

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Letter to the Editor
Volume 14, Number 2, April 2023, pages 158-160

A Possible Exquisite Crosstalk of Urate Transporter 1 With Other Urate Transporters for Chronic Kidney Disease and Cardiovascular Disease Induced by Dotinurad
Hidekatsu Yanaia, b, Hiroki Adachia, Mariko Hakoshimaa, Hisayuki Katsuyamaa
aDepartment of Diabetes, Endocrinology and Metabolism, National Center for Global Health and Medicine Kohnodai Hospital, Chiba, Japan
bCorresponding Author: Hidekatsu Yanai, Department of Diabetes, Endocrinology and Metabolism, National Center for Global Health and Medicine Kohnodai Hospital, Ichikawa, Chiba 272-8516, Japan
Manuscript submitted March 14, 2023, accepted March 28, 2023, published online April 8, 2023
Short title: Inhibition of URAT1 by Dotinurad in CKD and CVD
doi: https://doi.org/10.14740/cr1496
| To the Editor | ▴Top |
We previously reported that the switching from fenofibrate to the selective peroxisome proliferator-activated receptor (PPAR) α modulator, pemafibrate, increased serum uric acid (UA) levels and reduced estimated glomerular filtration rate (eGFR) in patients with dyslipidemia [1]. Fenofibrate has a property to decrease serum UA by inhibition of urate transporter 1 (URAT1) by its major metabolite [2]. Although fenofibrate was reported to decrease the eGFR [3], the mechanism of fenofibrate-induced renal impairment has been remained unclear. Further, our previous discussion on such issue was premature [1]. Recently, the role of UA transporters has been clarified [4] (Fig. 1a). Renal excretion of UA is the major regulator of serum UA, and renal UA reabsorption is mainly mediated by URAT1 and glucose transporter 9 (GLUT9). Organic anion transporters (OATs) 1, 3 transport UA from the renal interstitial into renal proximal tubule epithelial cells. ATP-binding cassette, subfamily G, 2 (ABCG2) has been identified as a high-capacity UA exporter that mediates renal and/or extra-renal UA excretion.
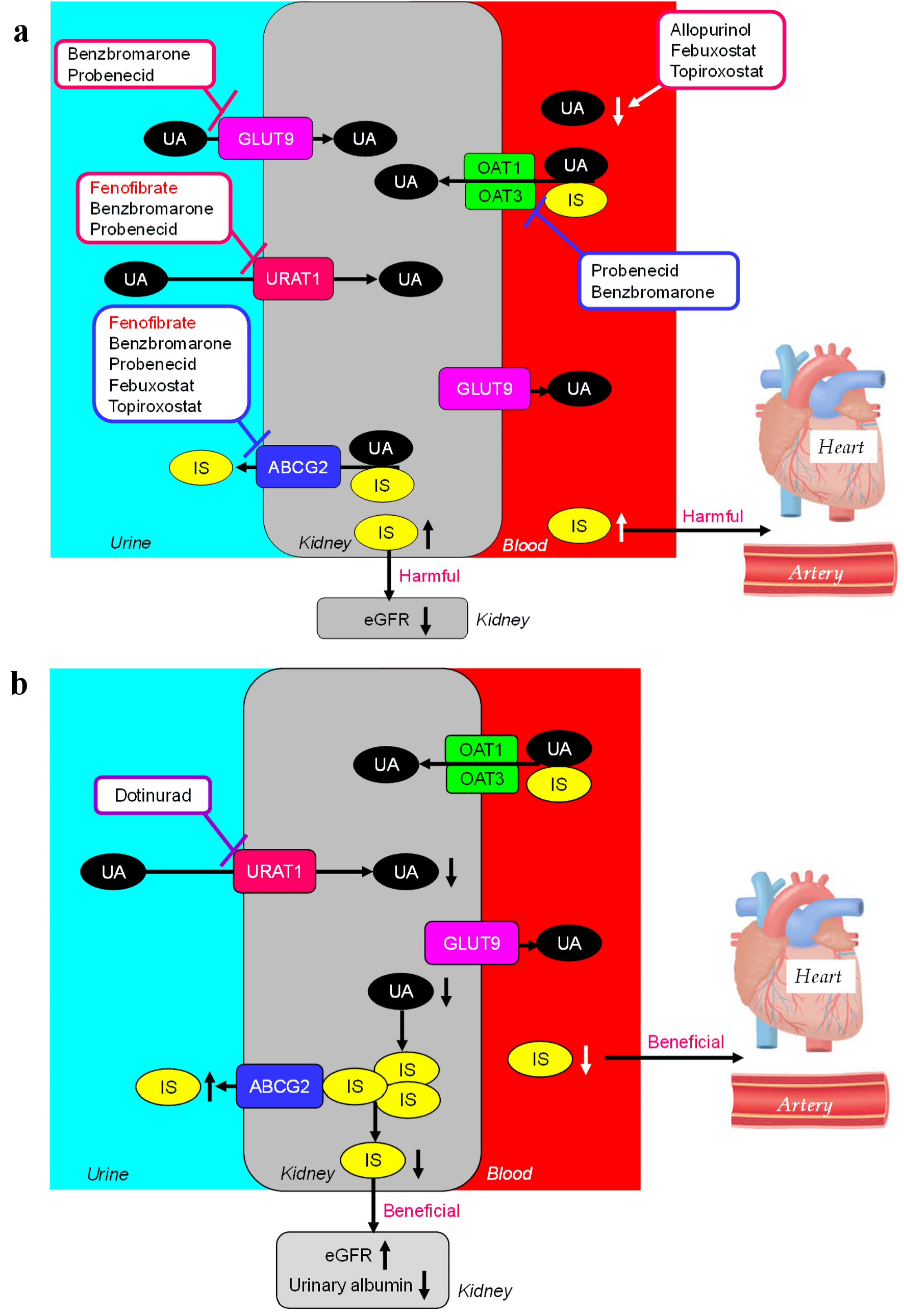 Click for large image | Figure 1. The effects of fenofibrate and uric acid (UA)-lowering drugs on UA transports and UA and indoxyl sulfate (IS) metabolism (a). The effects of dotinurad on UA transports and UA and IS metabolism (b). URAT1: urate transporter 1; OAT: organic anion transporter; GLUT9: glucose transporter 9; ABCG: ATP-binding cassette, subfamily G; eGFR: estimated glomerular filtration rate. |
Indoxyl sulfate (IS) is a well-known uremic toxin that accumulates under renal impairment and is involved in the progression of chronic kidney disease (CKD) and cardiovascular disease (CVD), by inducing inflammation and free radical production [5, 6]. IS excretion is also mediated by OAT1/3 and ABCG2 as well as UA excretion [4]. ABCG2 inhibitors, such as febuxostat (xanthin oxidase (XO) inhibitor), caused renal IS accumulation by suppressing its excretion via ABCG2 in rats [7]. Fenofibrate completely inhibits ABCG2 which may lead to increase in renal IS [8], resulting in elevation of eGFR. Another XO inhibitor, topiroxostat, also inhibits ABCG2, however, allopurinol does not inhibit ABCG2. OAT inhibitors such as probenecid (uricosuric drug, URAT1, and GLUT9 inhibitor), suppressed IS uptake into the kidney, leading to increased plasma IS [7]. Increased plasma IS may be harmful to cardiovascular system by inducing inflammation and free radical production. Benzbromarone (uricosuric drug) inhibits OAT1 and OAT3, however, its inhibitory potency for OAT1/3 is lower than those of probenecid [9], which may not lead to an increase in plasma IS. Probenecid and benzbromarone inhibit ABCG2, which may be unfavorably associated with renal function. In short, the inhibition of OAT1/3 and ABCG2 increase IS in plasma and kidney, which may be unfavorably associated with the development of CVD and CKD, respectively.
Very recently, we reported that the addition of the selective URAT1 inhibitor dotinurad to highly-evidence-proved drugs to improve CKD such as sodium-glucose cotransporter 2 (SGLT2) inhibitor and a glucagon-like peptide 1 (GLP-1) receptor agonist, improved eGFR in a diabetic patient with CKD stage G4 [10]. Dotinurad inhibits URAT1 specifically, however, does not inhibit ABCG2 [9], and reduces renal UA accumulation, which may increase the transport of renal accumulated IS by ABCG2 because UA may compete with IS for ABCG2 (Fig. 1b). This exquisite crosstalk between URAT1 and ABCG2 induced by dotinurad may be beneficially associated with the development and progression of CKD. Our recent study showed that dotinurad reduced urinary albumin creatinine ratio (UACR) and increased eGFR in patients with CKD [11], supporting our hypothesis.
Dotinurad does not inhibit OAT1/3, and then does not increase plasma IS [7]. Possibly, plasma IS may decrease when renal IS decreased because renal excretion is the major regulator of blood UA and IS. This excellent crosstalk between URAT1 and OAT1/3 induced by dotinurad may be favorably associated with the development of CVD.
In conclusion, the selective inhibition of URAT1 by dotinurad may induce favorable metabolic changes of uremic toxin, which may be beneficially associated with the development and progression of CKD and CVD.
Acknowledgments
We thank the staffs of the Division of Research Support, National Center for Global Health and Medicine Kohnodai Hospital.
Financial Disclosure
Authors have no financial disclosure to report.
Conflict of Interest
The authors declare that they have no conflict of interest concerning this article.
Informed Consent
Not applicable.
Author Contributions
HY designed the research and wrote the paper. MH, HK, and HA collected and analyzed data. All authors approved the final version of paper.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Yanai H, Katsuyama H, Hakoshima M. A significant increase of estimated glomerular filtration rate after switching from fenofibrate to pemafibrate in type 2 diabetic patients. Cardiol Res. 2021;12(6):358-362.
doi pubmed pmc - Uetake D, Ohno I, Ichida K, Yamaguchi Y, Saikawa H, Endou H, Hosoya T. Effect of fenofibrate on uric acid metabolism and urate transporter 1. Intern Med. 2010;49(2):89-94.
doi - Sica DA. Fibrate therapy and renal function. Curr Atheroscler Rep. 2009;11(5):338-342.
doi - Yanai H, Adachi H, Hakoshima M, Katsuyama H. Molecular biological and clinical understanding of the pathophysiology and treatments of hyperuricemia and its association with metabolic syndrome, cardiovascular diseases and chronic kidney disease. Int J Mol Sci. 2021;22(17):9221.
doi pubmed pmc - Barreto FC, Barreto DV, Liabeuf S, Meert N, Glorieux G, Temmar M, Choukroun G, et al. Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin J Am Soc Nephrol. 2009;4(10):1551-1558.
doi pubmed pmc - Motojima M, Hosokawa A, Yamato H, Muraki T, Yoshioka T. Uremic toxins of organic anions up-regulate PAI-1 expression by induction of NF-kappaB and free radical in proximal tubular cells. Kidney Int. 2003;63(5):1671-1680.
doi - Taniguchi T, Omura K, Motoki K, Sakai M, Chikamatsu N, Ashizawa N, Takada T, et al. Hypouricemic agents reduce indoxyl sulfate excretion by inhibiting the renal transporters OAT1/3 and ABCG2. Sci Rep. 2021;11(1):7232.
doi pubmed pmc - Miyata H, Takada T, Toyoda Y, Matsuo H, Ichida K, Suzuki H. Identification of febuxostat as a new strong ABCG2 inhibitor: potential applications and risks in clinical situations. Front Pharmacol. 2016;7:518.
doi pubmed pmc - Taniguchi T, Ashizawa N, Matsumoto K, Saito R, Motoki K, Sakai M, Chikamatsu N, et al. Pharmacological evaluation of dotinurad, a selective urate reabsorption inhibitor. J Pharmacol Exp Ther. 2019;371(1):162-170.
doi - Yanai H, Yamaguchi N, Adachi H. Chronic kidney disease stage G4 in a diabetic patient improved by multi-disciplinary treatments based upon literature search for therapeutic evidence. Cardiol Res. 2022;13(5):309-314.
doi pubmed pmc - Yanai H, Katsuyama H, Hakoshima M, Adachi H. Urate transporter 1 can be a therapeutic target molecule for chronic kidney disease and diabetic kidney disease: a retrospective longitudinal study. Biomedicines. 2023;11(2):567.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.