

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Short Communication
Volume 14, Number 2, April 2023, pages 149-152

Sodium Chloride Physiological Saline Solution Versus Water Preparations Injectable in the Use of Shockwave Intravascular Lithotripsy: A Single-Center Experience
Quentin Landolffa, f ![]() , Matthieu Godina, Alexandre Canvillea, Benjamin Hontonb, Jacques Monseguc, Marine Quillotd, Jacques Berlanda, Rene Koninga, Nicolas Amabilee
, Matthieu Godina, Alexandre Canvillea, Benjamin Hontonb, Jacques Monseguc, Marine Quillotd, Jacques Berlanda, Rene Koninga, Nicolas Amabilee
aDepartment of Interventional Cardiology, Clinique Saint Hilaire, Rouen, France
bDepartment of Interventional Cardiology, Clinique Pasteur, Toulouse, France
cDepartment of Interventional Cardiology, Institut Cardio-Vasculaire, Groupe Hospitalier Mutualiste Grenoble, France
dDepartment of Interventional Cardiology, Centre Hospitalier Henri Duffaut, Avignon, France
eDepartment of Interventional Cardiology, Institut Mutualiste Montsouris, Paris, France
fCorresponding Author: Quentin Landolff, Department of Interventional Cardiology, Clinique Saint Hilaire, Rouen, France
Manuscript submitted March 3, 2023, accepted March 17, 2023, published online April 8, 2023
Short title: Water PPI in the Use of Shockwave IVL
doi: https://doi.org/10.14740/cr1489
| Abstract | ▴Top |
Background: Shockwave intravascular lithotripsy (IVL) coronary system is a very useful new technology for de novo severely calcified coronary artery plaques before percutaneous coronary intervention (PCI). The device uses a semi-compliant low-pressure balloon, integrated into a sterile catheter, to deliver by vaporizing fluid an expanding bubble that generates high-pressure ultrasonic energy by waves that create multiplane longitudinal micro-macro fractures in calcified plaques, which facilitate optimal stent placement and expansion, and luminal gain.
Methods: The use of Shockwave IVL coronary system in our cardiac catheterization laboratory (Cath lab) at the “Clinique Saint-Hilaire” in Rouen, France, started in March 2019, with 42 procedures performed since this date: two patients in 2019, two patients in 2020, seven patients in 2021, 23 patients in 2022, and eight patients since the beginning of 2023.
Results: We had experienced problems at the beginning of our activity for the first 11 patients (two patients in 2019, two patients in 2020, and seven patients in 2021): after less than five pulses, the shock therapy stopped. We used initially for Shockwave IVL semi-compliant low-pressure integrated balloons a mixture of 50% contrast and 50% water preparations injectable (PPI). After changing water PPI by sodium chloride physiological saline solution, we never encountered this problem again for the following 31 patients (23 patients in 2022, and eight patients since the beginning of 2023). In fact, the proper functioning of Shockwave IVL system requires ions in balloon mixture in addition to the contrast. It is thanks to the ions contained in sodium chloride physiological saline solution that the spark necessary for shocks delivery after balloon inflation is produced.
Conclusions: Water PPI or sodium chloride physiological saline solution is used in angioplasty balloons in a lot of Cath labs worldwide. It is therefore essential to disseminate in the worldwide Cath lab the obligation to put in Shockwave IVL semi-compliant low-pressure integrated balloons sodium chloride physiological saline solution, rather than water PPI for optimal performance, and the importance of Shockwave Medical reporting this to interventional cardiologists.
Keywords: Angioplasty; Shockwave intravascular lithotripsy; Calcified coronary artery
| Introduction | ▴Top |
Shockwave intravascular lithotripsy (IVL) coronary system is a very useful new technology for de novo severely calcified coronary artery plaques before percutaneous coronary intervention (PCI). The device uses a semi-compliant low-pressure balloon, integrated into a sterile catheter, to deliver by vaporizing fluid an expanding bubble that generates high-pressure ultrasonic energy by waves that create multiplane longitudinal micro-macro fractures in calcified plaques, which facilitate optimal stent placement and expansion, and luminal gain [1].
Shockwave IVL coronary system is approved by the Food and Drug Administration (FDA) and Commission European (CE) mark, through the Disrupt CAD clinical trials, including the pivotal Disrupt CAD III study, confirm that Shockwave IVL is a safe technology with a high success rate [2].
| Materials and Methods | ▴Top |
Participants and procedure
The use of Shockwave IVL coronary system in our cardiac catheterization laboratory (Cath lab) at the “Clinique Saint-Hilaire” in Rouen, France, started in March 2019, with 42 procedures performed since this date: two patients in 2019, two patients in 2020, seven patients in 2021, 23 patients in 2022, and eight patients since the beginning of 2023.
Institutional Review Board approval
The anonymous data of our patients were retrieved via the Cardioreport software affiliated to the French “France-PCI” registry.
Ethical compliance with human study
The study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki declaration.
| Results | ▴Top |
We had experienced problems at the beginning of our activity using Shockwave IVL coronary system during balloon inflation for the first 11 patients (two patients in 2019, two patients in 2020, and seven patients in 2021). After less than five pulses, the shock therapy stopped, which we attributed to presence of air in Shockwave IVL semi-compliant low-pressure integrated balloon (Fig. 1). This problem was not resolved despite repeated balloon deflations. We subsequently encountered the same problem despite changing the batches of Shockwave IVL balloons and Shockwave IVL generator. The practice for angioplasty balloons in our Cath lab, including Shockwave IVL balloons, since our predecessors (interventional cardiologists), was to make a balloon mixture of 50% contrast and 50% water PPI. As it was a usual practice, we did not change the composition of the balloon mixture (prepared by the nurses), not even thinking that this mixture was composed of 50% water PPI and not 50% sodium chloride physiological saline solution. It was only after several weeks that we found the solution by informing us about balloon mixture used water PPI for every different angioplasty balloon in our Cath lab. After changing water PPI by sodium chloride physiological saline solution, we never encountered this problem again for the following 31 patients (23 patients in 2022, and eight patients since the beginning of 2023) (Fig. 2).
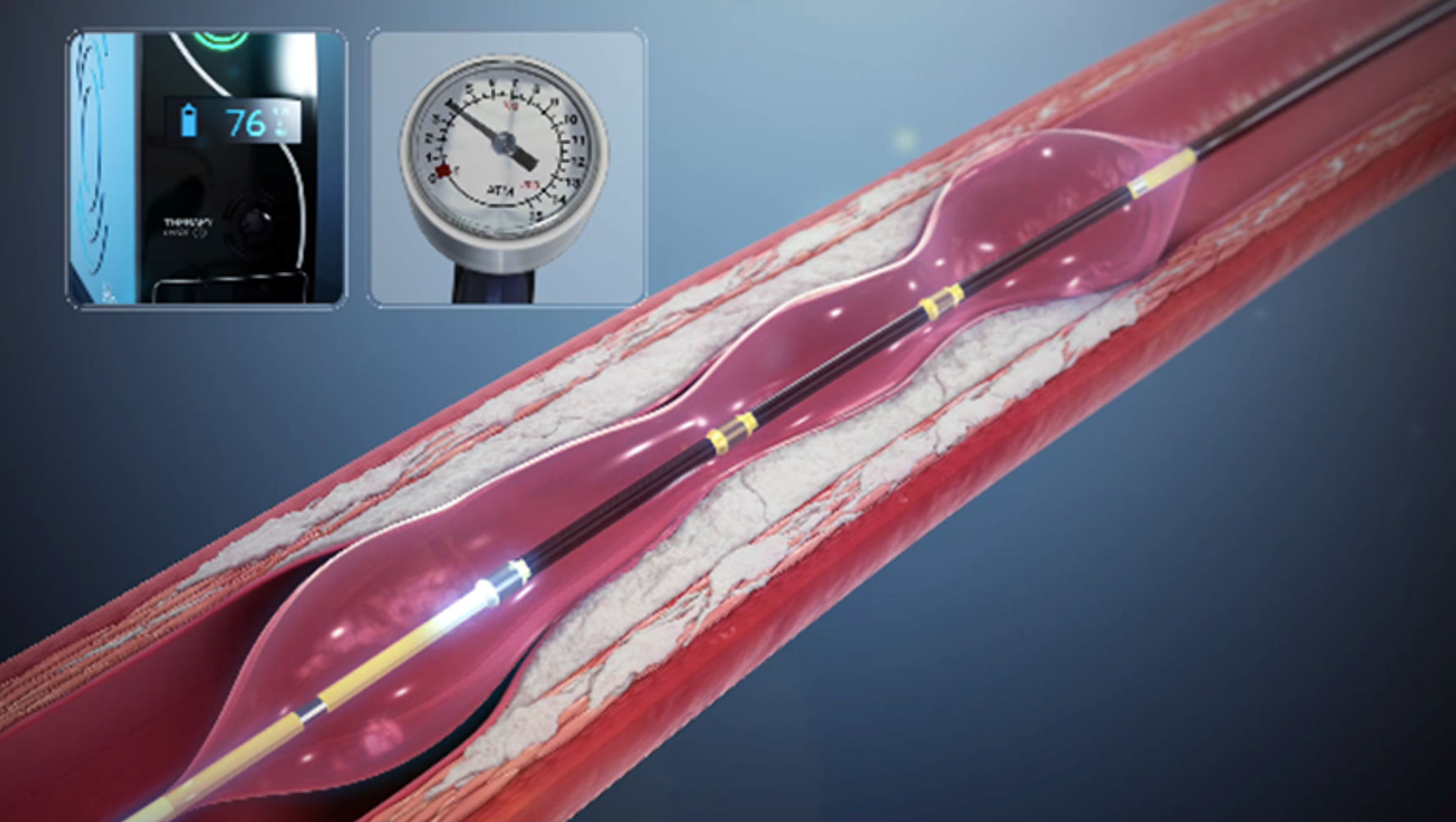 Click for large image | Figure 1. The shock therapy stopped after less than five pulses with Shockwave IVL coronary system, during inflation of Shockwave IVL semi-compliant low-pressure integrated balloon with a mixture 50% contrast and 50% water PPI for the first 11 patients (two patients in 2019, two patients in 2020, and seven patients in 2021). IVL: intravascular lithotripsy. |
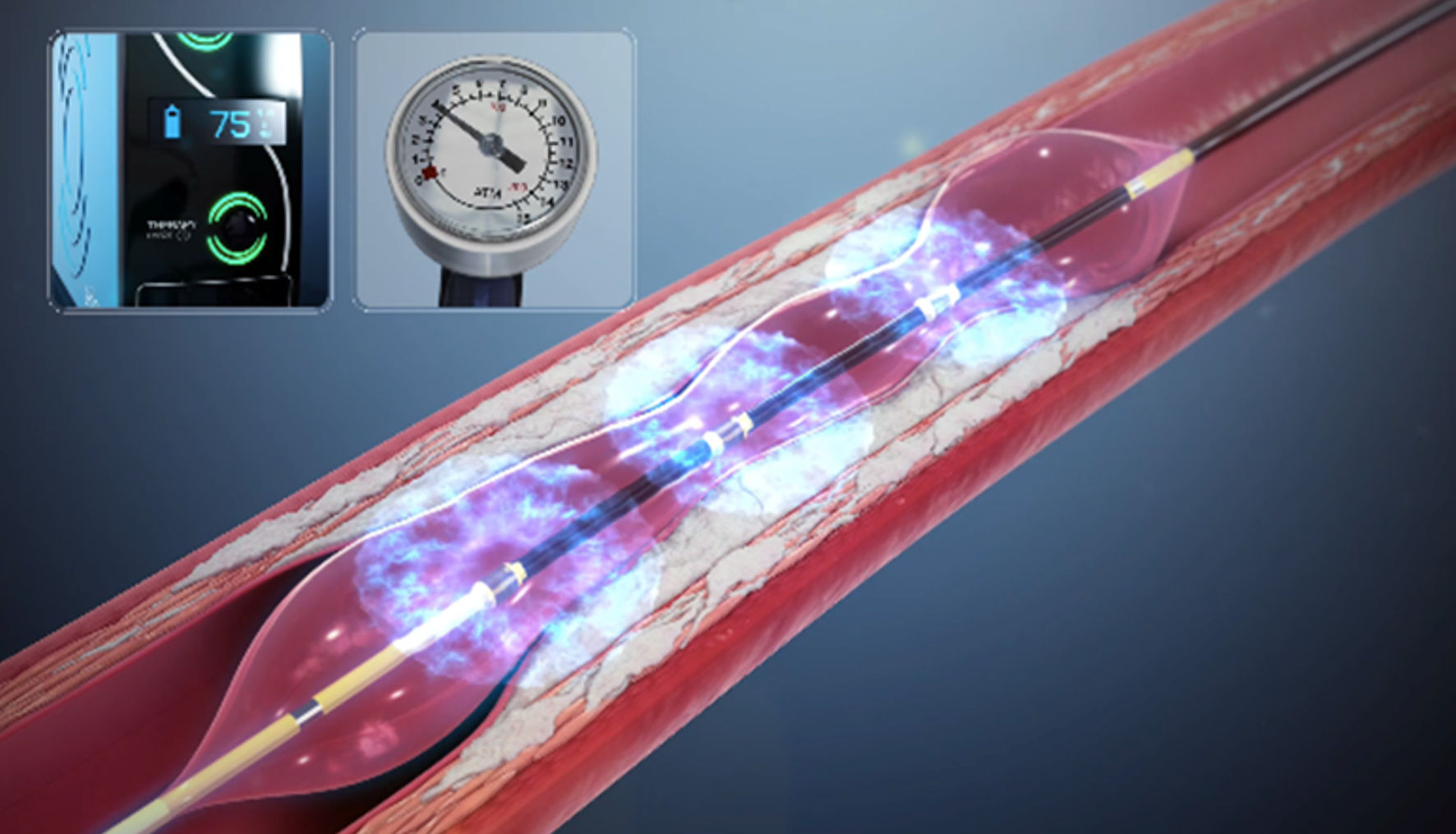 Click for large image | Figure 2. No pulse malfunction with Shockwave IVL coronary system was noted during inflation of Shockwave IVL semi-compliant low-pressure integrated balloon with a mixture 50% contrast and 50% sodium chloride physiological saline solution for the following 31 patients (23 patients in 2022, and eight patients since the beginning of 2023). IVL: intravascular lithotripsy. |
| Discussion | ▴Top |
As a matter of fact, the proper functioning of Shockwave IVL system requires ions in balloon mixture in addition to the contrast. It is thanks to the ions contained in sodium chloride physiological saline solution that the spark necessary for shocks delivery after balloon inflation is produced. Another French center encountered the same problems using a mixture of glucose serum and contrast. In fact, Shockwave Medical does not always tell interventional cardiologists what the right mixture should be.
Thus, Shockwave IVL system is composed of a generator, a connector cable, and a sterile catheter including the lithotripsy emitters in a semi-compliant low pressure integrated balloon. The lithotripsy emitters create electric sparks gaps that produce plasma vapor bubbles in the ambient fluid medium within the integrated balloon. Shockwave IVL system produces low levels of electric energy, resulting in the formation and rapid expansion of vapor bubbles, also known as cavitation bubbles, performing in acoustic pressure swells that radiate circumferentially and transmurally in an unfocused way. These acoustic pressure waves interact with high-density tissues like calcium without affecting soft tissue, because of similar acoustic impedance characteristics of water and soft tissue. These interactions break the calcium by creating micro-macro fractures, when shockwaves encounter tissue with differing acoustic impedance, such as the transition from soft to calcified tissue, and increase vessel compliance. Shockwave IVL semi-compliant low-pressure integrated balloon, available in diameters from 2.5 mm to 4 mm, with a length of 12 mm, selected in a 1:1 ratio to the reference coronary artery diameter, is able to deliver 10 pulses in each sequence at the rate of one pulse per second for a maximum of 80 pulses per sterile catheter (120 pulses for the latest generation model). The low-pressure inflation at 4 atm then 6 atm avoids the barotraumatic vessel wall injuries by stress related to high-pressure inflation. Fluid in Shockwave IVL semi-compliant low-pressure integrated balloon facilitates effective transmission of Shockwave IVL energy to vascular tissue by several mechanisms: creation of the spark which requires ions, adequate interface with analogous acoustic impedances, without thermal injury, and protecting lithotripsy emitters from direct contact with coronary artery wall. Shockwave IVL acoustics bursts, compared with orbital or rotational atherectomy, penetrate deeper into the arterial wall resulting in micro-macro fractures without affecting soft tissue [3-5].
Conclusions
Water PPI or glucose serum or sodium chloride physiological saline solution is used in angioplasty balloons in a lot of Cath lab worldwide. Because of the Shockwave IVL system operating mechanism, the delivery of pulses cannot function if the balloon contains a mixture of water PPI and contrast. It is therefore essential to disseminate in the Cath lab worldwide the obligation to put in Shockwave IVL semi-compliant low-pressure integrated balloons sodium chloride physiological saline solution rather than water PPI for optimal performance, and the importance of Shockwave Medical reporting this to interventional cardiologists.
Acknowledgments
We thank Nicolas Bussy and Ingrid Masson (Shockwave Medical) for the figures.
Financial Disclosure
BH and NA received speaker fees from Shockwave Medical. The other authors have no conflict of interest and no financial or non-financial interests that are directly or indirectly related to the work submitted for publication.
Conflict of Interest
None to declare.
Informed Consent
All the informed consents for publication were obtained.
Author Contributions
QL wrote the manuscript. MG, AC, JB, and RK participated in interventional procedures and patients’ inclusion. BH and JM did the literacy research. MQ and NA participated in the review of the article.
Data Availability
The author declares that data supporting the findings of this study are available within the article.
Abbreviations
Cath lab: catheterization laboratory; CE: Commission European; FDA: Food and Drug Administration; IVL: intravascular lithotripsy; PCI: percutaneous coronary intervention; PPI: preparations injectable
| References | ▴Top |
- Honton B, Monsegu J. Best practice in intravascular lithotripsy. Interv Cardiol. 2022;17:e02.
doi pubmed pmc - Kereiakes DJ, Di Mario C, Riley RF, Fajadet J, Shlofmitz RA, Saito S, Ali ZA, et al. Intravascular lithotripsy for treatment of calcified coronary lesions: patient-level pooled analysis of the disrupt CAD studies. JACC Cardiovasc Interv. 2021;14(12):1337-1348.
doi - Kereiakes DJ, Virmani R, Hokama JY, Illindala U, Mena-Hurtado C, Holden A, Hill JM, et al. Principles of intravascular lithotripsy for calcific plaque modification. JACC Cardiovasc Interv. 2021;14(12):1275-1292.
doi - Serruys PW, Katagiri Y, Onuma Y. Shaking and breaking calcified plaque: Lithoplasty, a breakthrough in interventional armamentarium? JACC Cardiovasc Imaging. 2017;10(8):907-911.
doi - Karimi Galougahi K, Patel S, Shlofmitz RA, Maehara A, Kereiakes DJ, Hill JM, Stone GW, et al. Calcific plaque modification by acoustic shock waves: intravascular lithotripsy in coronary interventions. Circ Cardiovasc Interv. 2021;14(1):e009354.
doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.