

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 14, Number 5, October 2023, pages 351-359

Influence of Daily Aerobic Exercise Duration on Phase 2 Cardiac Rehabilitation at a Rehabilitation Hospital and Health-Related Quality of Life After Discharge
Tomohiro Matsuoa, b, Takuro Ohtsuboa, b, Tomoki Yanasea, b, Katsuhiro Uenoa, Shuichi Kozawac, Takako Matsubarab, Yosuke Morimotoa, b, d
aDepartment of Rehabilitation, Nishi Memorial Port-island Rehabilitation Hospital, Kobe 650-0046, Japan
bFaculty of Rehabilitation, Kobe Gakuin University Graduate School, Kobe 651-2180, Japan
cDepartment of Cardiology, Nishi Memorial Port-island Rehabilitation Hospital, Kobe 650-0046, Japan
dCorresponding Author: Yosuke Morimoto, Faculty of Rehabilitation, Kobe Gakuin University Graduate School, Kobe 651-2180, Japan
Manuscript submitted June 15, 2023, accepted July 28, 2023, published online August 22, 2023
Short title: Aerobic Exercise and HR-QoL After Discharge
doi: https://doi.org/10.14740/cr1527
| Abstract | ▴Top |
Background: Phase 2 in-patient cardiac rehabilitation (CR) at a rehabilitation hospital is now added the medical service fees in Japan and in light of the recent reimbursement for CR, a study needed to be performed to determine exertional exercise on its effectiveness and benefits to patients. We examined the effects of daily aerobic exercise duration on health-related quality of life (HR-QoL) at 6 months after discharge from phase 2 CR.
Methods: Of the 54 consecutive cardiovascular disease patients admitted to a rehabilitation hospital after acute care, 43 were considered acceptable candidates for enrollment according to predetermined inclusion and exclusion criteria. Of these, 40 patients completed study requirements, including return of a questionnaire on HR-QoL survey 6 months after discharge. The primary outcome was HR-QoL as evaluated using the EuroQol five-dimension five-level (EQ-5D-5L). Two multiple regression models were constructed to assess the influences of daily aerobic exercise duration (content of rehabilitation) and other clinicodemographic variables assessed during acute care (model 1) or at transfer from acute care to a rehabilitation hospital (model 2).
Results: Both model 1, which included age, Barthel index of daily function before hospitalization, and daily aerobic exercise duration in the rehabilitation hospital (R2 = 0.553, P < 0.001), and model 2, which included New York Heart Association functional classification at transfer, Charlson comorbidity index at transfer, and daily aerobic exercise duration (R2 = 0.336, P = 0.002) identified aerobic exercise duration as a significant independent factor influencing HR-QoL at 6 months post-discharge (model 1: P = 0.041; model 2: P = 0.010).
Conclusions: Enhanced daily aerobic exercise content during phase 2 in-hospital CR can significantly improve longer-term HR-QoL among cardiovascular disease patients independently of other clinicodemographic factors, including age, activities of daily living before treatment, and baseline condition at rehabilitation onset. These findings, that in the small sample size, support the continued expansion of phase 2 CR at a rehabilitation hospital in Japan.
Keywords: Aerobic exercise; Health-related quality of life; Phase 2 cardiac rehabilitation; Rehabilitation hospital
| Introduction | ▴Top |
The primary goals of rehabilitation following significant cardiac events (cardiac rehabilitation, CR) are prevention of recurrence or rehospitalization and restoration of physical function, and treatment strategies have been proposed in Japan to achieve these outcomes at different CR phases [1]. However, with rapid population aging in Japan and major advances in cardiovascular disease treatment, a growing number of patients entering phase 1 CR are highly deconditioned, have multiple comorbidities, and (or) demonstrate impaired activities of daily living (ADLs) [2]. These patients have difficulty recovering ADLs and other physical functions and exhibit low exercise tolerance during brief phase 1 CR. Cardiovascular diseases were recent added as one of the requirements for calculating the convalescent rehabilitation coverage in the FY 2022 Revision of Medical Fees. To improve rehabilitation outcome, a phase 2 CR program at a rehabilitation hospital has been added to the medical service fees that includes comprehensive physical, occupational, and speech therapy for up to 3 h per day during a maximum 90-day stay. The main objectives of this phase 2 CR are to achieve home discharge by phase 2 CR as well as to improve health-related quality of life (HR-QoL) after home discharge, as poor HR-QoL is associated with an increased risk of all-cause death and combined cardiac death/rehospitalization for heart failure [3]. Although many reports have shown that CR is effective in improving HR-QoL [4], there have been no studies focused specifically on components of the Japanese phase 2 CR delivered in rehabilitation hospitals.
The guidelines of the Japanese Circulation Society [5] recommend moderate-intensity endurance training during CR given the high-level evidence for therapeutic efficacy, but again there are few reports directly assessing the effectiveness of this CR component in rehabilitation hospitals [6]. Two critical parameters influencing the therapeutic efficacy of aerobic exercise are the intensity and duration (which can be carefully monitored in rehabilitation hospitals). HR-QoL is influenced by numerous factors in addition to the amount of aerobic exercise performed in the rehabilitation hospital, including general health condition before and during hospitalization. Therefore, the purpose of this study was to examine the effects of aerobic exercise duration on HR-QoL after discharge from in-patient phase 2 CR while considering other clinicodemographic factors before and during hospitalization in the outcome model analysis.
| Materials and Methods | ▴Top |
Study design and study population
This prospective cohort study was conducted from November 2020 to May 2022. The participants were patients who received conservative or surgical treatment for cardiovascular diseases at an acute care hospital and were subsequently transferred to Nishi Memorial Port-island Rehabilitation Hospital for phase 2 CR. Patients were excluded if they were younger than 18 years, had limited walking ability due to cerebrovascular diseases, severe disturbance of consciousness, tetraplegia or paraplegia, spinal cord infarction, critical limb ischemia, or absence of a lower extremity, or if they refused to participate. In addition, patients were excluded if they died during hospitalization, were unable to continue in-patient treatment, were transferred to an acute care hospital, or prevented assessment. This study was approved by the ethics committee of Nishi Memorial Port-island Rehabilitation Hospital (Approval No: 13) and Kobe Gakuin University (Approval No: 22-01), and written informed consent was obtained from each patient. The present study also complied with the principles of the Declaration of Helsinki regarding investigations on human subjects.
Data before hospitalization and upon transfer to the rehabilitation hospital
The information prior to admission to an acute care hospital, as the presence of caregivers, Barthel index (BI) as an indicator for ADL [7], and Kihon checklist as an assessment of frailty were collected [8]. Clinical and demographic information collected on transfer to the rehabilitation hospital were as follows: age, gender, body mass index, reason for CR (heart failure, ischemic heart disease (angina pectoris, acute coronary syndrome), cardiovascular surgery (coronary artery bypass grafting, valvular surgery, or both), aortic surgery (aortic vascular replacement, stent grafting, or both), combined cardiovascular and aortic surgery), New York Heart Association functional classification (NYHA class), Charlson comorbidity index (CCI), left ventricular ejection fraction (LVEF) as determined by Simpson’ method, left atrial dimension, early diastolic transmitral flow velocity to early diastolic mitral annular tissue velocity ratio (E/e’), biochemical test data (serum hemoglobin, albumin, C-reactive protein, and B-type natriuretic peptide), estimated glomerular filtration rate, and length of stay in the acute care hospital. The length of stay in the rehabilitation hospital and aerobic exercise duration per day were also recorded.
Assessments during in-patient rehabilitation
ADLs were assessed at the time of transfer to the rehabilitation hospital and at discharge by a trained physical therapist and an occupational therapist using the functional independence measure (FIM) [9]. The FIM is an 18-item scale that assesses the degree of independence or assistance needed by a person to perform various motor tasks (13 items) and cognitive tasks (five items) in daily living. Each item was scored on a seven-point Likert scale from complete dependence on assistance (1) to complete independence (7). Thus, lower scores indicate poorer ADL.
To evaluate physical function, we measured handgrip strength, knee extension strength, gait speed, and short physical performance battery (SPPB) performance at admission and discharge from the rehabilitation hospital. Hand grip strength was measured twice using a digital handgrip meter (T-2177, TOEI LIGHT Co., Ltd) and the higher value recorded for analysis. Knee extension strength was measured using a hand-held dynamometer (µTas F-1, Anima Co., Ltd). Briefly, measurements of isometric knee extension strength were performed at 90° of knee flexion in a sitting posture, and two measurements were conducted after the orientation and one practice exercise. The higher value was then divided by body weight (BW) as the correction value (%BW). Gait speed was assessed as a comfortable walking speed of over 10 m and was converted to m/s. The SPPB was administered as described by Guralnik et al [10]. Briefly, we calculated the overall score for balance ability, 4-m walking time, and 5-repetition sit-to-stand time. To evaluate exercise tolerance, we administered the 6-minute walk test (6MWT) at transfer and discharge. The 6MWT was performed in a 20-m straight line with no steps or obstacles, and the maximum distance walked in 6 min was recorded in accord with the standards of the America Thoracic Society [11]. Patients received a full explanation of all tasks prior to testing.
Cognitive function was assessed using the Japanese version of the mini-mental state examination (MMSE) [12]. The MMSE scale ranges from 0 to 30 points, with higher scores indicating better cognitive function.
Data collection after discharge from a rehabilitation hospital
At 6 months after discharge from the rehabilitation hospital, a letter was sent to the patients to confirm survival, hospital readmission status, and HR-QoL. We measured HR-QoL using the EuroQol five-dimension five-level (EQ-5D-5L) instrument and the EQ-5D-5L index value calculator version 2.0 [13]. The EQ-5D-5L was developed as a general instrument (not specific to any single disease) to complement existing HR-QoL measures [14]. The items provide information on five domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each item is answered using a five-point categorical rating scale ranging from “no problems at all” to “extreme problems (unable to do)”, and recoded from 0 (dead) to 1 (full health). A Japanese version of the EQ-5D-5L developed by Tsuchiya and colleagues was used in the present study [15].
CR
The CR program was created based on the guidelines of the Japanese Circulation Society [5]. Exercise programs in CR focus on aerobic exercise, resistance training, and stretching [16]. The “quantity” of aerobic exercise is a composite of frequency, intensity, time, type, volume, and progression/revision (FITT-VP) [16]. Although cardiopulmonary exercise testing based on anaerobic thresholds is recommended for determining exercise intensity [16], this is often not feasible for patients transferred to a rehabilitation hospital due to significant decline in ADL, stroke, or coexisting musculoskeletal disease. Therefore, we mainly used the Borg scale [17] for rating perceived exertion and the talk test for monitoring relative intensity [18]. The intensity and duration of exercise were increased or decreased in response to changes in the patient’s medical condition. The total aerobic exercise duration was obtained from medical records and divided by the length of hospital stay to calculate average aerobic exercise duration per day. Individualized rehabilitation programs such as ADL and balance training were also provided every day for up to 3 h per day according to the patient’s condition. In addition, patient education, which is an essential component of CR to improve HR-QoL [19, 20], was provided generously to all patients during their hospitalization. Finally, speech therapy was performed if deemed necessary by the attending physician.
Statistical analysis
Clinicodemographic parameters following CR were compared to pre-intervention baseline values using the paired-sample t-test or Wilcoxon signed-rank test as appropriate. Two multiple regression models were constructed to identify variables associated with HR-QoL 6 months after discharge, one including daily aerobic exercise duration plus preadmission variables (model 1) and the other including daily aerobic exercise duration plus variables measured at transfer to the rehabilitation hospital (model 2). Candidate factors for multiple linear regression were selected according to a literature review and clinical expertise. The sample size was based on the number of factors suitable for multivariate analysis, as reported by Peter et al [21]. All analyses were performed using the Statistical Package for the Social Sciences version 25.0 (IBM Corp., Armonk, NY, USA). A P < 0.05 was considered statistically significant for all tests.
| Results | ▴Top |
Patient demographics
A total of 54 patients transferred to a rehabilitation hospital after acute care for cardiovascular diseases were identified as potential candidates for this study, of which 40 meeting inclusion and exclusion criteria and completing the EQ-5D-5L at 6 months after discharge were included in the analysis. The flowchart of participants throughout the study is illustrated in Figure 1, and patient baseline characteristics are summarized in Table 1. The FIM, SPPB, gait speed test, hand grip strength test, knee extensor strength test, MMSE, and 6MWT were administered on admission and at discharge, and all were significantly improved following the phase 2 rehabilitation program (Table 2).
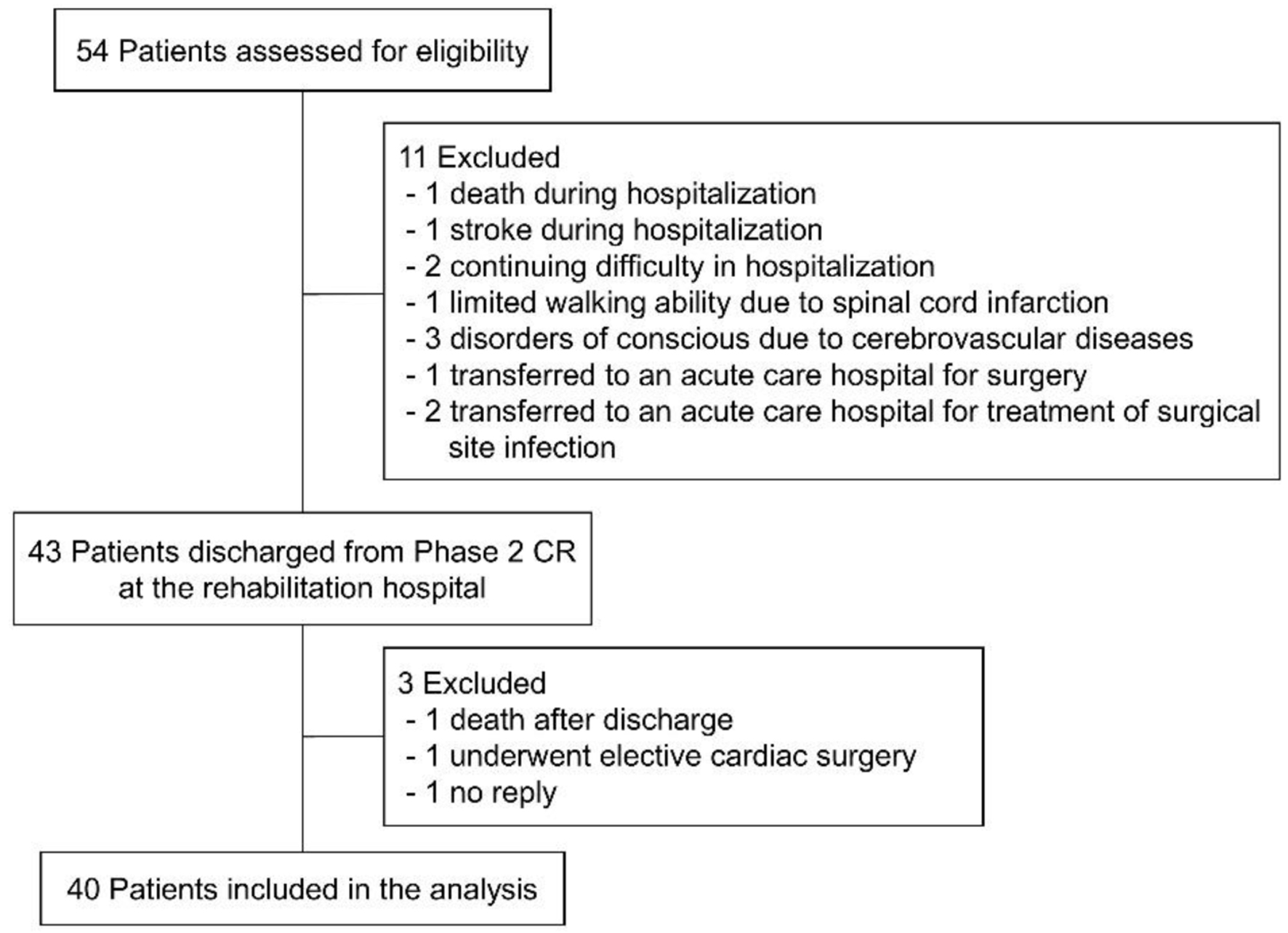 Click for large image | Figure 1. Flowchart of study participation and exclusion. |
 Click to view | Table 1. Baseline Characteristics of the Study Patients |
Click to view | Table 2. Changes in ADL, Physical Function, Cognitive Function, and Exercise Tolerance After Rehabilitation |
Rehabilitation dose
Mean daily aerobic exercise duration was 19.2 ± 19.0 min/day, total average daily in-patient rehabilitation time was 131.2 ± 17.1 min, and the mean length of hospitalization was 57.4 ± 28.0 days (Table 1).
HR-QoL at 6 months post-discharge
One patient died during the study period, and three required readmissions to an acute care hospital due to cardiovascular diseases. The EQ-5D-5L score 6 months after discharge was 0.696 ± 0.235. The results of multiple regression analysis for the EQ-5D-5L 6 months after discharge are shown in Table 3. Variables were selected by the forced entry method, and multivariate analysis was performed using two models. Model 1 included age, BI before hospitalization, and mean daily aerobic exercise duration in the rehabilitation hospital as independent variables, while model 2 included NYHA class and CCI at transfer as well as mean daily aerobic exercise duration. According to model 1 (R2 = 0.553, P < 0.001), both BI before hospitalization (P < 0.001) and mean daily aerobic exercise duration (P = 0.041) were significant independent factors influencing HR-QoL at 6 months post-discharge, while in model 2 (R2 = 0.336, P = 0.002), mean daily aerobic exercise duration was the only significant independent factor influencing HR-QoL (P = 0.010).
Click to view | Table 3. Multiple Regression Analysis of Factoring Influencing EQ-5D-5L at 6 Months Post-Discharge |
| Discussion | ▴Top |
Few studies have evaluated the long-term efficacy of in-patient phase 2 CR after acute care for cardiovascular diseases. This study is the first to report that longer daily aerobic exercise duration as a component phase 2 CR results in better post-discharge HR-QoL.
Most of subjects in this study were elderly and female, with relatively normal cardiac function and moderate heart failure severity. Also, more than 70% were postoperative patients. These characteristics (Table 1) are likely representative of the typical phase 2 CR population as the recovery process after cardiac surgery is prolonged among the elderly [22] and these institutions specialize in treating patients who cannot be discharged home after acute care alone but are sufficiently stable for chronic treatment.
The EQ-5D-5L at 6 months after discharge was 0.696 ± 0.235, lower than the average values reported by Shiroiwa et al [23] for community-dwelling Japanese in their 70s (male: 0.889 ± 0.154, female: 0.876 ± 0.157) and 80s (male: 0.821 ± 0.203, female: 0.774 ± 0.220). In their study, it was proposed that comorbidities such as stroke, Parkinson’s disease, and depression, as well as symptoms such as chest pain, breathlessness, swelling or heaviness of legs, and limb motion problems could account for the decline in EQ-5D-5L. Therefore, it is possible that cardiovascular disease-induced physical dysfunction, exercise intolerance, and disease symptoms reduced HR-QoL after discharge from phase 2 CR in rehabilitation hospitals. Surprisingly, however, average HR-QoL was also lower than reported previously following discharge from cardiac surgery [24], even though most patients in the current study cohort were recovering from cardiac surgery, possibly because these patients were older and included a greater proportion of NYHA class 3 or higher. Indeed, the same study [24] reported that older patients and those with ischemic heart disease did not improve to the minimal clinical important difference (MCID), so improving HR-QoL after discharge may be difficult. Nonetheless, we found that a longer duration of aerobic exercise during phase 2 CR had lasting beneficial effects on HR-QoL despite these impediments to recovery.
Two separate multiple regression analysis with HR-QoL after discharge as the dependent variable identified longer daily aerobic exercise duration in the rehabilitation hospital as an independent predictor of improved HR-QoL. Beta-blockers did not affect the primary outcome. Aerobic exercise improves exercise tolerance [25, 26] and the metabolic capacity of skeletal muscle [27], which allows for increased daily physical activity [26]. Greater exercise tolerance and metabolic capacity also enhance self-efficacy [28], which in turn can promote continuation of aerobic exercise [29] and further improve HR-QoL [30]. Thus, sustained physical activity after discharge may have improved HR-QoL in the months after discharge. Future investigations are warranted to assess the overall duration of this improvement and determine whether outpatient programs can further conserve these health gains.
Many previous reports have shown that aerobic exercise-based CR can effectively improve HR-QoL [4, 31], and indeed one of the main goals of CR for patients with coronary artery disease and heart failure is to improve HR-QoL [5]. It has also been reported that aerobic exercise early after cardiac surgery and aerobic exercise significantly improve HR-QoL and exercise tolerance 6 months after valvular surgery [32, 33]. Although the overall benefits of aerobic exercise and dependence on timing of initiation and intensity have been reported, this is among the first studies to examine the effect of daily aerobic exercise duration as part of phase 2 CR on longer-term HR-QoL. Our results suggest that longer daily aerobic exercise as part of phase 2 in-patient CR at rehabilitation hospitals can substantially improve HR-QoL after discharge.
ADL score before admission was also an independent predictor of better HR-QoL in the model including pre-hospitalization clinicodemographic parameters (model 1), possibly due to disease-related ADL decline and subsequent improvement of physical function by acute care treatment and rehabilitation. In older patients, functional limitations due to long-term illness have a four-fold greater impact on HR-QoL than the illness alone [34]. Thus, the decrease in ADL prior to treatment likely reduced baseline HR-QoL independently of phase 2 CR.
These findings suggest that continued CR at a rehabilitation hospital can improve ADL, physical function, cognitive function, and exercise tolerance. In fact, the benefits of CR on physical function and exercise tolerance in this study exceeded those previously reported (below MCID) [35-38]. The average daily CR time in this study was approximately 130 min, longer than previous studies due to the greater availability of intensive rehabilitation facilities and staff compared to acute care hospitals. However, a systematic review and meta-analysis reported that an SPPB score < 10 is predictive of all-cause mortality [39], and a substantial proportion of patients scored below 10 even after CR (Table 2). In addition, gait speed was frequently below 1 m/s. Lower gait speed in the elderly is associated with an increased risk of hospitalization and cardiovascular mortality [40, 41], and a gait speed < 1.0 m/s was associated with lower survival and higher rehospitalization at 1 year post-treatment among patients with heart failure [42]. Furthermore, 6-minute walking distance was substantially below 300 m (Table 2), a performance level also reported to predict poor prognosis among patients with heart failure [43]. In-patient CR significantly improved physical function and ADL, but some patients still demonstrated worsening prognosis. Further changes to phase 2 CR content are required to improve these outcomes at discharge from rehabilitation hospital, especially in Japan, where phase 2 CR at rehabilitation hospitals has only recently been included in the medical service fees. Tsuchihashi et al [44] reported that poor social support is associated with rehospitalization of heart failure patients. Therefore, for further long-term improvement in HR-QoL, social support should be continued after discharge from the rehabilitation hospital.
Limitations
This study has several limitations. First, the number of patients that can be admitted for longer-term in-patient CR is very limited, so the sample size was correspondingly small. Second, the physiological exercise load was not uniform among the study group because exercise intensity was set using the Borg scale. Finally, other components of phase 2 CR were not examined by regression analysis, so the improved HR-QoL may not be solely the result of longer aerobic exercise duration.
Conclusions
We demonstrate that a longer daily aerobic exercise duration as part of in-patient CR is an independent predictor of better HR-QoL at 6 months post-discharge. This study provides support for the continued expansion of phase 2 CR in Japanese rehabilitation hospitals.
Acknowledgments
We would like to thank all staff members from the Nishi Memorial Port-island Rehabilitation Hospital.
Financial Disclosure
This study was funded by the Yuumi Memorial Foundation for Home Health Care.
Conflict of Interest
The authors declare that there is no conflict of interest.
Informed Consent
All patients provided written informed consent.
Author Contributions
TM (Tomohiro Matsuo): acquisition, analysis, and interpretation of data, writing and revising the manuscript, composition of tables and figures. TO, TY, and KU: acquisition of data. SK and TM (Takako Matsubara): revising the manuscript critically for important intellectual content. YM: conception and design of the study, analysis, interpretation of data, revising the manuscript critically. All authors approved the final version of the manuscript to be published.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
CR: cardiac rehabilitation; HR-QoL: health-related quality of life; EQ-5D-5L: EuroQol five-dimension five-level; ADLs: activities of daily living; BI: Barthel index; NYHA class: New York Heart Association functional classification; CCI: Charlson comorbidity index; LVEF: left ventricular ejection fraction; E/e’: early diastolic transmitral flow velocity to early diastolic mitral annular tissue velocity ratio; FIM: functional independence measure; SPPB: short physical performance battery; BW: body weight; 6MWT: 6-minute walk test; MMSE: mini-mental state examination; FITT-VP: frequency, intensity, time, type, volume, and progression/revision; MCID: minimal clinically important difference
| References | ▴Top |
- Izawa H, Yoshida T, Ikegame T, Izawa KP, Ito Y, Okamura H, Osada N, et al. Standard cardiac rehabilitation program for heart failure. Circ J. 2019;83(12):2394-2398.
doi pubmed - Yokota J, Takahashi R, Matsukawa Y, Matsushima K. Examination of independent predictors of discharge disposition in acute phase hospitalized heart failure patients undergoing phase I cardiac rehabilitation. Eur J Phys Rehabil Med. 2020;56(6):780-786.
doi pubmed - Kato N, Kinugawa K, Seki S, Shiga T, Hatano M, Yao A, Hirata Y, et al. Quality of life as an independent predictor for cardiac events and death in patients with heart failure. Circ J. 2011;75(7):1661-1669.
doi pubmed - Michalsen A, Grossman P, Lehmann N, Knoblauch NT, Paul A, Moebus S, Budde T, et al. Psychological and quality-of-life outcomes from a comprehensive stress reduction and lifestyle program in patients with coronary artery disease: results of a randomized trial. Psychother Psychosom. 2005;74(6):344-352.
doi pubmed - Makita S, Yasu T, Akashi YJ, Adachi H, Izawa H, Ishihara S, Iso Y, et al. JCS/JACR 2021 guideline on rehabilitation in patients with cardiovascular disease. Circ J. 2022;87(1):155-235.
doi pubmed - Morisawa T, Ueno K, Fukuda Y, Kanazawa N, Kawaguchi H, Zaiki R, Fuzisaki H, et al. Significance of sequential cardiac rehabilitation program through inter-hospital cooperation between acute care and rehabilitation hospitals in elderly patients after cardiac surgery in Japan. Heart Vessels. 2017;32(10):1220-1226.
doi pubmed - Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.
pubmed - Arai H, Satake S. English translation of the Kihon Checklist. Geriatr Gerontol Int. 2015;15(4):518-519.
doi pubmed - Granger CV, Hamilton BB, Linacre JM, Heinemann AW, Wright BD. Performance profiles of the functional independence measure. Am J Phys Med Rehabil. 1993;72(2):84-89.
doi pubmed - Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, Scherr PA, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85-94.
doi pubmed - ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111-117.
doi pubmed - Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198.
doi pubmed - van Hout B, Janssen MF, Feng YS, Kohlmann T, Busschbach J, Golicki D, Lloyd A, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708-715.
doi pubmed - Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337-343.
doi pubmed - Tsuchiya A, Ikeda S, Ikegami N, Nishimura S, Sakai I, Fukuda T, Hamashima C, et al. Estimating an EQ-5D population value set: the case of Japan. Health Econ. 2002;11(4):341-353.
doi pubmed - Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, Coke LA, et al. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013;128(8):873-934.
doi pubmed - Borg GA. Perceived exertion. Exerc Sport Sci Rev. 1974;2:131-153.
pubmed - Persinger R, Foster C, Gibson M, Fater DC, Porcari JP. Consistency of the talk test for exercise prescription. Med Sci Sports Exerc. 2004;36(9):1632-1636.
pubmed - Rich MW, Beckham V, Wittenberg C, Leven CL, Freedland KE, Carney RM. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. N Engl J Med. 1995;333(18):1190-1195.
doi pubmed - Mayer-Berger W, Simic D, Mahmoodzad J, Burtscher R, Kohlmeyer M, Schwitalla B, Redaelli M. Efficacy of a long-term secondary prevention programme following inpatient cardiovascular rehabilitation on risk and health-related quality of life in a low-education cohort: a randomized controlled study. Eur J Prev Cardiol. 2014;21(2):145-152.
doi pubmed - Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373-1379.
doi pubmed - Morimoto Y, Matsuo T, Yano Y, Fukushima T, Eishi K, Kozu R. Impact of sarcopenia on the progress of cardiac rehabilitation and discharge destination after cardiovascular surgery. J Phys Ther Sci. 2021;33(3):213-221.
doi pubmed pmc - Shiroiwa T, Noto S, Fukuda T. Japanese population norms of EQ-5D-5L and health utilities index mark 3: disutility catalog by disease and symptom in community settings. Value Health. 2021;24(8):1193-1202.
doi pubmed - Borregaard B, Pedersen SS, Berg SK, Dahl J, Ekholm O, Sibilitz K, Zwisler ADO, et al. What to expect after open heart valve surgery? Changes in health-related quality of life. Qual Life Res. 2020;29(5):1247-1258.
doi pubmed - Jones AM, Carter H. The effect of endurance training on parameters of aerobic fitness. Sports Med. 2000;29(6):373-386.
doi pubmed - O'Connor PJ, Puetz TW. Chronic physical activity and feelings of energy and fatigue. Med Sci Sports Exerc. 2005;37(2):299-305.
doi pubmed - Adamopoulos S, Coats AJ, Brunotte F, Arnolda L, Meyer T, Thompson CH, Dunn JF, et al. Physical training improves skeletal muscle metabolism in patients with chronic heart failure. J Am Coll Cardiol. 1993;21(5):1101-1106.
doi pubmed - Tikac G, Unal A, Altug F. Regular exercise improves the levels of self-efficacy, self-esteem and body awareness of young adults. J Sports Med Phys Fitness. 2022;62(1):157-161.
doi pubmed - Kaewthummanukul T, Brown KC. Determinants of employee participation in physical activity: critical review of the literature. AAOHN J. 2006;54(6):249-261.
doi pubmed - Mitchell T, Barlow CE. Review of the role of exercise in improving quality of life in healthy individuals and in those with chronic diseases. Curr Sports Med Rep. 2011;10(4):211-216.
doi pubmed - Toda G, Shibata S, Nakamizo R, Seto S, Yano K. Effect of physical exercise training on health-related quality of life and exercise tolerance in patients with left ventricular dysfunction. J Cardiol. 2004;44(5):179-187.
pubmed - Eder B, Hofmann P, von Duvillard SP, Brandt D, Schmid JP, Pokan R, Wonisch M. Early 4-week cardiac rehabilitation exercise training in elderly patients after heart surgery. J Cardiopulm Rehabil Prev. 2010;30(2):85-92.
doi pubmed - Ueshima K, Kamata J, Kobayashi N, Saito M, Sato S, Kawazoe K, Hiramori K. Effects of exercise training after open heart surgery on quality of life and exercise tolerance in patients with mitral regurgitation or aortic regurgitation. Jpn Heart J. 2004;45(5):789-797.
doi pubmed - Netuveli G, Wiggins RD, Hildon Z, Montgomery SM, Blane D. Functional limitation in long standing illness and quality of life: evidence from a national survey. BMJ. 2005;331(7529):1382-1383.
doi pubmed pmc - Soubra R, Chkeir A, Novella JL. A systematic review of thirty-one assessment tests to evaluate mobility in older adults. Biomed Res Int. 2019;2019:1354362.
doi pubmed pmc - Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc. 2006;54(5):743-749.
doi pubmed - Rinaldo L, Caligari M, Acquati C, Nicolazzi S, Paracchini G, Sardano D, Giordano A, et al. Functional capacity assessment and Minimal Clinically Important Difference in post-acute cardiac patients: the role of Short Physical Performance Battery. Eur J Prev Cardiol. 2022;29(7):1008-1014.
doi pubmed - Singh SJ, Puhan MA, Andrianopoulos V, Hernandes NA, Mitchell KE, Hill CJ, Lee AL, et al. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1447-1478.
doi pubmed - Pavasini R, Guralnik J, Brown JC, di Bari M, Cesari M, Landi F, Vaes B, et al. Short Physical Performance Battery and all-cause mortality: systematic review and meta-analysis. BMC Med. 2016;14(1):215.
doi pubmed pmc - Cesari M, Kritchevsky SB, Penninx BW, Nicklas BJ, Simonsick EM, Newman AB, Tylavsky FA, et al. Prognostic value of usual gait speed in well-functioning older people—results from the Health, Aging and Body Composition Study. J Am Geriatr Soc. 2005;53(10):1675-1680.
doi pubmed - Dumurgier J, Elbaz A, Ducimetiere P, Tavernier B, Alperovitch A, Tzourio C. Slow walking speed and cardiovascular death in well functioning older adults: prospective cohort study. BMJ. 2009;339:b4460.
doi pubmed pmc - Pulignano G, Del Sindaco D, Di Lenarda A, Alunni G, Senni M, Tarantini L, Cioffi G, et al. Incremental value of gait speed in predicting prognosis of older adults with heart failure: insights from the IMAGE-HF study. JACC Heart Fail. 2016;4(4):289-298.
doi pubmed - Rostagno C, Olivo G, Comeglio M, Boddi V, Banchelli M, Galanti G, Gensini GF. Prognostic value of 6-minute walk corridor test in patients with mild to moderate heart failure: comparison with other methods of functional evaluation. Eur J Heart Fail. 2003;5(3):247-252.
doi pubmed - Tsuchihashi-Makaya M, Kato N, Chishaki A, Takeshita A, Tsutsui H. Anxiety and poor social support are independently associated with adverse outcomes in patients with mild heart failure. Circ J. 2009;73(2):280-287.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.