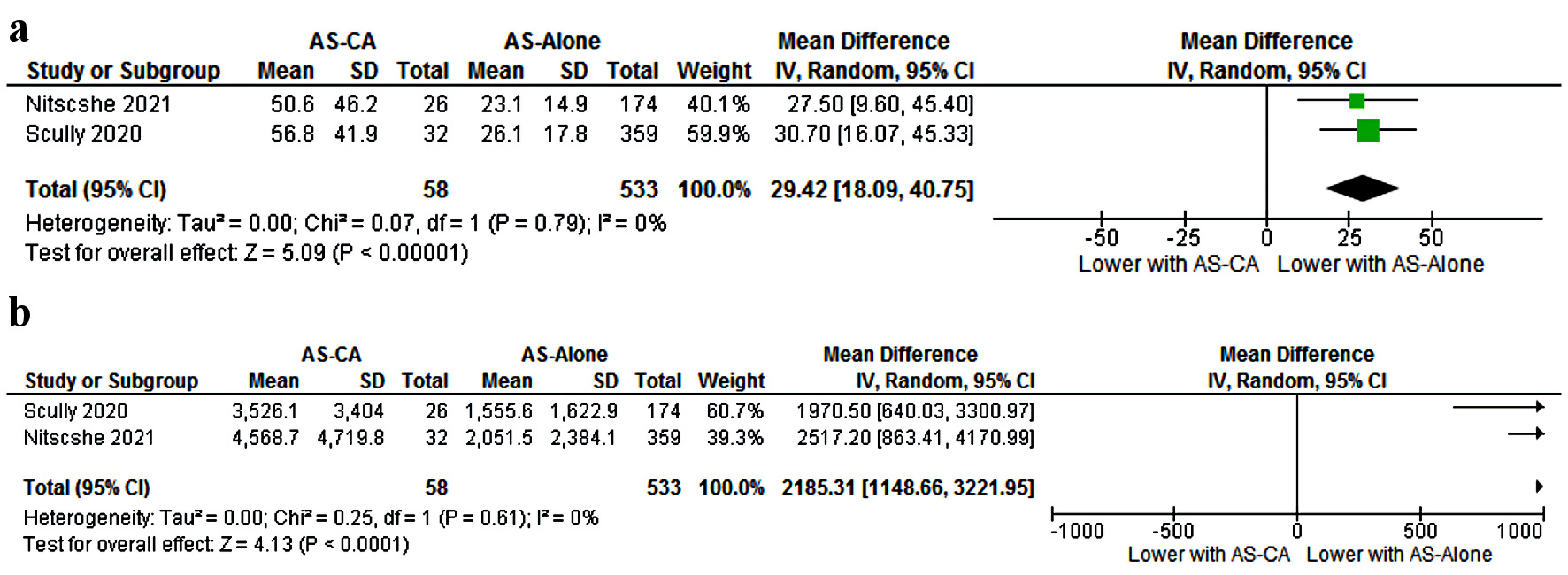 Click for large image | Figure 7. Biochemical comparison of: (a) High-sensitivity troponin; (b) NT-proBNP. NT-proBNP: N-terminal pro-brain natriuretic peptide; CI: confidence interval; AS-CA: aortic stenosis with cardiac amyloidosis; AS-alone: aortic stenosis. |
All-cause mortality
Three studies reported 1-year all-cause mortality [8, 9, 11], while three other studies noted all-cause mortality in median follow-up duration ranging from 1.6 to 2.3 years [12-14]. During the reported follow-up period for at least 1 year, patients with AS-CA had higher all-cause mortality than patients with AS alone (33% vs. 22%, P = 0.02) (Fig. 8).
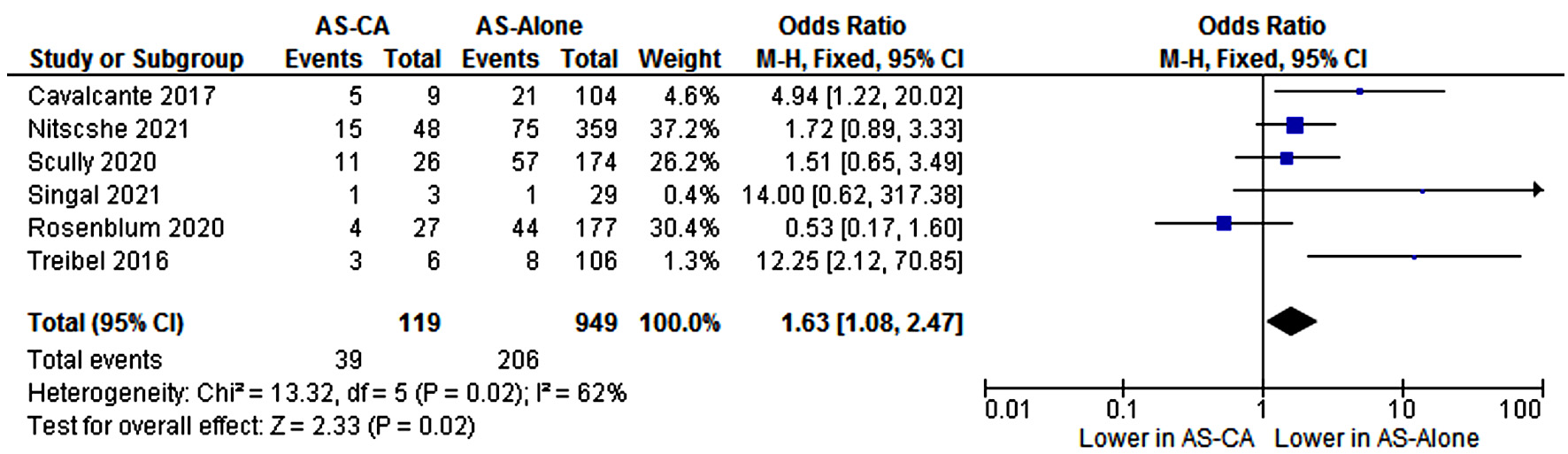 Click for large image | Figure 8. Comparison of all-cause mortality among patients with AS-CA and patients with AS-alone. CI: confidence interval; AS-CA: aortic stenosis with cardiac amyloidosis; AS-alone: aortic stenosis. |
Based on the above analysis, various diagnostic parameters were identified which increase the propensity of underlying CA among patients with AS. The parameters are summarized in Table 5.
Click to view | Table 5. Clinical and Echocardiographic Parameters Suggestive of Concomitant Cardiac Amyloidosis (Means Provided in Brackets Where Applicable) |
Meta-regression to identify associated biomarkers
In order to demonstrate the incremental utility of various diagnostic parameters highlighted in Table 5, meta-regression was performed using the identified significant variables. Entering all the baseline variables and removing the non-significant variables resulted in the following model.
Standard differences in means = 0.2236 + 6MWT (-2.2943) + E/A ratio (4.6541) + hsTNT (3.7329) + MCF (-2.5668) + mitral annular S’ (-1.0305) + NT-proBNP (3.1850) + SVI (-1.3880)
The overall model was significant (Q = 219.10, df = 7, P < 0.001). The R2 analog for this model was 0.76. Parameters that drove the highest gain in R2 included NT-proBNP (0.22), hsTNT (0.16) and E/A ratio (0.17). In addition, the analysis identified parameters most significantly associated with concomitant CA. Table 6 lists the parameters in descending order of their relative strength of estimate noted by the model. Goodness of fit - H0: Tau2 = 0.5770, Tau = 0.760, I2 = 89.13%, Q = 625.61, df = 68, P < 0.001.
Click to view | Table 6. Random-Effects Meta-Regression: Standard Mean Differences and Independent Variables |
Cost effectiveness analysis
Cost-effectiveness is usually measured in quality-adjusted life-years (QALY). It is estimated that tafamidis alone adds on an average 1.29 QALY in ATTR patients [17]. This is in addition to the effects of other FDA-approved medications and the lifestyle modifications/targeted therapies the patients may receive following the diagnosis. The average cost of a nuclear pyrophosphate (PYP) scan is between $3,000 to $7,000 in the USA (without insurance). At an estimated detection rate of one in nine post-TAVR patients, the cost of detection of one ATTR patient would be between $27,000 to $63,000. For each QALY added by tafamidis, the cost of detection with nuclear PYP scan will be between $20,930 to $48,837/QALY. This is well below the proposed incremental cost-effectiveness ratio (ICER) for USA: $50,000 to $150,000/QALY [18]. This assumption however does not take into account the downstream costs following the diagnosis, which can be multifactorial and difficult to estimate.
| Discussion | ▴Top |
In the current meta-analysis, we noted that: 1) the prevalence of concomitant ATTR-CA in patients undergoing TAVR/SAVR is 11% (a prevalence of one in nine patients); 2) patients with AS-CA have worse prognostic biomarkers at the time of TAVR/SAVR than those with AS alone; and 3) we identified associated clinical parameters which should raise the suspicion of concomitant CA among patients with severe AS.
ATTR-CA is increasingly being recognized as an important cause of heart failure. However, ATTR-CA is characterized by vague manifestations, frequently with an overlap with other forms of HFpEF. Diagnosis often requires a strong suspicion and some degree of pattern recognition by the clinicians. In a prospective study of HFpEF patients undergoing endomyocardial biopsy 14% patients had CA, of which the most common was the ATTR-wt [19]. HFpEF-CA patients in the study were older, had higher troponin I levels, higher NT-ProBNP levels and larger LVMI, which is similar to the findings in our study. Amyloidosis is also associated with poor survival in comparison to other causes of heart failure [20].
One of the common associations of ATTR is with AS. Patients with significant AS have a high prevalence of ATTR, with studies suggesting up to 16% prevalence [8, 9, 21]. Increasingly, TAVR has become the preferred management for severe AS in the USA, and more than 100,000 TAVR procedures were performed between 2012 to 2016 [22]. Not screening such patients in their perioperative period for concomitant CA represents a lost opportunity to identify a potentially fatal disease which could alter the long-term prognosis. The present meta-analysis noted a pooled prevalence of ATTR-CA at 11% among AS patients undergoing TAVR/SAVR. This equates to one in nine patients undergoing the procedure, or which translates to 11,000 patients who underwent TAVR between 2012 to 2016 had concomitant CA. Such high prevalence of ATTR in AS should prompt reconsideration of screening strategies in patients with AS in general and severe AS patients undergoing TAVR/SAVR.
99mTechnetium (Tc) labeled nuclear PYP scan offers a low-cost, widely available, and noninvasive screening of ATTR with phenomenal accuracy (> 95% sensitivity and specificity for ATTR in one study) [23]. The detection rate of ATTR-CA is rising due to the availability of such accurate noninvasive testing [21, 23, 24]. This is indicative of a previously underestimated high prevalence of ATTR in the community. However, it is not known if a nuclear PYP scan screening protocol for patients who are being evaluated for TAVR/SAVR would result in a cost-effective process to detect ATTR-CA. Screening and treatment of patients with AS-CA through an early screening strategy is yet to be made uniform. Our meta-analysis shows worse mortality among patients with AS-CA than AS-alone patients. It still remains undeciphered whether treatment of AS-CA prior to TAVR/SAVR can improve outcomes. Nitsche et al reported in their study that seven of 47 patients were treated with tafamidis after aortic valve replacement but did not result in a mortality difference [8]. All other the studies did not consistently report use of tafamidis and other FDA-approved medications in those diagnosed with AS-CA. Therefore, the downstream benefit of medical therapy for ATTR remains unknown. Our study provides additional insight into the benefits of ATTR-CA screening in patients with significant AS and to identify functional, laboratory, and echocardiographic features that would raise the clinical suspicion for concomitant CA.
Various associations to CA have been reported in the literature. CTS precedes development of CA by 5 - 9 years and is significantly higher in prevalence among ATTR-wt patients [25]. Atrial fibrillation is diagnosed in about one in every three patients with ATTR. RBBB and high-grade atrioventricular (AV) blocks are prevalent among patients with amyloidosis, owing to the infiltrative effect on the conduction pathway [26]. Our analysis suggested that patients with AS-CA are more likely to have increased interventricular septal wall thickening, increased LA diameter, lower MCF and lower SVI compared to patients with AS alone. The thicker ventricular walls are likely indicative of the infiltrative process inherent in amyloidosis which supersedes the true hypertrophy seen with AS alone. Similarly increased LA dimensions likely indicate worse restrictive diastolic dysfunction, and the low stroke volume indicates the low ventricular volume and decreased contractility in amyloid patients.
Pagourelias et al highlighted that among echocardiographic indices, E/e’ ratio, LA volume index and MCF have high specificity with MCF having highest accuracy for potential underlying amyloidosis [27]. Castano et al reported average mitral annular S’ ≤ 6 cm/s to be a strong predictor for CA on echocardiography which should prompt cardiac scintigraphy for screening [10]. With advancing amyloid deposition, the deterioration of left ventricular function correlates to an increase in wall thickness over time [28]. Thus, MCF functions as an early predictor of mortality in ATTR patients compared to ejection fraction (EF), as the EF may continue to stay in the normal range even in advanced disease because of concomitant decrease in end-diastolic volume and stroke volume [29]. Chacko et al reported SVI, right atrial area index, longitudinal strain, and E/e’ were all independently associated with mortality in a cohort of patients with ATTR-wt with presence of AS independently increasing the mortality [30]. The present study noted that patients with AS-CA had higher E/A ratio again indicative of worse diastolic dysfunction.
In our analysis, we noted that patients with AS-CA were more likely to have LFLG AS physiology than patients with AS alone. This also corresponds with the low MCF and SVI in the patients with AS-CA. Castano et al reported that stage D3 low-flow AS presents with a preserved EF phenotype initially in patients with both AS and CA and then worsens to stage D2 LFLG AS with a low LVEF as systolic dysfunction ensues [10]. Patients with LFLG with reduced EF, have poor prognosis and require a dobutamine stress echocardiography to assess flow reserve; however, in the subset of amyloid patients where dobutamine is unable to effectively increase LV outflow and results tend to be inconclusive often necessitating CT for quantification of aortic valve calcium burden [31]. These patients are likely to be missed in clinical practice as their AS remains masked behind the low-pressure gradients. The high prevalence of concomitant AS-CA in such LFLG AS patients adds further to the misdiagnosis of CA. Based on the findings of the meta-analysis, it is emphasized that LFLG AS be considered a risk factor for underlying AS-CA and be screened accordingly. Table 5 summarizes all the additional risk factors indicative of an underlying AS-CA. In addition, an incremental effect was noted when more risk factors were present in any given patient summarized in Table 6.
Moreover, the presence of ATTR in patients with severe AS was associated with worse prognostic biomarkers of myocardial injury and functional capacity in our meta-analysis. Cardiac biomarkers are often elevated among patients with CA, indicating ongoing cardiac myocyte toxicity either from the hemodynamic effects of diastolic failure or the amyloid fibril-related direct toxicity [32]. Takashio et al highlighted high serum hsTNT in the setting of cardiac hypertrophy is highly suggestive of CA [33]. Elevated hsTnT levels have been shown to be a strong predictor of all-cause mortality among patients with CA [34]. Similarly, elevated NT-proBNP elevation is strongly associated with mortality among patients with both AL- and ATTR amyloidosis [35]. This translated into worse all-cause mortality among the AS-CA patients in our study.
Various pathophysiological mechanisms have been suggested to explain the association of AS with CA. Endothelial damage from deposition of amyloid deposits in the aortic valve could lead to AS. Another possibility suggested is the co-occurrence of both processes independently but driven by the common factor of aging. AS-induced turbulence could also accelerate the process of amyloid deposition in the cardiac tissues [36]. In addition, CA is a progressively fatal disease, if left untreated. Transthyretin-stabilizing agent tafamidis was approved by FDA for treatment of ATTR, following a landmark trial (ATTR-ACT), which showed a reduction in the combination of all-cause mortality and cardiovascular-related hospitalizations [2]. The medication was also shown to slow the worsening of functional decline among ATTR patients. In addition to the above, two other agents for the hereditary ATTR polyneuropathy are inotersen and patisiran [3, 4]. Patisiran may play a role in reversing cardiomyopathy-related remodeling in hereditary ATTR patients [37]. With the advent of efficacious therapies, it is imperative to diagnose and treat ATTR to improve the long-term prognosis of the patients post TAVR/SAVR [38]. Thus, identifying patients with ATTR and intervening with treatment around the time of the valve procedure could provide an important opportunity to alter the course of the disease. Our cost-effectiveness analysis yielded a favorable picture for widespread screening of TAVR/SAVR patients with nuclear PYP scan, with additional QALY added by tafamidis treatment alone.
The findings of the present study are comparable to a prior meta-analysis by Ho et al [39] in which CA had a 14% prevalence in AS patients referred for TAVR/SAVR. However, the study included heterogenous types of studies including those not comparing AS-CA to AS-alone and those not making a distinction between AL and ATTR. Consequently, the study focused on presenting the prevalence of AS-CA without identifying risk factors for screening. The present study provides an outlook to identify CA patients amongst TAVR/SAVR referred AS patients by identifying high-risk factors and proposes a cost-effective screening for AS-CA. An earlier reported smaller systematic review by Ricci et al [40] demonstrated higher all-cause mortality in patients with AS-CA, with left ventricular wall thickness being a major prognostic marker. This study focused primarily on mortality outcomes in patients with AS-CA. Our study also found mortality among patients with AS-CA to be higher.
The studies included in the present meta-analysis did not consistently report the use of novel ATTR-specific therapy after the diagnosis of AS-CA. This was largely because the studies were started or completed before the newer targeted therapies became available. Thus, though the prevalence of AS-CA is known, the benefit accrued from starting medical therapy remains unexplored and a potential idea for future prospective studies. In addition to this, heart transplantation is also a viable option for the ATTR patients who lack significant extra-cardiac disease which requires an early diagnosis [41]. This again underlines the need for an effective screening strategy for such patients.
In summary, concomitant ATTR-CA is frequently associated in patients with significant AS. Screening them for ATTR can result in an early diagnosis and treatment of this otherwise rapidly fatal disease. Various risk factors for concomitant AS-CA were identified, and a cost-effective analysis was discussed in detail. Given the noted prevalence of one CA in nine AS patients, the use of nuclear PYP scan would result in a cost-effective screening strategy to identify concomitant CA in patients undergoing TAVR/SAVR.
Limitations
Significant heterogeneity existed among the studies due to the nature of the studies (observational or retrospective). The number of patients with AS-CA in each study was small. Selection bias, though unavoidable, was reduced after review of the studies by two authors. Due to the lack of randomized control trials, we had to use prospective and retrospective cohort studies for this meta-analysis. There was variability in the definition of CA and in screening tools used. The studies were performed in various countries where the diagnostic algorithms and the ATTR-specific imaging techniques used for screening were variable (Table 2) [8-12]. The overall efficacy and sensitivity of all the various screening techniques were assumed to be comparable for the purpose of the meta-analysis. There was no consistent description of the type of ATTR in the patients (genetic vs. wild-type). The meta-analysis excluded studies reporting AL amyloidosis patients, as this would introduce heterogeneity related to the variable incidence of AL amyloidosis in AS patients and the difference in screening tools [39].
Within the regression model, some of the well-known parameters reported in the literature including global longitudinal strain difference [42] were not found to be significant in the analysis as the difference in reported means was not significant in the pooled analysis. This may be indicative of the heterogeneity inherent in the studies and the relatively small sample size in the individual studies. The analyses are provided here (Fig. 6).
Conclusions
CA has a high prevalence in patients with AS and is associated with worse prognostic biomarkers than AS alone. An effective screening strategy for AS-CA can increase awareness, institute early treatment and allow planning for long-term care.
Acknowledgments
None to declare.
Financial Disclosure
No funding was received by authors for this manuscript.
Conflict of Interest
None of the authors have any conflict of interest to declare.
Informed Consent
No consent was required for this study as it was a meta-analysis of already published data.
Author Contributions
GV conceptualized the study idea. SA and NM extracted and analyzed the data. The initial manuscript was drafted by SA and GV. All authors contributed to the critical review and improvement of the manuscript and have reviewed the final version of the manuscript prior to submission.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
TAVR: transcatheter aortic valve replacement; SAVR: surgical aortic valve replacement; AS: aortic stenosis; CA: cardiac amyloidosis; 6MWT: 6-min walk test; MCF: myocardial contraction fraction; SVI: stroke volume index; LVMI: left ventricular mass index; LFLG: low-flow low-gradient; hsTNT: high-sensitivity cardiac troponin
| References | ▴Top |
- Wang L, Swerdel JN, Weaver J, Weiss B, Pan G, Yuan Z, DiBattiste PM. Incidence rate of hospitalization and mortality in the first year following initial diagnosis of cardiac amyloidosis in the US claims databases. Curr Med Res Opin. 2021;37(8):1275-1281.
doi pubmed - Maurer MS, Schwartz JH, Gundapaneni B, Elliott PM, Merlini G, Waddington-Cruz M, Kristen AV, et al. Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N Engl J Med. 2018;379(11):1007-1016.
doi pubmed - Brannagan TH, Wang AK, Coelho T, Waddington Cruz M, Polydefkis MJ, Dyck PJ, Plante-Bordeneuve V, et al. Early data on long-term efficacy and safety of inotersen in patients with hereditary transthyretin amyloidosis: a 2-year update from the open-label extension of the NEURO-TTR trial. Eur J Neurol. 2020;27(8):1374-1381.
doi pubmed - Adams D, Gonzalez-Duarte A, O'Riordan WD, Yang CC, Ueda M, Kristen AV, Tournev I, et al. Patisiran, an RNAi therapeutic, for hereditary transthyretin amyloidosis. N Engl J Med. 2018;379(1):11-21.
doi pubmed - Wells G, Shea B, O'Connell J, Robertson J, Peterson V, Welch V, Losos M, et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analysis. Available at: https://www.ohri.ca//programs/clinical_epidemiology/oxford.asp. Accessed May 30, 2022.
- McGuinness LA, Higgins JPT. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods. 2021;12(1):55-61.
doi pubmed - Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785-1805.
doi pubmed - Nitsche C, Scully PR, Patel KP, Kammerlander AA, Koschutnik M, Dona C, Wollenweber T, et al. Prevalence and Outcomes of Concomitant Aortic Stenosis and Cardiac Amyloidosis. J Am Coll Cardiol. 2021;77(2):128-139.
doi pubmed - Scully PR, Patel KP, Treibel TA, Thornton GD, Hughes RK, Chadalavada S, Katsoulis M, et al. Prevalence and outcome of dual aortic stenosis and cardiac amyloid pathology in patients referred for transcatheter aortic valve implantation. Eur Heart J. 2020;41(29):2759-2767.
doi pubmed - Castano A, Narotsky DL, Hamid N, Khalique OK, Morgenstern R, DeLuca A, Rubin J, et al. Unveiling transthyretin cardiac amyloidosis and its predictors among elderly patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur Heart J. 2017;38(38):2879-2887.
doi pubmed - Singal AK, Bansal R, Singh A, Dorbala S, Sharma G, Gupta K, Saxena A, et al. Concomitant Transthyretin Amyloidosis and Severe Aortic Stenosis in Elderly Indian Population: A Pilot Study. JACC CardioOncol. 2021;3(4):565-576.
doi pubmed - Cavalcante JL, Rijal S, Abdelkarim I, Althouse AD, Sharbaugh MS, Fridman Y, Soman P, et al. Cardiac amyloidosis is prevalent in older patients with aortic stenosis and carries worse prognosis. J Cardiovasc Magn Reson. 2017;19(1):98.
doi pubmed - Rosenblum H, Masri A, Narotsky DL, Goldsmith J, Hamid N, Hahn RT, Kodali S, et al. Unveiling outcomes in coexisting severe aortic stenosis and transthyretin cardiac amyloidosis. Eur J Heart Fail. 2021;23(2):250-258.
doi pubmed - Treibel TA, Fontana M, Gilbertson JA, Castelletti S, White SK, Scully PR, Roberts N, et al. Occult transthyretin cardiac amyloid in severe calcific aortic stenosis: prevalence and prognosis in patients undergoing surgical aortic valve replacement. Circ Cardiovasc Imaging. 2016;9(8):e005066.
doi pubmed - Oda S, Kidoh M, Takashio S, Inoue T, Nagayama Y, Nakaura T, Shiraishi S, et al. Quantification of myocardial extracellular volume with planning computed tomography for transcatheter aortic valve replacement to identify occult cardiac amyloidosis in patients with severe aortic stenosis. Circ Cardiovasc Imaging. 2020;13(5):e010358.
doi pubmed - Longhi S, Lorenzini M, Gagliardi C, Milandri A, Marzocchi A, Marrozzini C, Saia F, et al. Coexistence of degenerative aortic stenosis and wild-type transthyretin-related cardiac amyloidosis. JACC Cardiovasc Imaging. 2016;9(3):325-327.
doi pubmed - Kazi DS, Bellows BK, Baron SJ, Shen C, Cohen DJ, Spertus JA, Yeh RW, et al. Cost-effectiveness of tafamidis therapy for transthyretin amyloid cardiomyopathy. Circulation. 2020;141(15):1214-1224.
doi pubmed - Sacristan JA. How to assess the value of low-value care. BMC Health Serv Res. 2020;20(1):1000.
doi pubmed - Hahn VS, Yanek LR, Vaishnav J, Ying W, Vaidya D, Lee YZJ, Riley SJ, et al. Endomyocardial biopsy characterization of heart failure with preserved ejection fraction and prevalence of cardiac amyloidosis. JACC Heart Fail. 2020;8(9):712-724.
doi pubmed - Kocher F, Kaser A, Escher F, Doerler J, Zaruba MM, Messner M, Mussner-Seeber C, et al. Heart failure from ATTRwt amyloid cardiomyopathy is associated with poor prognosis. ESC Heart Fail. 2020;7(6):3919-3928.
doi pubmed - Cappelli F, Perfetto F, Martone R, Di Mario C. Cardiac amyloidosis in patients undergoing TAVR: why we need to think about it. Cardiovasc Revasc Med. 2021;22:109-114.
doi pubmed - Abugroun A, Daoud H, Abdel-Rahman ME, Hallak O, Igbinomwanhia E, Sanchez A, Shroff A, et al. National trends of outcomes in transcatheter aortic valve replacement (TAVR) through transapical versus endovascular approach: from the National Inpatient Sample (NIS). Cardiovasc Revasc Med. 2020;21(8):964-970.
doi pubmed - Bokhari S, Castano A, Pozniakoff T, Deslisle S, Latif F, Maurer MS. (99m)Tc-pyrophosphate scintigraphy for differentiating light-chain cardiac amyloidosis from the transthyretin-related familial and senile cardiac amyloidoses. Circ Cardiovasc Imaging. 2013;6(2):195-201.
doi pubmed - Gillmore JD, Maurer MS, Falk RH, Merlini G, Damy T, Dispenzieri A, Wechalekar AD, et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation. 2016;133(24):2404-2412.
doi pubmed - Milandri A, Farioli A, Gagliardi C, Longhi S, Salvi F, Curti S, Foffi S, et al. Carpal tunnel syndrome in cardiac amyloidosis: implications for early diagnosis and prognostic role across the spectrum of aetiologies. Eur J Heart Fail. 2020;22(3):507-515.
doi pubmed - Cappelli F, Vignini E, Martone R, Perlini S, Mussinelli R, Sabena A, Morini S, et al. Baseline ECG features and arrhythmic profile in transthyretin versus light chain cardiac amyloidosis. Circ Heart Fail. 2020;13(3):e006619.
doi pubmed - Pagourelias ED, Mirea O, Duchenne J, Van Cleemput J, Delforge M, Bogaert J, Kuznetsova T, et al. Echo parameters for differential diagnosis in cardiac amyloidosis: a head-to-head comparison of deformation and nondeformation parameters. Circ Cardiovasc Imaging. 2017;10(3):e005588.
doi pubmed - Quarta CC, Solomon SD, Uraizee I, Kruger J, Longhi S, Ferlito M, Gagliardi C, et al. Left ventricular structure and function in transthyretin-related versus light-chain cardiac amyloidosis. Circulation. 2014;129(18):1840-1849.
doi pubmed - Rubin J, Steidley DE, Carlsson M, Ong ML, Maurer MS. Myocardial Contraction Fraction by M-Mode Echocardiography Is Superior to Ejection Fraction in Predicting Mortality in Transthyretin Amyloidosis. J Card Fail. 2018;24(8):504-511.
doi pubmed - Chacko L, Martone R, Bandera F, Lane T, Martinez-Naharro A, Boldrini M, Rezk T, et al. Echocardiographic phenotype and prognosis in transthyretin cardiac amyloidosis. Eur Heart J. 2020;41(14):1439-1447.
doi pubmed - Ternacle J, Krapf L, Mohty D, Magne J, Nguyen A, Galat A, Gallet R, et al. Aortic stenosis and cardiac amyloidosis: JACC review topic of the week. J Am Coll Cardiol. 2019;74(21):2638-2651.
doi pubmed - Ton VK, Mukherjee M, Judge DP. Transthyretin cardiac amyloidosis: pathogenesis, treatments, and emerging role in heart failure with preserved ejection fraction. Clin Med Insights Cardiol. 2014;8(Suppl 1):39-44.
doi pubmed - Takashio S, Yamamuro M, Izumiya Y, Hirakawa K, Marume K, Yamamoto M, Ueda M, et al. Diagnostic utility of cardiac troponin T level in patients with cardiac amyloidosis. ESC Heart Fail. 2018;5(1):27-35.
doi pubmed - Qian G, Wu C, Zhang Y, Chen YD, Dong W, Ren YH. Prognostic value of high-sensitivity cardiac troponin T in patients with endomyocardial-biopsy proven cardiac amyloidosis. J Geriatr Cardiol. 2014;11(2):136-140.
- Damy T, Jaccard A, Guellich A, Lavergne D, Galat A, Deux JF, Hittinger L, et al. Identification of prognostic markers in transthyretin and AL cardiac amyloidosis. Amyloid. 2016;23(3):194-202.
doi pubmed - Fabbri G, Serenelli M, Cantone A, Sanguettoli F, Rapezzi C. Transthyretin amyloidosis in aortic stenosis: clinical and therapeutic implications. Eur Heart J Suppl. 2021;23(Suppl E):E128-E132.
doi pubmed - Solomon SD, Adams D, Kristen A, Grogan M, Gonzalez-Duarte A, Maurer MS, Merlini G, et al. Effects of Patisiran, an RNA interference therapeutic, on cardiac parameters in patients with hereditary transthyretin-mediated amyloidosis. Circulation. 2019;139(4):431-443.
doi pubmed - Sperry BW, Jones BM, Vranian MN, Hanna M, Jaber WA. Recognizing transthyretin cardiac amyloidosis in patients with aortic stenosis: impact on prognosis. JACC Cardiovasc Imaging. 2016;9(7):904-906.
doi pubmed - Ho JS, Kor Q, Kong WK, Lim YC, Chan MY, Syn NL, Ngiam JN, et al. Prevalence and outcomes of concomitant cardiac amyloidosis and aortic stenosis: A systematic review and meta-analysis. Hellenic J Cardiol. 2022;64:67-76.
doi pubmed - Ricci F, Ceriello L, Khanji MY, Dangas G, Bucciarelli-Ducci C, Di Mauro M, Fedorowski A, et al. Prognostic significance of cardiac amyloidosis in patients with aortic stenosis: a systematic review and meta-analysis. JACC Cardiovasc Imaging. 2021;14(1):293-295.
doi pubmed - Vaidya GN, Patel JK, Kittleson M, Chang DH, Kransdorf E, Geft D, Czer L, et al. Intermediate-term outcomes of heart transplantation for cardiac amyloidosis in the current era. Clin Transplant. 2021;35(6):e14308.
doi pubmed - Agha AM, Parwani P, Guha A, Durand JB, Iliescu CA, Hassan S, Palaskas NL, et al. Role of cardiovascular imaging for the diagnosis and prognosis of cardiac amyloidosis. Open Heart. 2018;5(2):e000881.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.