

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 13, Number 6, December 2022, pages 393-397

Rare Occurrence of Apical Hypertrophic Cardiomyopathy Among Hispanics
Mohammed S. Abdallaa, b, Prasun Pudasaineea, Akshaya Ramachandrana, Muhammad S. Akbara
aDepartment of Internal Medicine, Ascension Saint Francis Hospital, Evanston, IL, USA
bCorresponding Author: Mohammed S. Abdalla, Department of Internal Medicine, Ascension Saint Francis Hospital, Evanston, IL 60202, USA
Manuscript submitted October 6, 2022, accepted October 27, 2022, published online December 1, 2022
Short title: Rare Case of ApHCM Among Hispanics
doi: https://doi.org/10.14740/cr1437
| Abstract | ▴Top |
Apical hypertrophic cardiomyopathy (ApHCM), also known as Yamaguchi syndrome represents an uncommon morphologic variant of hypertrophic cardiomyopathy (HCM) in which the myocardial hypertrophy predominantly involves the apex of the left ventricle (LV). It is exemplified by “giant” negative precordial T-waves on electrocardiography and a peculiar “spade-like” configuration of LV cavity on ventriculography historically, and more recently, on echocardiography with use of image enhancing agents. The disease entity was first described in 1976. Available literature reveals that it is prevalent largely among the East-Asian population but is rare among non-Asians. Here, we report a case of a 66-year-old Hispanic male with multiple cardiac histories including persistent atrial fibrillation, non-ST-elevation myocardial infarction (NSTEMI), and ventricular fibrillation cardiac arrest with multiple inconclusive evaluations, who later in life was found to have ApHCM. This case highlights the rare incidence of the disease among the Hispanic population and underlines the challenging diagnosis that requires a high index of suspicion in patients with cardiac symptoms, as ApHCM can masquerade as ischemic coronary heart disease. Our case also describes an unusual clinical course for ApHCM presenting with extreme clinical features, including ventricular arrhythmias and cardiac arrest, unlike the usual benign natural history of this disease.
Keywords: Apical hypertrophic cardiomyopathy; Yamaguchi syndrome; Hispanic; Echocardiogram; Ventricular fibrillation; Cardiac arrest
| Introduction | ▴Top |
Apical hypertrophic cardiomyopathy (ApHCM) is an uncommon variant of hypertrophic cardiomyopathy (HCM), most prevalent in East Asia and was first described in Japan in 1976. The disease is characterized by left ventricular (LV) hypertrophy involving the apex, giving the LV cavity a spade-like configuration on ventriculography and echocardiography with contrast. In electrocardiogram (ECG), ApHCM is characterized by marked T- wave inversions in the precordial leads (known as giant T-waves), which are often the only clue towards the diagnosis. Although significantly more common in Japanese and East Asians, the disease is increasingly being described in other populations worldwide. Here, we report a rare occurrence of ApHCM in a Hispanic male who had extensive cardiac history with inconclusive evaluations for several years and was ultimately diagnosed with the disease.
| Case Report | ▴Top |
A 66-year-old Hispanic male presented to the hospital with frequent episodes of dizziness for several days. He described the episodes as brief periods of lightheadedness unrelated to physical exertion and associated with palpitations and general weakness. During one of these episodes, he experienced shock from his automated internal cardiac defibrillator (AICD) which prompted him to seek medical care. He denied any history of nausea, vomiting, diaphoresis, abdominal pain, syncopal episode, dyspnea at rest or exertion, orthopnea, paroxysmal nocturnal dyspnea, or leg swelling.
The patient has a past medical history of hypertension, diabetes mellitus and history of cardiac arrest due to ventricular fibrillation about 2 years prior to his current presentation. At that time, he was diagnosed with non-ST-elevation myocardial infarction (NSTEMI), and coronary angiography at that time showed insignificant coronary artery disease, and single chamber AICD was placed for secondary prevention. He was also diagnosed with persistent atrial fibrillation within the last 1 year.
His medications included metoprolol, clopidogrel, rivaroxaban atorvastatin and metformin. He has not been compliant with his medical treatment and has not seen his cardiologist in over a year.
The patient works as a dishwasher in a restaurant but has not been able to go to work lately because of the increasing episodes of dizziness. He denies tobacco use, alcohol, or illicit drug use. He denies a family history of sudden cardiac death or any known cardiac disease.
On physical examination, his vital signs were as follows: blood pressure of 107/70 mm Hg, heart rate of 66/min, respiratory rate of 18, temperature of 37.0 °C and oxygen saturation (SpO2) of 98% when breathing ambient air. His peripheral pulses are symmetrical and of good volume. He has no jugular venous distention (JVD) or dependent edema. He has an implantable cardiac defibrillator (ICD) device in the left upper chest with intact overlying skin with no signs of infection or dehiscence. His first and second heart sounds are normal, no cardiac murmurs, rubs, or gallops are appreciated upon auscultation. The remainder of the physical examination was unremarkable. His ECG revealed atrial fibrillation with normal ventricular rate, marked T-wave inversions in the precordial leads V3 to V6 (Fig. 1), unchanged from prior ECG obtained during the preceding year (Fig. 2). Relevant labs include a high-sensitivity troponin of 56 (0 - 20 pg/mL) which has remained stable with chronic elevation based on comparison with old labs and had normal thyroid stimulating hormone.
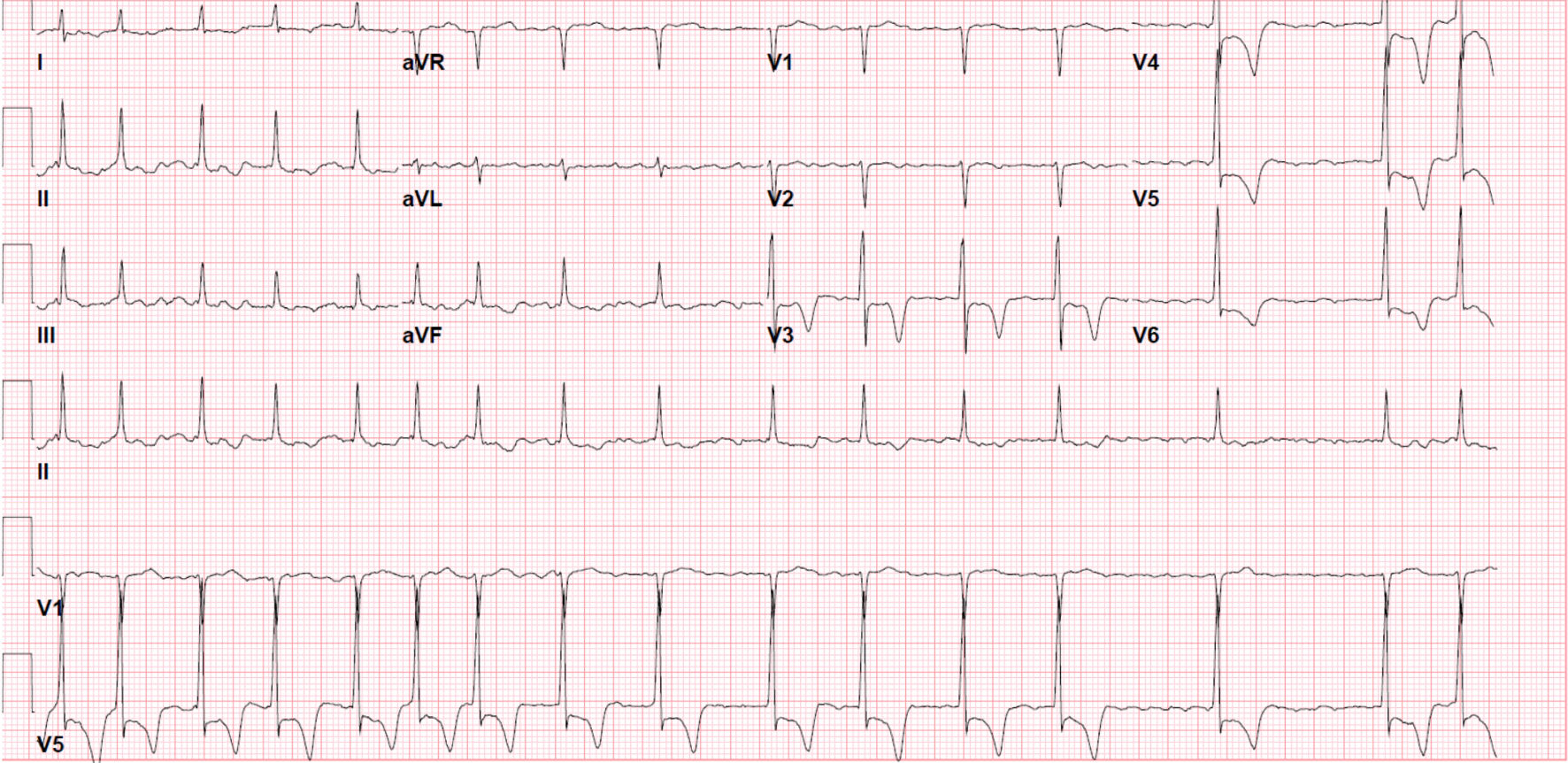 Click for large image | Figure 1. ECG on presentation shows atrial fibrillation and prominent T-waves inversion in leads V3 through V6. ECG: electrocardiogram. |
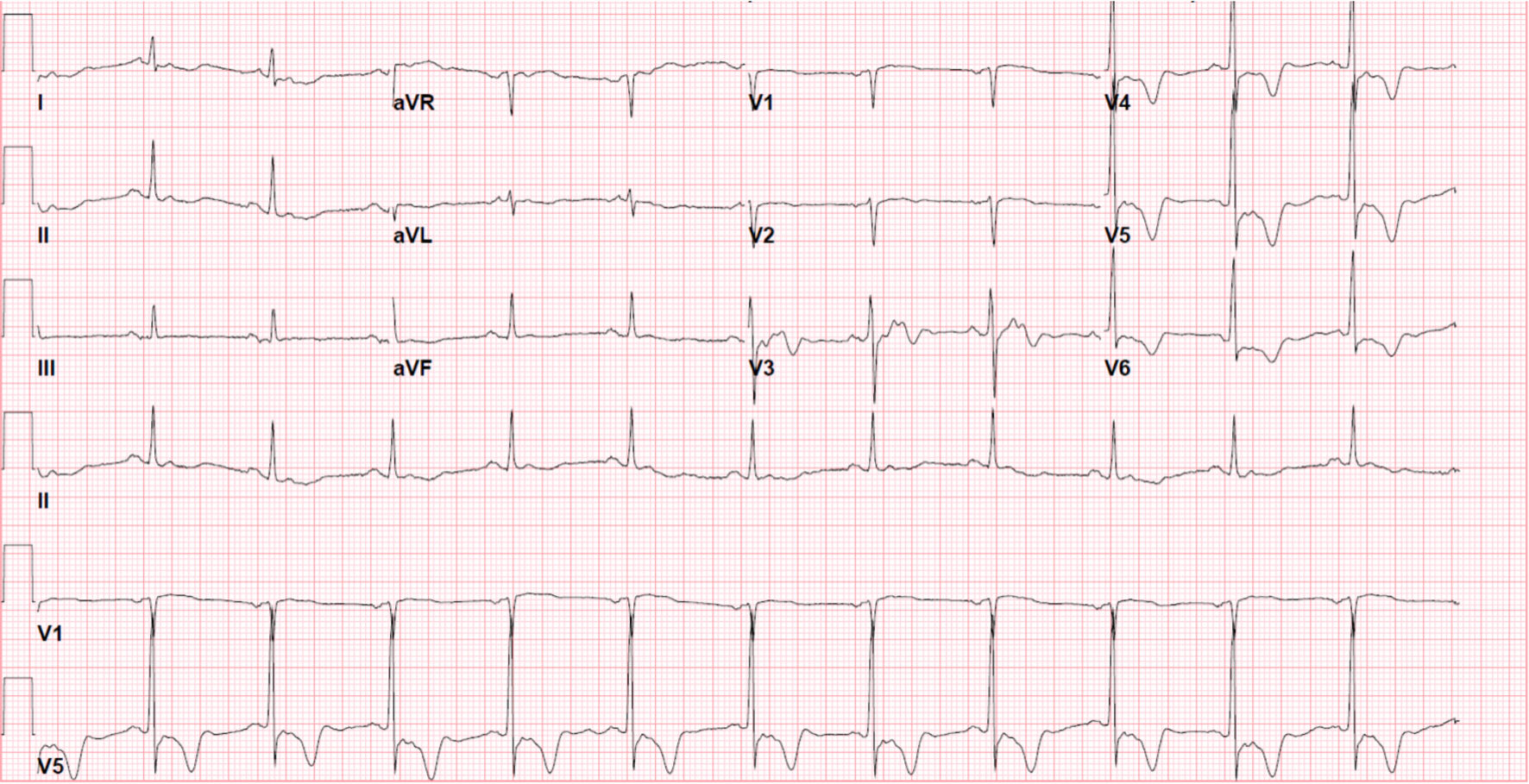 Click for large image | Figure 2. ECG about 1 year prior to presentation shows normal sinus rhythm and prominent T-waves inversion in leads V3 through V6. ECG: electrocardiogram. |
AICD interrogation showed inappropriate ICD shock for rapid atrial fibrillation. His chest X-ray was unremarkable. Echocardiography showed hypertrophy of the left ventricular apex which was more prominent upon use of contrast-enhanced study (Fig. 3a-d). His echocardiogram otherwise showed normal global left ventricular systolic function with a visually estimated ejection fraction of 60-65%. Left ventricle relaxation by Doppler could not be assessed due to underlying cardiac arrhythmia. E/e’ ratio is < 8, suggestive of normal LV filling pressures. A diagnosis of ApHCM was made and the patient was started on amiodarone to reduce the burden of his arrhythmias, he was discharged home in a good condition and scheduled for outpatient follow-up with a cardiac electrophysiologist.
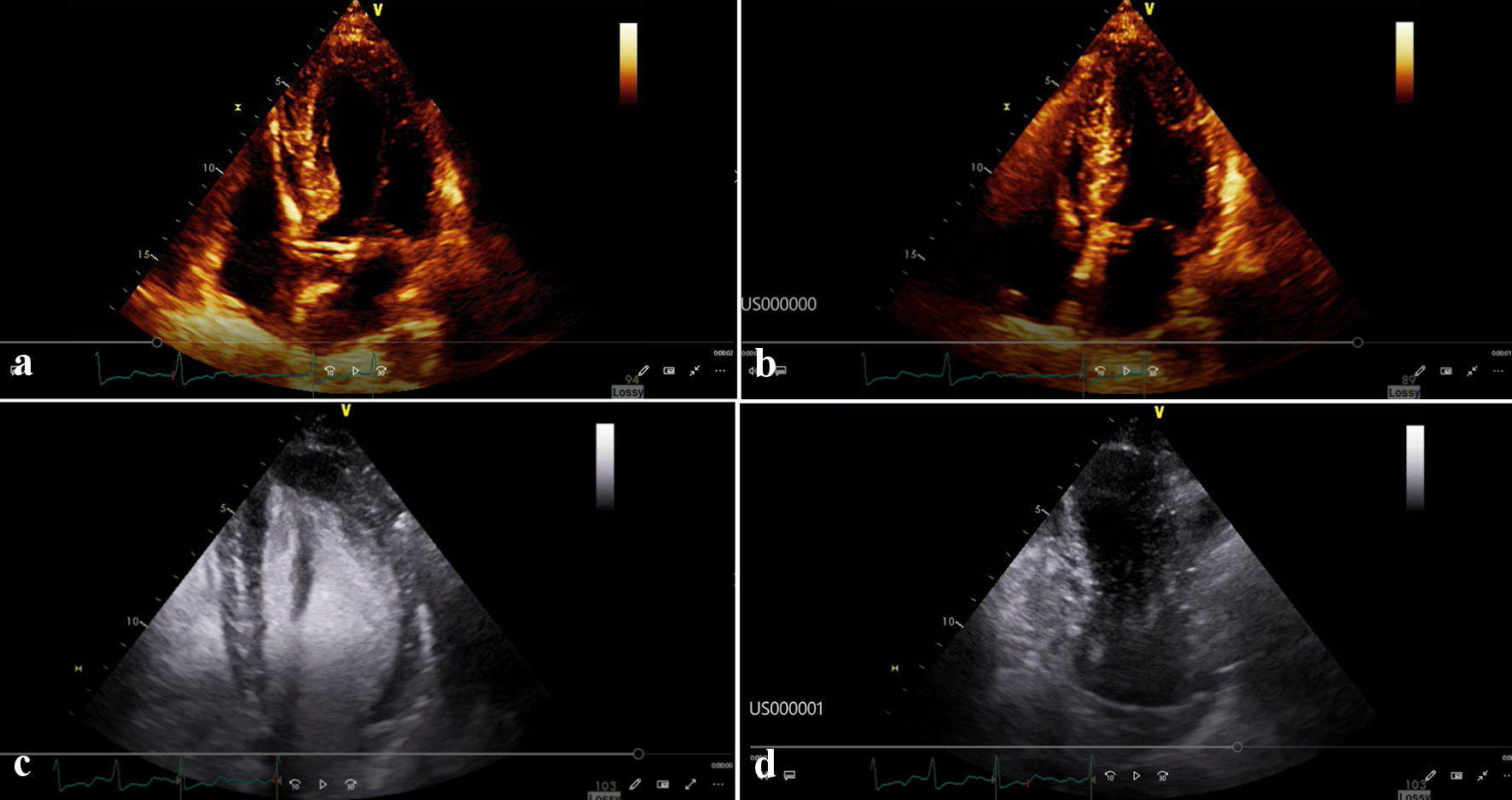 Click for large image | Figure 3. (a) Echocardiogram without contrast during diastole. (b) Echocardiogram without contrast during systole. (c) Echocardiogram with contrast during diastole showing the spade like ventricular cavity. (d) Echocardiogram with contrast during systole. |
| Discussion | ▴Top |
We report a case of a 66-year-old Hispanic male with ApHCM. ApHCM is a subtype of HCM that typically involves the left ventricular apex leading to a spade-like left ventricular cavity. The disease is common in East Asian and was first reported in Japan in 1976 [1]. Although ApHCM has been well documented among other populations worldwide [2-6], to our knowledge, only one case has been reported among Hispanics [7].
ApHCM has familial inheritance, mostly in an autosomal dominant pattern, although fewer ApHCM patients report a positive family history compared with classic HCM [8]. The majority of mutations are sarcomeric with significant influence from demographic and environmental factors [8]. Sporadic forms of the disease caused by acquired sarcomeric genetic mutations also exist [8]. Histopathological findings are not distinguishable from other forms of HCM. These can be of different extent, and consist mainly of edema, interstitial fibrosis, disorganization of myocardial fibers, and bizarre nuclei in the myocardium [9].
The variability of its clinical presentation and the clinical course makes ApHCM a challenging diagnosis. The diagnosis is commonly missed or delayed [10], as in our patient’s case.
Symptoms of ApHCM are indistinguishable from those of coronary heart disease (CHD) or those of other forms of cardiomyopathy and include chest pain, palpitations, dyspnea, lightheadedness, and syncope [10]. In extreme cases, cardiac arrest can occur due to ventricular arrhythmias as occurred with our patient. Diastolic heart failure can develop because of impaired left ventricular filling secondary to left ventricular wall stiffness and decreased compliance. This in turn can lead to increased atrial pressures and dilatation which predisposes to atrial fibrillation as seen in our patient’s case.
Patients with ApHCM can also develop small-vessel coronary artery disease and microvascular obstruction. This is thought to be related to left ventricular cavity obliteration and the persistence of apical contraction into diastole, resulting in regional apical myocardial perfusion defects. [11].
The diagnosis of ApHCM used to rely on the demonstration of the characteristic spade-like configuration of the left ventricular cavity and marked apical obliteration on left ventriculography along with the characteristic “giant” negative T-waves and high QRS voltage on surface ECG [12]. However, these giant negative T-waves (negative T-wave voltage of ≥ 1 mV [13], although characteristic, are no longer required for diagnosis because of lack of specificity. Many other cardiac conditions including coronary artery disease and other forms of HCM are often associated with similar T-wave changes.
Diagnosis of ApHCM currently relies on identifying the characteristic apical left ventricular hypertrophy (LVH) through echocardiography or cardiac magnetic resonance imaging (CMR). Diagnostic criteria include apical wall thickness ≥ 15 mm and a ratio of maximal apical to posterior wall thickness ≥ 1.5 [13]. Contrast-enhanced echocardiography provides a better view of the left ventricular configuration in patients with ApHCM, hence improving diagnostic yield and two-dimensional speckle tracking echocardiography, thereby allowing the assessment of LV apical deformation [14]. In the case of our patient, ApHCM was initially missed when conventional echocardiography was used during initial presentation but was eventually diagnosed using contrast-enhanced echocardiography.
ApHCM has been classically thought of as a benign condition with a favorable clinical course; however, many studies suggest that the risk of significant cardiac events including cardiac arrest, myocardial ischemia, advanced heart failure, atrial and ventricular arrhythmias is comparable to other forms of HCM [10]. Three features have been identified as predictors of cardiovascular morbidity in some studies, these include age less than 41 at presentation, left atrial enlargement, and New York Heart Association functional class II or more at baseline [13]. The annual cardiovascular mortality in these patients was estimated to be about 0.1% [13]. In our patient’s case, his first clinical presentation was cardiac arrest.
Treatment goals for ApHCM include decreasing heart rate and reducing ventricular arrhythmia burden using beta-blockers and calcium-channel blockers, and the use of angiotensin-converting enzyme inhibitors for afterload reduction [15]. Ablation has been employed to treat sustained monomorphic ventricular tachycardia (VT) that results from apical scarring [16]. The need for an ICD is based on the same European Society of Cardiology (ESC) 5-year HCM sudden cardiac death (SCD) risk scoring system used for other forms of cardiomyopathy [8, 17], although this tends to underestimate the need for ICD in patients with ApHCM, as these patients typically report less family history of sudden cardiac death compared to other forms of HCM. Apical myomectomy has been utilized for the treatment of symptomatic midventricular obstruction with cavity obliteration (MVOCO) as a means of reducing gradients to help improve symptoms of heart failure [18].
Conclusions
ApHCM has been historically thought of as a disease of the Far East, however, an increasing number of cases has been reported in other populations. The prevalence of disease in Hispanic populations is not known but our case report of a Hispanic patient with ApHCM raises the importance of keeping a high index of suspicion when considering differential diagnosis in patients with cardiac symptoms regardless of their racial origin. Although ApHCM can present a diagnostic challenge given its nonspecific symptoms and signs, the presence of the characteristic giant T-waves in the precordial leads, although nonspecific, can serve as a very important clue towards diagnosis. Our case also highlights the possibility of extreme manifestation of ApHMC as cardiac arrest although many previous studies reported a more benign course compared to other forms of HCM.
Acknowledgments
None to declare.
Financial Disclosure
No funding was received for this case report.
Conflict of Interest
There is no conflict of interest in this case report from all authors.
Informed Consent
The patient has provided informed consent for publication.
Author Contributions
Mohammed Abdalla, MD, reviewed literature about the topic, prepared the discussion part of the submission with focus of elements relevant to our case and provided relevant referencing. Prasun Pudasainee, MD, prepared the case presentation including the patient’s history, physical examination, relevant investigations, treatment, and outcome and obtained the supporting imaging and ECG with the help of the supervising cardiologist. Akshaya Ramachandran, MD, did the proof reading of the whole manuscript and helped with the organization of the case presentation. Muhammad S. Akbar, MD, is the supervising cardiologist who diagnosed the case, helped with identifying the relevant clinical data, provided us with the echocardiogram pictures and ECG and made the revision of the overall case report.
Data Availability
Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
| References | ▴Top |
- Sakamoto T, Tei C, Murayama M, Ichiyasu H, Hada Y. Giant T wave inversion as a manifestation of asymmetrical apical hypertrophy (AAH) of the left ventricle. Echocardiographic and ultrasono-cardiotomographic study. Jpn Heart J. 1976;17(5):611-629.
doi pubmed - Rovelli EG, Parenti F, Devizzi S. Apical hypertrophic cardiomyopathy of "Japanese type" in a Western European person. Am J Cardiol. 1986;57(4):358-359.
doi - Kureshi SA, Malik SM, Hyder W. Apical hypertrophic cardiomyopathy in Pakistan: electrocardiographic, echocardiographic and myocardial scintigraphic features. J Pak Med Assoc. 1995;45(5):117-120.
- Kranidis A, Filippatos G, Mavrogeni S, Kostopoulos K, Kappos K, Kardaras F, Fehske W, et al. Apical hypertrophic cardiomyopathy with unusual features in a Greek woman. Jpn Heart J. 1994;35(3):395-402.
doi pubmed - Albanesi Filho FM, Castier MB, Lopes AS, Ginefra P. [Is the apical hypertrophic cardiomyopathy seen in one population in Rio de Janeiro city similar to that found in the East?]. Arq Bras Cardiol. 1997;69(2):117-123.
doi - Kitaoka H, Doi Y, Casey SA, Hitomi N, Furuno T, Maron BJ. Comparison of prevalence of apical hypertrophic cardiomyopathy in Japan and the United States. Am J Cardiol. 2003;92(10):1183-1186.
doi pubmed - Shah FA, Fujikawa P, Miller JB, Singh H. A novel case of yamaguchi syndrome in a hispanic male. Cureus. 2021;13(9):e17651.
doi - Arad M, Penas-Lado M, Monserrat L, Maron BJ, Sherrid M, Ho CY, Barr S, et al. Gene mutations in apical hypertrophic cardiomyopathy. Circulation. 2005;112(18):2805-2811.
doi pubmed - Nakanishi S, Nishiyama S, Nishimura S, Yamaguchi H, Matsuya S. [Histological features of apical hypertrophic cardiomyopathy]. J Cardiogr Suppl. 1985;6:3-11.
- Jan MF, Todaro MC, Oreto L, Tajik AJ. Apical hypertrophic cardiomyopathy: Present status. Int J Cardiol. 2016;222:745-759.
doi pubmed - Stephenson E, Monney P, Pugliese F, Malcolmson J, Petersen SE, Knight C, Mills P, et al. Ineffective and prolonged apical contraction is associated with chest pain and ischaemia in apical hypertrophic cardiomyopathy. Int J Cardiol. 2018;251:65-70.
doi pubmed - Yamaguchi H, Ishimura T, Nishiyama S, Nagasaki F, Nakanishi S, Takatsu F, Nishijo T, et al. Hypertrophic nonobstructive cardiomyopathy with giant negative T waves (apical hypertrophy): ventriculographic and echocardiographic features in 30 patients. Am J Cardiol. 1979;44(3):401-412.
doi - Eriksson MJ, Sonnenberg B, Woo A, Rakowski P, Parker TG, Wigle ED, Rakowski H. Long-term outcome in patients with apical hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002;39(4):638-645.
doi - Kao YC, Lee MF, Mao CT, Chen WS, Yang NI, Cherng WJ, Hung MJ. Differences of left ventricular systolic deformation in hypertensive patients with and without apical hypertrophic cardiomyopathy. Cardiovasc Ultrasound. 2013;11:40.
doi pubmed - Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124(24):e783-831.
doi - Inada K, Seiler J, Roberts-Thomson KC, Steven D, Rosman J, John RM, Sobieszczyk P, et al. Substrate characterization and catheter ablation for monomorphic ventricular tachycardia in patients with apical hypertrophic cardiomyopathy. J Cardiovasc Electrophysiol. 2011;22(1):41-48.
doi pubmed - O'Mahony C, Jichi F, Ommen SR, Christiaans I, Arbustini E, Garcia-Pavia P, Cecchi F, et al. International External Validation Study of the 2014 European Society of Cardiology Guidelines on sudden cardiac death prevention in hypertrophic cardiomyopathy (EVIDENCE-HCM). Circulation. 2018;137(10):1015-1023.
doi pubmed - Schaff HV, Brown ML, Dearani JA, Abel MD, Ommen SR, Sorajja P, Tajik AJ, et al. Apical myectomy: a new surgical technique for management of severely symptomatic patients with apical hypertrophic cardiomyopathy. J Thorac Cardiovasc Surg. 2010;139(3):634-640.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.