

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 14, Number 4, August 2023, pages 261-267

Safety and Feasibility of Tele-Cardiac Rehabilitation Using Remote Biological Signal Monitoring System: A Pilot Study
Miho Nishitani-Yokoyamaa, b, f, Kazunori Shimadaa, Kei Fujiwaraa, Abidan Abulimitia, Hiroki Kasuyaa, Mitsuhiro Kunimotoa, Yurina Yamaguchia, Minoru Tabatac, Masakazu Saitohd, Tetsuya Takahashid, Hiroyuki Daidaa, d, Shuko Nojirie, Tohru Minaminoa
aDepartment of Cardiovascular Biology and Medicine, Juntendo University Graduate School of Medicine, Tokyo, Japan
bCardiovascular Rehabilitation and Fitness, Juntendo University Hospital, Tokyo, Japan
cDepartment of Cardiovascular Surgery, Juntendo University Graduate School of Juntendo Medicine, Tokyo, Japan
dFaculty of Health Science, Juntendo University, Tokyo, Japan
eMedical Technology Innovation Center, Juntendo University, Tokyo, Japan
fCorresponding Author: Miho Nishitani-Yokoyama, Department of Cardiovascular Biology and Medicine, Juntendo University Graduate School of Medicine, Bunkyo-ku, Tokyo 113-8421, Japan
Manuscript submitted June 17, 2023, accepted July 27, 2023, published online August 4, 2023
Short title: Pilot Study on Tele-Cardiac Rehabilitation
doi: https://doi.org/10.14740/cr1530
| Abstract | ▴Top |
Background: Cardiac rehabilitation (CR) is categorized as a class I recommendation in the guidelines for the management of patients with cardiovascular disease (CVD). However, the penetration rate of outpatient CR is low in Japan. We designed a pilot study to evaluate the safety and feasibility of tele-CR using a remote biological signal monitoring system.
Methods: A total of nine patients (median aged 70.0 (66.0 - 76.0) years (male = 6) with CVD who participated in phase II CR for 1 month under the exercise prescription using the cardiopulmonary exercise test (CPET) were analyzed. They participated in the tele-CR program with a remote biological signal monitoring system (Nipro HeartLineTM, Osaka, Japan, and Duranta, Miyagi, Japan) in the CR room and were instructed by the CR staff from a separate room in the hospital. We evaluated the occurrence and degree of remote biological signal monitoring defects as safety evaluation items, i.e., whether the patients could set the remote biological signal monitoring equipment, as a feasibility evaluation item during a 3-month period. We also performed CPET at the baseline and follow-up. Following the 3-month tele-CR program, a total of 122 remote CR programs were performed using the remote biological signal monitoring system.
Results: No patient experienced a lack of remote biological signal monitoring during exercise therapy. Significant improvement was noted in the exercise capacity, as assessed using the cardiopulmonary test (from 19.5 (16.7 - 20.2) mL/kg/min to 21.1 (17.3 - 22.8) mL/kg/min, P = 0.01, age ratio from 86% (75-96%) to 99% (78-104%), P = 0.01). One patient required support using the remote biological signal monitoring system, including information technology literacy.
Conclusions: This study suggests the safety and feasibility of tele-CR using the remote biological signal monitoring system. However, further investigations are required to explore the suitability, effects, and cost-effectiveness of tele-CR as an alternative to center-based CR in the future.
Keywords: Tele-cardiac rehabilitation; Remote biological signal monitoring system; Exercise capacity; Industry-academia collaboration
| Introduction | ▴Top |
Comprehensive cardiac rehabilitation (CR), including exercise training, has been proven to improve exercise capacity and quality of life (QoL) and reduce cardiovascular and total mortality in patients with cardiovascular disease (CVD) [1, 2]. The guidelines of the American College of Cardiology, American Heart Association, and Japanese Circulation Society (JCS) have recommended the use of CR in patients with CVD as a class I intervention [2, 3]. In Japan, CR can be provided for 150 days under medical insurance, and most of this period corresponds to phase II (recovery period). Phase II CR is generally provided as a collective CR at a CR facility after discharge, with several patients visiting the hospital at a fixed time [2]. However, in Japan, the implementation of CR remains low even in JCS training hospitals. A recent study has reported that 3.8-7.6% of the patients participate in CR in Japan [4, 5]. Outpatient CR has problems on the medical side, such as the limited number of medical facilities that can provide it, and problems on the patient side, such as the difficulty of patients attending a hospital in a group setting at a given time [4, 5]. In recent years, the spread of coronavirus disease 2019 (COVID-19) has exacerbated the problem of low adoption and implementation rates of outpatient CR [6-8]. To solve the problems related to outpatient CR, home-based CR initiatives in which voluntary exercise is performed under the guidance of a medical practitioner have been implemented. It has been reported as a potential complementary therapy [9]. However, whether the exercise therapy is sufficient is likely to vary from patient to patient, and there are issues in terms of efficacy and safety [10]. Tele-CR can be defined as a remote CR program that uses biological signal monitoring system to support it [11]. A report has observed that it is possible to perform remote CR with the same level of safety as under the supervision of a specialist using internet of things (IoT) to monitor necessary biosignals and e-learning methods for patients at home [12]. In exercise therapy, which is an element of comprehensive CR, the most important point is how to provide efficacy while maintaining safety. In this study, we performed remote CR using real-time biosignal monitoring and examined its safety and feasibility.
| Materials and Methods | ▴Top |
Study design and subjects
This study is a single-center prospective pilot study. The subjects were 12 patients with CVD who attended the Juntendo University Hospital Heart Center from March 2020 to March 2021 and participated in phase II CR. They participated in the tele-CR study after confirming that they were able to perform phase II CR stably for 1 month under exercise prescription by the cardiopulmonary exercise test (CPET). Individuals satisfying the following criteria were excluded: 1) patients weighing over 130 kg; 2) patients with poorly controlled complications; 3) patients satisfying the contraindication/withdrawal criteria for CR; 4) patients with unstable cardiovascular condition; 5) patients who experienced a cardiovascular event within 1 month after starting phase II CR; 6) patients who had difficulty performing aerobic exercise using a bicycle ergometer owing to the effects of cerebral infarction and/or orthopedic disease; 7) patients under treatment for malignant neoplasms; 8) other individuals whose participation was deemed inappropriate by the principal investigator; and 9) pregnant or breastfeeding women. After the principal and subinvestigators obtained the patients’ consent, their eligibility was verified by the Juntendo Clinical Research and Trial Center. We assessed whether each patient experienced a lack of remote biological signal monitoring (no communication of blood pressure, oxygen saturation, and electrocardiogram (ECG) waveforms) during exercise therapy and whether such problems forced the patient to discontinue exercise. Exercise tolerance (peak oxygen intake; peak VO2) at 3 months after implementing the tele-CR was set as the secondary evaluation item. Exercise tolerance was evaluated using symptom-limited CPET (AE-310S, Minato Medical Science Co. Ltd., Osaka). Moreover, we secondarily investigated whether the patient was able to independently set up the exercise device for remote CR and ensure its safety. For every session, the following 11 items (Table 1) were checked by compiling their presence/absence, frequency, and whether intervention by a medical professional was required.
 Click to view | Table 1. Eleven Items Checked |
Informed consent was obtained from all participants according to the mandates of the Ethics Committee of Juntendo University Hospital (CRB3180012). This study was conducted in accordance with the ethical principles in the Declaration of Helsinki. This study was registered in the Japan Registry of Clinical Trials (jRCT) system under trial ID jRCTs032190217.
Tele-CR program and tele-monitoring system
The subjects participated in the exercise therapy using the remote biological signal monitoring system in the CR room at Juntendo University Hospital during the implementation period of phase II CR. Medical professionals monitored and instructed the subjects during the exercise therapy in a separate room within the hospital premises (Fig. 1). For 1 month before starting the program, the CR staff members supported the subjects in becoming accustomed to connecting and using the monitoring device. The primary system used for the remote CR was a support system for remote diagnosis (NIPRO Heartline™, NIPRO). This system can be connected to various biological signal measurement devices (manometers, pulse oximeters, wearable ECG monitors, etc.) via Bluetooth, and the measured results can be captured automatically and sent to the operator in real-time. A wearable ECG monitor (Duranta) was used to monitor two-channel ECG waveforms. While the patients’ facial expressions were observed using a videophone via the campus local area network, their biological signals, including ECG waveforms, were monitored in real-time. Two devices were used for biological monitoring in this study: one biological monitoring device and one videophone device, which were connected to each other via Bluetooth. As per the CR guidelines issued by the JCS [3], each session comprised 20 - 40 min of aerobic exercise (front-and-back stretching, recumbent exercise bicycling, and walking) and additional self-weight resistance training, lasting for a total of 60 - 80 min. While conversing with the patient via video call, the operator instructed them on disease management, including information on various symptoms and nutritional guidance.
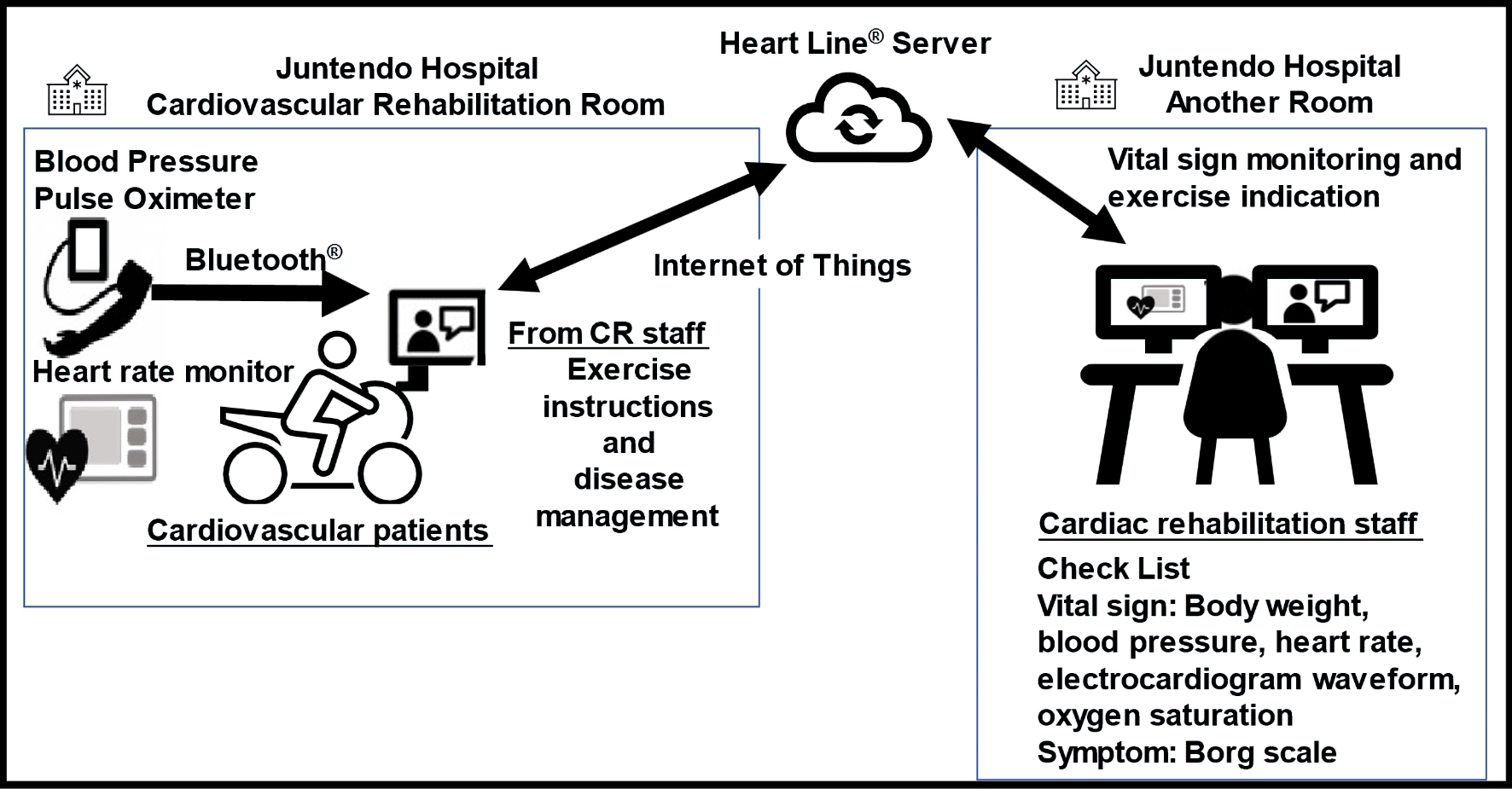 Click for large image | Figure 1. Schema of tele-CR. CR: cardiac rehabilitation. |
When overexercise or heart failure were suspected during an exercise session, either the session was terminated, or the regimen was reduced. To identify overexercise or heart failure, the following standards were used as per the CR guidelines issued by the JCS [3]: 1) subjective symptoms (persistent weariness, fatigue remaining from the previous day, and an increase of ≥ 2 on the Borg scale under the same loading conditions); 2) weight increasing tendency (≥ 2 kg increase in 1 week); 3) heart rate increasing tendency (≥ 10 beats per minute increase at rest or under the same loading conditions); and 4) blood B-type natriuretic peptide increasing tendency (≥ 100 pg/mL increase from before). For item 4), blood samples were collected and tested during regular outpatient checkups.
Blood biochemistry test
Blood biochemical tests were conducted for serum hemoglobin (Hb), low-density lipoprotein cholesterol, triglycerides, high-density protein cholesterol, hemoglobin A1c (HbA1c), and N-terminal pro-brain natriuretic peptide (NT-proBNP) at the beginning of CR.
Statistical analysis
The results were statistically expressed as means ± standard deviations following analysis using SAS (SAS Institute Inc., Cary, NC, USA). According to their distributions, the clinical characteristics of the groups were compared using paired Wilcoxon signed-rank test. Data at baseline and follow-up CR were compared for each patient using paired Wilcoxon signed-rank tests to evaluate the singular effects of CR. A P value of < 0.05 was considered statistically significant.
| Results | ▴Top |
Patient characteristics
As the study period coincided with the peak of the COVID-19 pandemic, three of the patients were unable to complete the phase II CR program. Nine (of whom six were men) completed the remote CR program that comprised a total of 122 exercise sessions. Table 2 shows the clinical characteristics of the patients. Overall, three of them had undergone open-heart surgery (two, mitral valve plasty; one, coronary arterial bypass), three had angina pectoris, and three had peripheral arterial disease. Of the nine patients, eight patients had hypertension, six patients had dyslipidemia, four patients had diabetes, and two patients were on maintenance dialysis. At the beginning of the program, exercise tolerance was 19.5 (16.7 - 20.2) mL/kg/min, which was 86% relative to the age and favorable. Furthermore, anaerobic threshold was 13.0 (11.2 - 13.4) mL/kg/min, which was 86% (78-90)% relative to the age. Although a 1-month support period by medical professionals was set aside for educating the subjects on how to set up and use the monitoring equipment, one patient had difficulty in independently using the devices and the monitoring system during remote CR and required 10 interventions. This individual failed to check “whether the device is connected to the remote biological monitoring system” and “whether the operation of the remote monitoring system can be checked during the rehabilitation session”, both of which were items related to remote monitoring. Regarding the safety of remote CR (which was the primary evaluation item), the positive frequency of problems during remote biological signal monitoring (problems in ECG waveforms) was 0 time (0%). While problems such as having to reboot the system because of communication errors in applications occurred two times (1.6%), no problems in biological signals, including ECG monitoring, were noted; thus, continued exercise was feasible. Moreover, no adverse events were noted during the remote CR program.
Click to view | Table 2. Patient Characteristics |
Figure 2 shows the change of exercise tolerance, which was the secondary evaluation item. The peak oxygen intake (from 19.5 (16.7 - 20.2) mL/kg/min to 21.1 (17.3 - 22.8) mL/kg/min, P = 0.01) and the anaerobic threshold (from 13.0 (11.2 - 13.4) mL/kg/min to 15.1 (13.3 - 15.8) mL/kg/min, P < 0.01) improved significantly 3 months later.
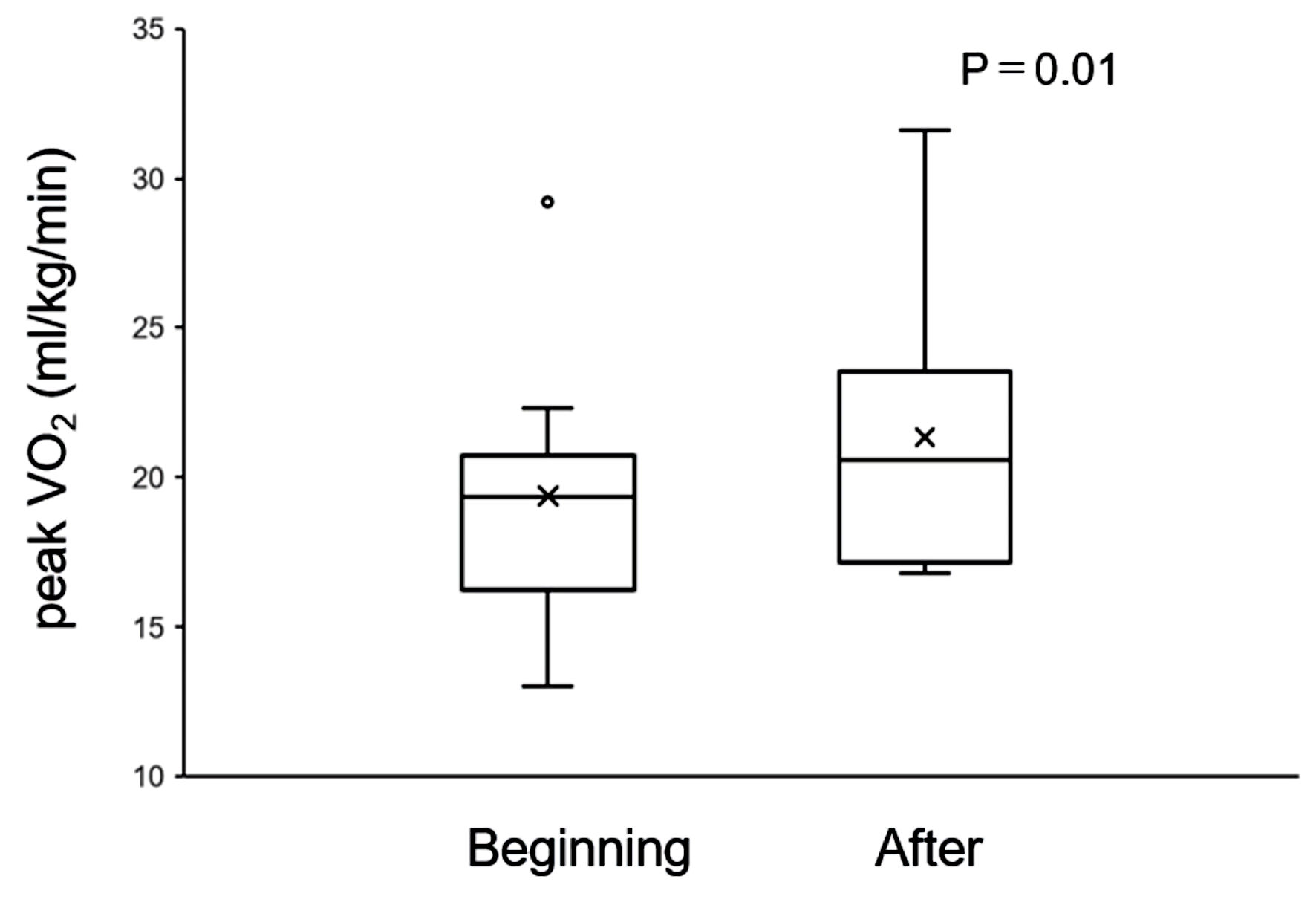 Click for large image | Figure 2. Comparison of exercise tolerance before and after tele-CR. CR: cardiac rehabilitation. |
| Discussion | ▴Top |
We conducted a pilot study on CR using a remote biological signal monitoring system during phase II CR. Neither monitoring-related problems nor cardiac accidents were noted in the course of the remote CR program comprising a total of 122 remote biological monitoring exercise sessions. CR using digital tools is mainly provided in three methods [13]: 1) In virtual CR, the patient and medical staff are in different locations, and exercise therapy is performed while being monitored in real time using audiovisual communication; 2) In synchronous CR, the patient and medical staff are face-to-face, and CR is performed through the use of digital technology; 3) In remote CR, patients exercise independently, and the data are transmitted and reviewed by medical staff using digital technology.
Currently, tele-CR is not covered by insurance, and this study is one of the few studies of tele-CR using real-time, face-to-face monitoring in patients participating phase II CR. This study is of importance as it has proposed a method that may complement presently practiced CR systems. There are two types of data exchange for biological signal monitoring: One is a face-to-face real-time exchange method using video chats. The other is a semi-synchronous method in which the patient data are uploaded to an online application, and medical professionals access these data as appropriate [14, 15]. In the present study, we were able to remotely acquire ECG waveforms, heart rates, circulatory parameters of blood pressure, and exercise intensity parameters while the patients were engaged in exercise. Also, the patients’ physical appearances were observed via a video screen. Based on this information, we were able to determine the appropriateness of the exercise regimen, such as whether the current workload was placing too much pressure on the patients. We believe that this in turn guaranteed safety in the implementation of the program. The CPET conducted 3 months later confirmed improvements in exercise tolerance. Implementing exercise therapy based on a proper exercise regimen under the supervision of medical professionals apparently contributed to these improvements.
While collecting more patient-related information guarantees increased safety, it also complicates certain procedures, such as setting up and troubleshooting the equipment, thereby limiting applicable patients. Moreover, it necessitates securing medical human resources for properly managing voluminous information. In the present study, while all subjects were able to independently perform the exercise, one found it difficult to use the remote monitoring equipment and required support from the medical staff for continuing and completing the program. Two devices were used for biological monitoring in this study: one biological monitoring device and one videophone device, which were connected to each other via Bluetooth. While some patients may be able to overcome the difficulties if remote devices are more streamlined or simply via practice, using a complex IoT system may prove to be immensely stressful because troubleshooting and other support may not necessarily be available. A previous study has suggested that a subject’s adeptness at information technology (information technology (IT) literacy) may be an important eligibility criterion [16]. Given the rapid aging of the population in Japan, the IT literacy of elderly patients is an important challenge. In the present study, the patient who required the assistance of the staff in using the equipment was 72 years old. However, a report has indicated that despite Japan having one of the world’s oldest populations, Japanese individuals aged 16 - 65 years displayed digital literacy and calculation ability that were among the best globally [17]. Therefore, as the population ages further, remote rehabilitation may become more widespread as an option for home-based medical care. To facilitate home care for patients, it is essential to reinforce social environments, such as improving Wi-Fi availability.
Being a comprehensive secondary prophylaxis program, CR includes not only exercise therapy but also alimentary therapy, correction/management of coronary risk factors, guidance for quitting smoking, psychological evaluation, guidance for returning to work, and psychological support [2]. In group-based CR, having many fellow participants has benefits similar to those in group therapy and is conducive to improving psychological support and QoL [18]. In terms of cost effectiveness and interaction among patients, the development of platforms where several patients are simultaneously connected is anticipated. Many more improvements will be required to achieve safety and the efficient management of patient information. This study involved patients with high exercise tolerance, namely a low-risk group for performing exercise. Consequently, no adverse events were noted, a frailty index was maintained (Short-Physical Performance Battery score from 12 to12), and exercise tolerance improved. Patient education using remote CR and mobile devices is considered a “good opinion” for patients with low- to moderate-risk CVD [9]. Recently, programs intended for high-risk patients, such as frail elderly individuals, have been assessed [19].
There are several limitations in this study. This research was a small-scale study involving participants in phase II CR at a single institution and was conducted to evaluate the safety and feasibility of tele-CR in this case series. Given the small sample size, no definitive conclusions could be reached. To demonstrate the advantages of tele-CR in improving exercise tolerance, prognosis and its safety for patients with low exercise tolerance, long-term interventions involving larger samples need to be implemented. The results of our tele-CR program indicate the feasibility of this system. It should be noted, however, that the outcome may be dependent on the patient’s digital literacy, internet environment, and available applications. In Japan, the Health, Labor, and Welfare Ministry has proposed 10 basic plans for patients with CVD and for improving the medical services [20]. In the future, it is necessary to develop remote medical systems that are simple and easy to use for anyone anywhere.
Conclusions
Tele-CR for phase II CR may be applicable as an intervention option for patients with CVD. We believe that it is essential to understand the advantages of and challenges in tele-CR and to further investigate the usefulness of tele-CR in terms of QoL, prognosis, and cost effectiveness while promoting industry-university and medical-engineering collaboration.
Acknowledgments
We greatly acknowledge the contributions of the members of Cardiovascular Rehabilitation and Fitness, Juntendo University Hospital, for tele-CR management. Akio Honzawa has assisted and supported in sample collection. The authors would like to thank Haruki Itoh, Yuji Nishizaki and the members of Medical Technology Innovation Center, Juntendo University, for their assistance with this work. The authors would also like to thank Yuji Kobayashi for the support in setting up and troubleshooting the remote CR system.
Financial Disclosure
This research was performed with the research grant of Japan Heart Club (npo-jhc.org).
Conflict of Interest
The authors declare that there are no conflicts of interest.
Informed Consent
Informed consent was obtained from all participants according to the mandates of the ethics committee of Juntendo University Hospital (CRB3180012).
Author Contributions
MNY, KS, MS, and HD conceived the study and obtained grant funding. MNY, AA, KF, and MT contributed to the conception and design of the work. TT, HK, MK, and YY contributed to the literature search. MNY, AA, and SN contributed to the data analysis for the work. MNY, KS, SN, and HD contributed to the drafting of the manuscript. KS, TT, and TM critically revised the manuscript.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon request.
Abbreviations
CR: cardiac rehabilitation; CVD: cardiovascular disease; CPET: cardiopulmonary exercise test; ECG: electrocardiogram; IoT: internet of things; JCS: Japanese Circulation Society; tele-CR: tele-cardiac rehabilitation; QoL: quality of life
| References | ▴Top |
- Braverman DL. Cardiac rehabilitation: a contemporary review. Am J Phys Med Rehabil. 2011;90(7):599-611.
doi pubmed - Makita S, Yasu T, Akashi YJ, Adachi H, Izawa H, Ishihara S, Iso Y, et al. JCS/JACR 2021 guideline on rehabilitation in patients with cardiovascular disease. Circ J. 2022;87(1):155-235.
doi pubmed - Smith SC, Jr., Allen J, Blair SN, Bonow RO, Brass LM, Fonarow GC, Grundy SM, et al. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update: endorsed by the National Heart, Lung, and Blood Institute. Circulation. 2006;113(19):2363-2372.
doi pubmed - Goto Y, Saito M, Iwasaka T, Daida H, Kohzuki M, Ueshima K, Makita S, et al. Poor implementation of cardiac rehabilitation despite broad dissemination of coronary interventions for acute myocardial infarction in Japan: a nationwide survey. Circ J. 2007;71(2):173-179.
doi pubmed - Kamiya K, Yamamoto T, Tsuchihashi-Makaya M, Ikegame T, Takahashi T, Sato Y, Kotooka N, et al. Nationwide survey of multidisciplinary care and cardiac rehabilitation for patients with heart failure in Japan - An Analysis of the AMED-CHF Study. Circ J. 2019;83(7):1546-1552.
doi pubmed - Kida K, Nishitani-Yokoyama M, Oishi S, Kono Y, Kamiya K, Kishi T, Node K, et al. Nationwide survey of Japanese Cardiac Rehabilitation Training Facilities during the coronavirus disease 2019 outbreak. Circ Rep. 2021;3(6):311-315.
doi pubmed pmc - Kida K, Nishitani-Yokoyama M, Kono Y, Kamiya K, Kishi T, Node K, Makita S, et al. Second Nationwide Survey of Japanese Cardiac Rehabilitation Training Facilities during the coronavirus disease 2019 (COVID-19) outbreak. Circ Rep. 2022;4(10):469-473.
doi pubmed pmc - Kirwan R, Perez de Heredia F, McCullough D, Butler T, Davies IG. Impact of COVID-19 lockdown restrictions on cardiac rehabilitation participation and behaviours in the United Kingdom. BMC Sports Sci Med Rehabil. 2022;14(1):67.
doi pubmed pmc - Thomas RJ, Beatty AL, Beckie TM, Brewer LC, Brown TM, Forman DE, Franklin BA, et al. Home-based cardiac rehabilitation: a scientific statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation. 2019;140(1):e69-e89.
doi pubmed - O'Connor CM, Whellan DJ, Lee KL, Keteyian SJ, Cooper LS, Ellis SJ, Leifer ES, et al. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA. 2009;301(14):1439-1450.
doi pubmed pmc - Kaihara T, Scherrenberg M, Falter M, Frederix I, Itoh H, Makita S, Akashi YJ, et al. Cardiac Telerehabilitation - A Solution for Cardiovascular Care in Japan. Circ Rep. 2021;3(12):733-736.
doi pubmed pmc - Frederix I, Vanhees L, Dendale P, Goetschalckx K. A review of telerehabilitation for cardiac patients. J Telemed Telecare. 2015;21(1):45-53.
doi pubmed - Golbus JR, Lopez-Jimenez F, Barac A, Cornwell WK, 3rd, Dunn P, Forman DE, Martin SS, et al. Digital technologies in cardiac rehabilitation: a science advisory from the American Heart Association. Circulation. 2023;148(1):95-107.
doi pubmed - Maddison R, Rawstorn JC, Stewart RAH, Benatar J, Whittaker R, Rolleston A, Jiang Y, et al. Effects and costs of real-time cardiac telerehabilitation: randomised controlled non-inferiority trial. Heart. 2019;105(2):122-129.
doi pubmed pmc - Kraal JJ, Peek N, Van den Akker-Van Marle ME, Kemps HM. Effects of home-based training with telemonitoring guidance in low to moderate risk patients entering cardiac rehabilitation: short-term results of the FIT@Home study. Eur J Prev Cardiol. 2014;21(2 Suppl):26-31.
doi pubmed - Liu S, Zhao H, Fu J, Kong D, Zhong Z, Hong Y, Tan J, et al. Current status and influencing factors of digital health literacy among community-dwelling older adults in Southwest China: a cross-sectional study. BMC Public Health. 2022;22(1):996.
doi pubmed pmc - Organisation for Economic Co-operation and Development (OECD). OECD skills outlook 2019. Learning for life. Country profile: Japan. https://www.oecd.org/japan/Skills-Outlook-JapanEN.pdf (accessed May 7, 2023).
- Pogosova N, Saner H, Pedersen SS, Cupples ME, McGee H, Hofer S, Doyle F, et al. Psychosocial aspects in cardiac rehabilitation: From theory to practice. A position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation of the European Society of Cardiology. Eur J Prev Cardiol. 2015;22(10):1290-1306.
doi pubmed - Saitoh M, Takahashi T, Morisawa T, Honzawa A, Yokoyama M, Abulimiti A, Kagiyama N, et al. Remote cardiac rehabilitation in older cardiac disease: a randomized case series feasibility study. Cardiol Res. 2022;13(1):57-64.
doi pubmed pmc - Kuwabara M, Mori M, Komoto S. Japanese national plan for promotion of measures against cerebrovascular and cardiovascular disease. Circulation. 2021;143(20):1929-1931.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.