

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 14, Number 4, August 2023, pages 315-318

Symptomatic Bronchogenic Cyst in a Lipomatous Interatrial Septum
Alexander T. Phana, d, Janie Hua, Buzand Oganesiana, Shammah O. Williamsb, c
aDepartment of Internal Medicine, Arrowhead Regional Medical Center, Colton, CA 92324, USA
bDepartment of Cardiology, Arrowhead Regional Medical Center, Colton, CA 92324, USA
cDepartment of Cardiology, Loma Linda University, Loma Linda, CA 92305, USA
dCorresponding Author: Alexander T. Phan, Department of Internal Medicine, Arrowhead Regional Medical Center, Colton, CA 92324, USA
Manuscript submitted May 29, 2023, accepted June 1, 2023, published online July 12, 2023
Short title: Interatrial Septal Bronchogenic Cyst
doi: https://doi.org/10.14740/cr1511
| Abstract | ▴Top |
Intracardiac bronchogenic cysts are extremely rare congenital anomalies that arise during foregut development when the embryologic heart tube and ventral foregut are in close proximity to one another. We report a case of an interatrial septal bronchogenic cyst found on non-contrast enhanced computed tomography (CT) in a 66-year-old female who presented to the emergency department with chest pain. Further cardiac investigations, including contrast-enhanced CT angiogram of the heart, transthoracic echocardiogram, and transesophageal echocardiogram, revealed a cystic mass in the lipomatous interatrial septum. The patient was subsequently diagnosed with a bronchogenic cyst of the interatrial septum. No surgical intervention was pursued, as the mass remained stable, and the cardiothoracic surgeon did not recommend excision. This case highlights a rare case of a symptomatic bronchogenic cyst arising in the interatrial septum diagnosed by imaging modalities. Bronchogenic cysts should be included in the differential diagnosis of intracardiac tumors.
Keywords: Bronchogenic cyst; Interatrial septal mass; Cardiology; Internal medicine
| Introduction | ▴Top |
Cardiac neoplasms are uncommon disease entities and have variable clinical manifestations. Metastatic cardiac masses are the most common form of cardiac neoplasm. Primary cardiac tumors are rare and have an incidence of 1.38 to 30 per 100,000 people annually, with cardiac myxoma representing approximately 50% of these tumors. Intracardiac masses may be characterized and diagnosed based on imaging modalities such as echocardiography (transthoracic and transesophageal), computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET). If an intracardiac mass is resectable, tissue diagnosis may be necessary to guide medical therapy, if indicated [1].
Bronchogenic cysts are a subset of bronchopulmonary foregut malformations of the lower airways that arise from anomalous budding of the foregut during embryologic development [2]. Cardiac origins of bronchogenic cysts are explained by the proximity of the developing heart and the ventral aspect of the foregut and primitive tracheobronchial tree [3-5]. Clinical manifestations are variable and may include dyspnea, chest discomfort, and arrhythmias [3-11]. Intracardiac bronchogenic cysts are a rare anomaly and their presence in the setting of a lipomatous interatrial septum is even rarer [5]. To date, the literature is limited in the management of intracardiac bronchogenic cysts. Here, we report our findings of a rare bronchogenic cyst located in a lipomatous interatrial septum that was identified based on imaging modalities.
| Case Report | ▴Top |
A 66-year-old female with a history of hypertension, gastroesophageal reflux disorder, asthma, and major depressive disorder presented to the emergency department complaining of intermittent, exertional, and non-pleuritic substernal chest pain for 3 days. She described her pain as 5/10 in intensity, non-positional, not associated with food intake, and tight in nature. She reported having similar episodes for the past 5 months. She denied subjective fevers, cough, dyspnea, palpitations, diaphoresis, edema, fatigue, and weight loss. Her home medications included sumatriptan, cetirizine, omeprazole, albuterol, and amlodipine. Her past surgical history included a prior uncomplicated tubal ligation. She had a 20 pack-year smoking history, drank two servings of alcohol daily, and denied illicit substance use.
Initial vital signs included a blood pressure of 142/83 mm Hg, pulse rate of 67, respiratory rate of 18, temperature of 37 °C, and oxygen saturation of 99% on ambient air. Her physical examination was only notable for an irregularly irregular cardiac rhythm. Due to concerns for possible acute coronary syndrome, the patient was given aspirin 325 mg orally and nitroglycerin 0.4 mg sublingually, while awaiting the remainder of her diagnostic workup. The aforementioned medications did not appear to alleviate her chest discomfort. An electrocardiogram (ECG) obtained at that time revealed atrial fibrillation without rapid ventricular response or ischemic changes, as did serial ECGs. The anterior-posterior chest X-ray was unremarkable. Serum electrolytes, urinalysis, urine toxicology, blood counts, troponin-I, and brain natriuretic peptide were within normal limits. The patient underwent a computed tomography (CT) scan of the chest without intravenous (IV) contrast, which revealed a 1.8 × 1.8 cm hyperattenuating focus within the heart in the region of the right atrium; no pulmonary emboli were noted. Of note, nuclear perfusion scan with technetium-99 sestamibi (Cardiolite) 2 years prior demonstrated no reversible perfusion defects on cardiac stress and at rest, and a non-contrast enhanced CT scan of the chest 1 year prior was unremarkable. As acute coronary syndrome had been ruled out, the patient was discharged with a diagnosis of cardiac mass with close outpatient follow-up.
Following this, the patient followed up with her primary care physician and was referred to cardiology for further workup of her cardiac mass. The patient underwent a transthoracic echocardiogram (TTE) with agitated saline contrast study, which demonstrated normal bilateral ventricular size and function, estimated left ventricular ejection fraction of 70%, non-elevated right ventricular systolic pressure, no abnormal shunting across the atrial septum, and no evidence of atrial septal defect or patent foramen ovale. Following this, the patient underwent a contrast-enhanced CT scan of the chest that revealed a mass of the interatrial septum measuring 2.61 × 3.59 cm, without mediastinal lymphadenopathy (Fig. 1). For better characterization of the mass, the patient underwent a transesophageal echocardiogram (TEE) enhanced with IV perflutren lipid microspheres (Definity), which demonstrated a lipomatous interatrial septum with a cystic mass with mucinous material of the interatrial septum that was predominantly right-sided (Supplementary Material 1, www.cardiologyres.org).
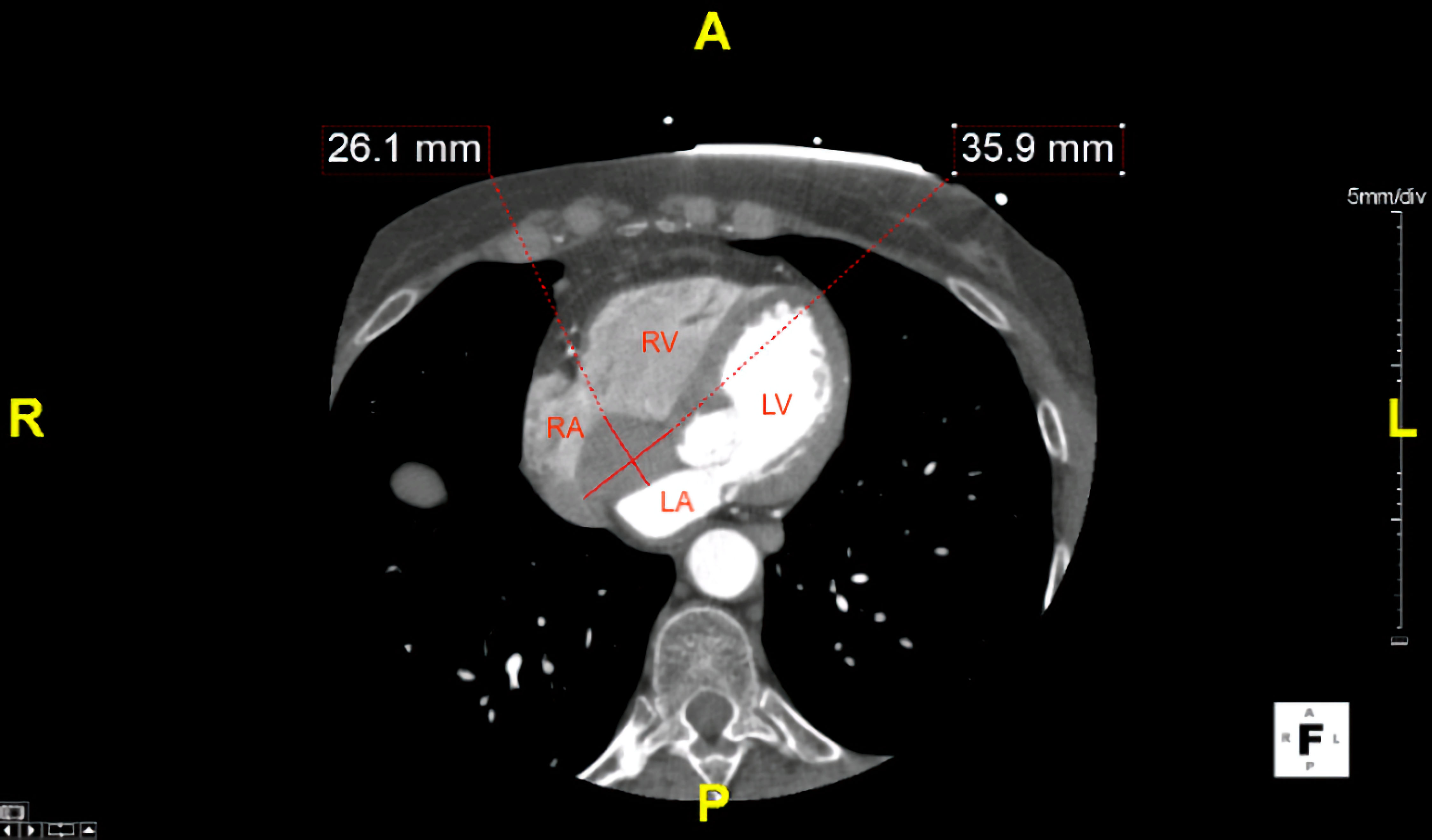 Click for large image | Figure 1. Axial section of a computed tomography of the chest with intravenous contrast demonstrating a 2.61 × 3.59 cm interatrial cardiac mass. RA: right atrium; RV: right ventricle; LA: left atrium; LV: left ventricle. |
The patient was then referred to a cardiothoracic surgeon and underwent a repeat TEE, which demonstrated a stable 2.7-cm diameter cystic mass of the posterior inferior portion of the interatrial septum projecting into the right atrium (Supplementary Material 2, www.cardiologyres.org). This same imaging study did not demonstrate color Doppler evidence of obstructive flow across the mitral and tricuspid valves as well (Supplementary Material 3, www.cardiologyres.org). The cardiothoracic surgeon decided not to proceed with surgical intervention, as the mass was stable and not causing any further symptoms for the patient, and recommended surveillance with TTEs at 6-month intervals. At 5-year follow-up, the patient has not had persistent symptoms of chest pain and the intracardiac mass has not grown in size.
| Discussion | ▴Top |
Bronchogenic cysts are benign tumors that rarely cause symptoms [9]. Bronchogenic cysts of intracardiac origin are rare and thought to arise when a segment of the tracheobronchial tree incorrectly buds into the cardiac primordia during pulmonary branching during the third week of embryogenesis, laying rest in cardiac tissue [2, 5, 9]. Most cardiac bronchogenic cysts present in the pericardium, with rare occurrence in the interatrial and interventricular septa [4, 6, 12]. The differential diagnoses of intracardiac lesions with cystic appearance include post-traumatic cyst, hydatid cyst, cor triatriatum, epicardial cyst, teratomas, cystic tumor of the atrioventricular nodal region, and cavernous lymphangioendothelioma [6, 9]. Although interatrial masses may not be cystic in nature, other differential diagnoses should include thrombi, myxomas, lipomas, fibroma, fibroelastomas, rhabdomyomas, and metastatic tumors [6, 9]. As this mass was near the vicinity of the right atrium, a cardiac myxoma was in the differential diagnosis; however, myxomas tend to grow in size over time. Since our patient’s mass was stable in size at 5-year follow-up, cardiac myxoma is unlikely.
It has been classically recommended that all bronchogenic cysts should be surgically resected for histologic diagnostic and therapeutic purposes [4, 7, 9, 11]. Upon biopsy, bronchogenic cysts are identified by their typical mucinous fluid and ciliated columnar or cuboidal epithelium [2, 7]. However, because the clinical course of bronchogenic cysts is typically indolent, the decision for surgical intervention should be individualized, as mass effect of the cyst may not necessarily cause adverse manifestations in all patients. Furthermore, biopsy of the cyst is a potentially dangerous procedure that can put the patient at risk for suppuration and embolization [3, 6, 7, 12].
Imaging findings of intracardiac bronchogenic cysts have been established, as most of these lesions are initially detected on chest CT, TTE, TEE, and MRI [3-12]. Radiologic findings typically describe a cystic homogenous mass, isointense tumor on T1-weighted MRI, and high-intensity tumor on T2-weighted MRI [4-12]. Though these imaging findings have aided in the diagnosis of intracardiac bronchogenic cysts, the literature has a dearth in the number of cases diagnosed without biopsy, even though a majority of these cysts are now being diagnosed preoperatively [5, 10]. In our case, two TEEs and a CT angiogram of the heart were sufficient to diagnose a bronchogenic cyst, given the imaging characteristics noted. Further, based on shared decision making between providers and the patient, a biopsy of the mass would not have provided any changes to the patient’s management, as it was stable on repeat imaging. Consequently, a surgical resection was not pursued. We also did not obtain an MRI due to cost and the overwhelming evidence found on TEE and CT angiogram of the heart. Thus, to prevent adverse patient outcomes, physicians should take into account the patient’s clinical manifestations and supporting radiological findings prior to considering the need for surgical intervention. In our patient’s case, imaging modalities were sufficient in the diagnosis and management of her interatrial bronchogenic cyst, and future studies may aim to assess the feasibility of avoiding unnecessary surgical intervention to diagnose intracardiac bronchogenic cysts.
Conclusions
Bronchogenic cyst of the interatrial septum rarely occurs and seldom causes symptoms. Most of these lesions are incidental findings on CT scan of the chest and further visualized with TEE and MRI; however, TEE is more cost-efficient. Consequently, we recommend that asymptomatic patients should be followed by surveillance TTEs and consistent outpatient cardiology observation. Surgical excision of intracardiac bronchogenic cysts is controversial and should only be done if patients are presenting with clinical manifestations directly caused by mass effect or if the lesion continues to grow. Further studies should assess the proficiency of MRI versus cardiac CT versus TEE in diagnosis of intracardiac bronchogenic cysts.
| Supplementary Material | ▴Top |
Suppl 1. Mid-esophagus four-chamber view of a TEE demonstrating an interatrial septal cystic mass.
Suppl 2. Mid-esophagus four-chamber view of a repeat TEE demonstrating a 2.7-cm diameter interatrial septal cystic mass protruding into the right atrium.
Suppl 3. Mid-esophagus four-chamber view of a TEE demonstrating non-obstructive mitral and tricuspid valvular flow.
Acknowledgments
The authors would like to thank and express their gratitude to Arrowhead Regional Medical Center’s exceptional nursing staff and unit managers for their expert clinical support.
Financial Disclosure
The authors have no financial or funding disclosures.
Conflict of Interest
The authors declare there is no conflict of interest.
Informed Consent
Informed consent was obtained from the family of the patient. The patient was also appropriately deidentified for this manuscript.
Author Contributions
ATP, JH, and BO contributed to the initial manuscript write-up, literature review, and editing of the manuscript. SOW attended on the case and contributed to decision-making, management of the patient, literature review, and editing of the manuscript.
Data Availability
Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
Abbreviations
ECG: electrocardiogram; CT: computed tomography; MRI: magnetic resonance imaging; PET: positron emission tomography; IV: intravenous; TTE: transthoracic echocardiogram; TEE: transesophageal echocardiogram
| References | ▴Top |
- Poterucha TJ, Kochav J, O'Connor DS, Rosner GF. Cardiac tumors: clinical presentation, diagnosis, and management. Curr Treat Options Oncol. 2019;20(8):66.
doi pubmed - Berrocal T, Madrid C, Novo S, Gutierrez J, Arjonilla A, Gomez-Leon N. Congenital anomalies of the tracheobronchial tree, lung, and mediastinum: embryology, radiology, and pathology. Radiographics. 2004;24(1):e17.
doi pubmed - Vaideeswar P, Agnihotri MA, Patwardhan AM. Intracardiac bronchogenic cyst. J Card Surg. 2011;26(3):266-268.
doi pubmed - Wang J, Zhu Q, Liang B, Shi H, Han P, Kong X. Left ventricular bronchogenic cyst. Ann Thorac Surg. 2016;101(2):744-746.
doi pubmed - Jiang H, Wang H, Wu H, Li X. Bronchogenic cyst of the interatrial septum. J Cardiothorac Surg. 2013;8:171.
doi pubmed pmc - Borges AC, Knebel F, Lembcke A, Panda A, Komoda T, Hiemann NE, Meyer R, et al. Bronchogenic cyst of the interatrial septum presenting as atrioventricular block. Ann Thorac Surg. 2009;87(6):1920-1923.
doi pubmed - Fukada Y, Endo Y, Nakanowatari H, Kitagawa A, Tsuboi E, Irie Y. Bronchogenic cyst of the interatrial septum. Fukushima J Med Sci. 2020;66(1):41-43.
doi pubmed pmc - Miwa E, Tani T, Okada Y, Furukawa Y. A rare cardiac tumor: Bronchogenic cyst of interatrial septum. Echocardiography. 2017;34(3):474-475.
doi pubmed - Seo N, Kang JW, Lim CH, Kim B, Lee HJ, Lim TH. CT findings of an intracardiac bronchogenic cyst. Int J Cardiovasc Imaging. 2011;27(5):701-704.
doi pubmed - Park J, Cho GY, Park KH, Oh IY. Intracardiac bronchogenic cyst: report of a growing lesion. Circulation. 2014;130(13):1107-1109.
doi pubmed - Forcillo J, Dion D, Sauvageot C, Jeanmart H. Intraventricular bronchogenic cyst: a rare congenital anomaly. Ann Thorac Surg. 2015;100(3):1101-1103.
doi pubmed - Kawase Y, Takahashi M, Takemura H, Tomita S, Watanabe G. Surgical treatment of a bronchogenic cyst in the interatrial septum. Ann Thorac Surg. 2002;74(5):1695-1697.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.