

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 14, Number 5, October 2023, pages 416-420

Unveiling the Influence of Smoking and Uncontrolled Lipid Profile in the Development of ST-Elevation Myocardial Infarction
Meutia Putri Aristyaa, c, Nada Putri Pranidyab, Mery Natalia Hutapeab, Afdhalun Anwar Hakimb
aFaculty of Medicine, Universitas Airlangga, Surabaya, East Java 60132, Indonesia
bDepartment of Cardiology, Badan Pengusahaan Hospital, Batam, Riau Islands 29428, Indonesia
cCorresponding Author: Meutia P. Aristya, Faculty of Medicine, Universitas Airlangga, Surabaya, East Java 60132, Indonesia
Manuscript submitted September 3, 2023, accepted October 7, 2023, published online October 25, 2023
Short title: Influence of Smoking and Lipid Profile in STEMI
doi: https://doi.org/10.14740/cr1564
| Abstract | ▴Top |
We report a case of a 25-year-old male with the traditional risk factor for coronary artery disease (CAD), such as frequent smoking, while the other risk factors such as familial history of CAD were denied and hypertension, obesity, diabetes mellitus, or coagulation factors were not found. Patient was admitted with anterior ST-elevation myocardial infarction. Coronary angiography showed high intracoronary thrombus burden and total occlusion of the proximal segment of left anterior descending artery. Percutaneous coronary intervention was then performed as the treatment of choice, and resulted with no residual stenosis after. The patient had a smooth and progressive recovery.
Keywords: Young age STEMI; ST-elevation myocardial infarction; Smoking
| Introduction | ▴Top |
Coronary artery disease (CAD) is still one of the main causes of death worldwide, including in Indonesia. It used to commonly occur in the older population, specifically those aged over 40 years [1]. However, recent trends demonstrate an increasing incidence in younger populations due to changes in lifestyle and unhealthy eating habits. Moreover, this rise in numbers is further exacerbated by various main risk factors such as smoking, obesity, diabetes mellitus and family history [2]. Consequently, there are more and more studies discussing and updating the management and prevention of acute myocardial infarction (AMI), especially in young populations.
The occurrence of AMI, which has shifted to a younger population, will certainly have more severe long-term effects because it may lead to more adverse outcomes. This correlation is often associated with increased morbidity rates, psychological impacts, and so on [2, 3]. Therefore, the purpose of writing this case report is to address a pressing health issue that demands our attention due to its increasing occurrence among young populations. In this report, we discuss a case of a 25-year-old man with no previous medical history who presented with ST-elevation myocardial infarction (STEMI). Understanding such cases is crucial to ensure prompt and accurate management and prevention of similar complaints in patients.
| Case Report | ▴Top |
A 25-year-old male with no prior medical history presented to the emergency department complaining of sudden retrosternal pain for the past 72 h with no improvement with rest. The patient was immediately transferred to the hospital. On presentation, his blood pressure was 106/66 mm Hg, heart rate was 114 bpm, oxygen saturation was 98% on room air, and his temperature was normal. Physical examination findings were within normal limits.
The patient presented with a risk factor of CAD, which is frequent daily tobacco use for the past 2 years, smoking around 2 packs per day. The patient’s body mass index (BMI) was 27.5, categorizing him as overweight. However, other additional supporting risk factors such as hypertension, diabetes mellitus, a familial history of premature CAD, or any coagulation disorder were absent. The usage of any substances or recreational drugs was also denied.
Multiple tests were performed during the examination in the emergency room, including an electrocardiogram, laboratory tests, a chest X-ray, and an echocardiogram. A 12-lead electrocardiogram revealed an anterior STEMI, which showed ST-segment elevation in leads V2-V4 (Fig. 1). The laboratory test indicated peak troponin I levels of 40,000 ng/L. The chest X-ray examination showed slight cardiomegaly with a cardiothoracic ratio (CTR) of 52%. A bedside echocardiogram was immediately performed, revealing hypokinesis of the anteroapical wall with moderately reduced left ventricular systolic function, estimated at 42%, and no valvular abnormalities, thrombi, or pericardial effusion were found. The patient was immediately transferred to the catheterization laboratory for immediate primary percutaneous coronary intervention (pPCI).
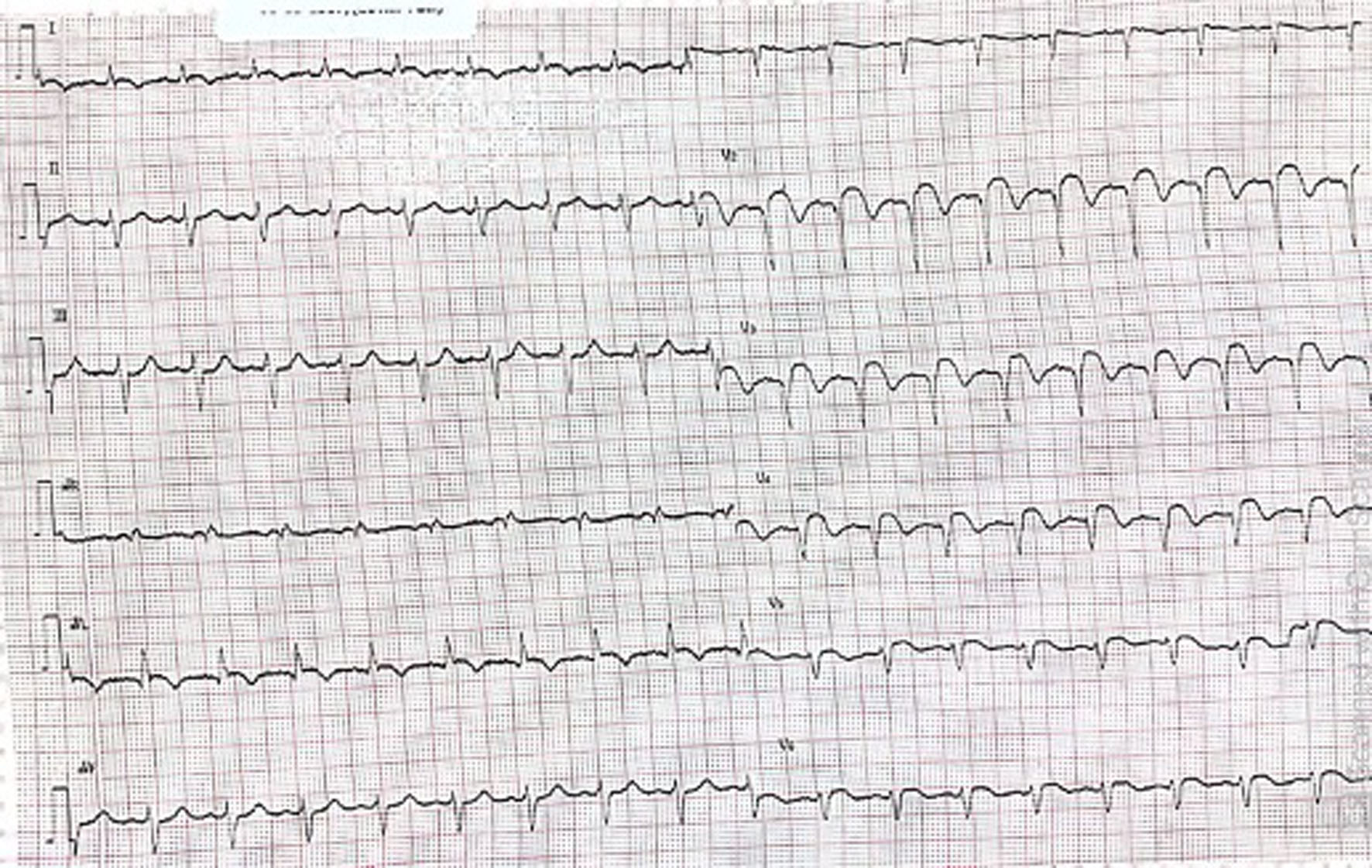 Click for large image | Figure 1. Electrocardiogram showing ST-elevation in anterior leads (V2, V3, V4). |
Coronary angiography showed a contrast-filling defect suggestive of thrombus formation and total occlusion of the proximal segment of the left anterior descending artery (LAD) (Fig. 2). The right coronary artery and the left circumflex artery were normal. A drug-eluting stent was implanted in the occluded site of the LAD, resulting in 0% stenosis from an initial 100% stenotic lesion in myocardial infarction TIMI flow 3 (Fig. 3).
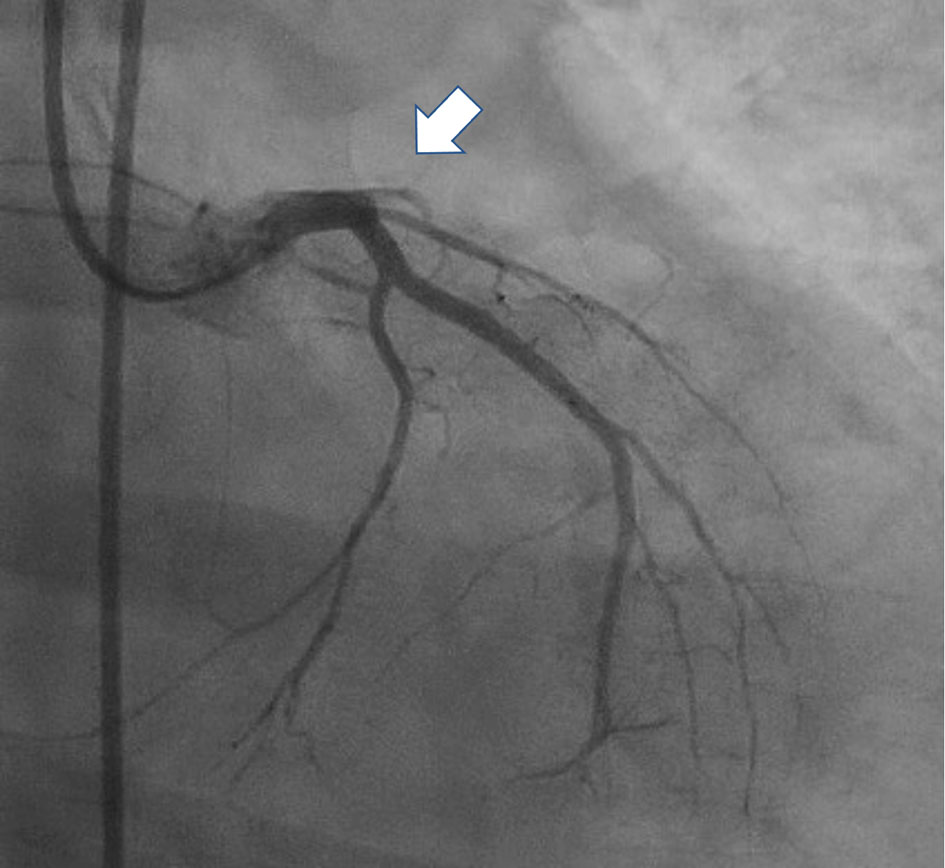 Click for large image | Figure 2. Coronary angiogram revealing 100% occlusion (arrow) of the osteal - proximal left anterior descending coronary artery. |
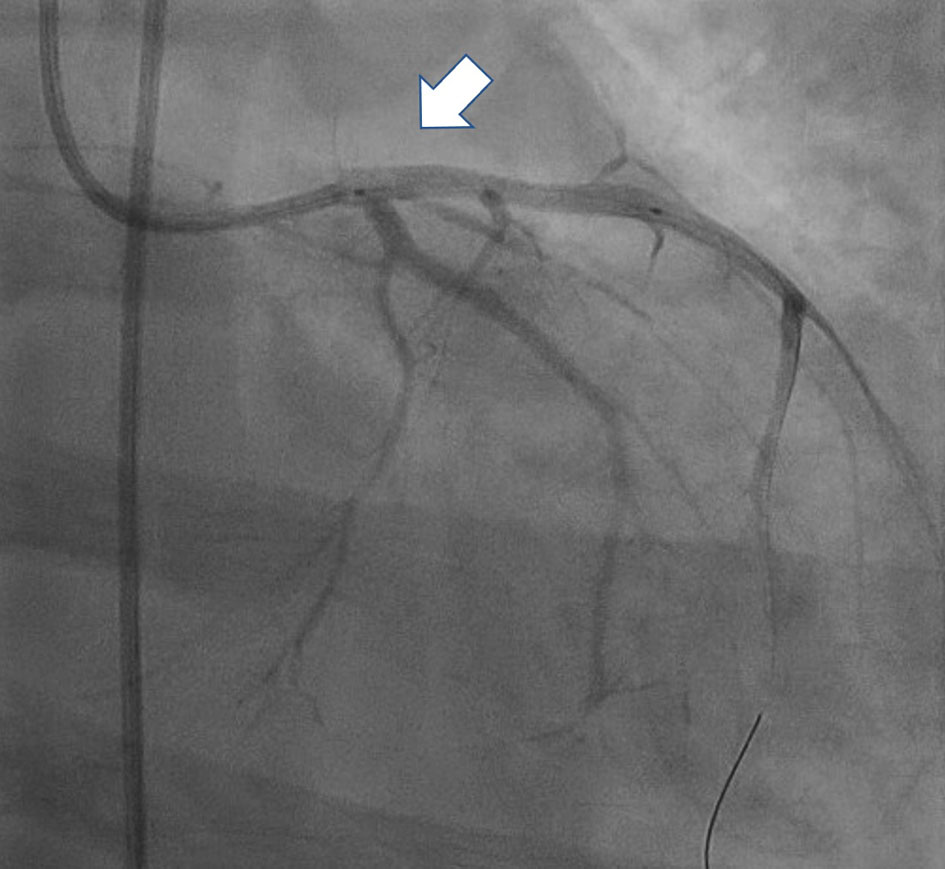 Click for large image | Figure 3. Post-intervention angiogram with normal flow (arrow) in the left anterior descending coronary artery. |
The patient was transferred to the intensive care unit. Laboratory tests demonstrated total cholesterol of 168 mg/dL, low-density lipoprotein cholesterol (LDL-C) of 107 mg/dL, high-density lipoprotein cholesterol of 44 mg/dL, triglycerides of 189 mg/dL, D-dimers of 347 ng/mL, partial thromboplastin time (PTT) of 13.6 s, activated partial thromboplastin time (aPTT) of 31.1 s, and C-reactive protein of 7 mg/L. Immunology tests for antiphospholipid antibodies and the lupus anticoagulant were also conducted and showed negative results, while levels of protein C, protein S, and antithrombin III were within normal limits. The nasopharyngeal swab for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), using reverse-transcription polymerase chain reaction (RT-PCR) assay, was negative. Toxicology tests for blood and urine were also conducted to obtain the proof of drug use such as cocaine or amphetamine, and it resulted negative. Apart from dual antiplatelet therapy with aspirin and clopidogrel, our patient continued to receive oral medications such as candesartan 4 mg once daily, bisoprolol 2.5 mg once daily, isosorbide dinitrate 5 mg twice daily, and atorvastatin 40 mg once daily.
An echocardiogram was performed 24 h following PCI and revealed an ejection fraction of 48% with residual wall motion abnormalities accompanying the anterior wall myocardial infarction. These findings indicated an improvement in ejection fraction compared to the initial result. The patient had a smooth recovery and was discharged symptom-free after 5 days on aspirin 80 mg daily, clopidogrel 75 mg daily, bisoprolol 2.5 mg daily, candesartan 4 mg daily, and atorvastatin 40 mg daily. The patient was given recommendations on weight reduction, a healthy diet, routine exercise, and quitting smoking, as smoking was found to be the only risk factor that had a significant impact on the patient’s previous condition.
| Discussion | ▴Top |
This case underscores the necessity of considering AMI and its potential causes in young individuals diagnosed with STEMI. The patient, who was actively working, suffered from an AMI with smoking being the sole known risk factor. To accurately diagnose and identify such cases in the adolescent population, it is crucial to screen for risk factors and have a comprehensive understanding of the disease’s pathophysiology in this age group. Regardless of age, myocardial infarction should be considered in any patient experiencing chest pain [3].
While the causes of myocardial infarction may vary, ranging from atherosclerosis to non-atherosclerotic coronary artery abnormalities, hypercoagulable states, and adverse drug effects [3, 4], obtaining a thorough medical history is essential to identify the underlying cause and prevent misdiagnosis. Such data can help identify the risks in the younger population subset, and incorporating earlier screening methods would be beneficial.
The risk factors for coronary heart disease in young patients differ slightly from those in older patients. Conditions such as diabetes, high blood pressure, and chronic kidney disease are less prevalent among younger patients compared to older ones [4]. However, smoking is a significant risk factor for coronary heart disease in young individuals. Young patients who experience a heart attack, specifically STEMI, are more likely to suffer cardiac arrest during their initial hospital stay [2, 4]. While both younger and older patients usually undergo PCI at a specialized center, younger patients receive treatment more promptly from the onset of symptoms [4].
Smoking
The relationship between smoking tobacco and cardiovascular diseases (CVDs) encompasses various aspects. Smoking is strongly associated with the early development of atherosclerosis, starting from adolescence and continuing into young adulthood. This habit significantly increases the risk of several CVDs, including AMI, stroke, peripheral artery disease, aortic aneurysm, and sudden death [5, 6]. Second-hand smoke, specifically the components found in passive smoking such as carbonyls and particulate matter, also has notable detrimental effects on cardiovascular health, which exerts detrimental effects on every stage of atherosclerosis, hastening blood clot formation, impairing endothelial function, promoting inflammation, and constricting coronary arteries, even in individuals with initially healthy blood vessels, leading to an elevated risk of acute coronary events and hospitalizations [6].
Research indicates that young patients with AMI who smoke are frequently observed. On the other hand, risk factors like high blood pressure, diabetes, and chronic kidney disease are more commonly found in older patients with myocardial infarction. Additionally, it has been noted that young patients with myocardial infarction often exhibit significant blockage in a major heart artery called the LAD [5], which aligns with our own findings. Recent studies have also shown that young patients rarely experience angina pectoris before myocardial infarction. Instead, angina pectoris quickly progresses to AMI. In these studies, only 12% of young patients with STEMI had angina pectoris before the event, significantly lower than the percentage observed in older patients [4, 6]. STEMI in young patients typically lacks ischemic preconditioning and develops and progresses more rapidly than in older patients [7]. This highlights the increased importance of pre-screening due to the high risk of unpredictable and severe events in this population.
To effectively prevent AMI in young patients, the primary focus should be on assisting them in quitting smoking. Cigarette smoking is widely recognized as a significant risk factor for the development of CAD in this age group [6, 7]. Numerous studies have highlighted that a substantial proportion of young AMI patients are smokers, with rates ranging from 70% to 90%. Comparatively, a significantly larger percentage of young AMI patients were current smokers when compared to those above 40 years old (37.5% vs. 23.0%; P < 0.001). Among young patients, there was also a higher incidence of STEMI (62.0% vs. 50.0%; P < 0.001) and a greater prevalence of non-significant narrowing in the coronary arteries (14.4% vs. 6.8%; P < 0.001) [7].
Lipid profile abnormalities
The findings of the recent studies revealed a significant correlation between a poor lipid profile and the occurrence of STEMI in young adults. Elevated levels of LDL-C were found to be strongly associated with an increased risk of STEMI in this age group [8]. These results highlight the importance of monitoring and managing lipid levels, even in younger individuals, to prevent the occurrence of potentially life-threatening cardiovascular events.
Furthermore, other studies also emphasized the role of high triglyceride levels in contributing to STEMI risk. Elevated triglyceride levels were shown to be an independent risk factor for STEMI in young adults, even in the absence of other lipid abnormalities [4, 8]. This finding underscores the need to address not only LDL-C but also triglyceride levels in the management of cardiovascular health, particularly in the younger population.
Recent studies concluded that a poor lipid profile, characterized by high LDL-C and triglyceride levels, is strongly associated with the development of STEMI in young individuals. Among young survivors of STEMI, high cholesterol levels were more commonly observed other than smoking cigarettes [7, 8]. However, hypertension and diabetes were less prevalent in younger patients compared to older individuals [8]. These findings highlight the importance of early detection and intervention to optimize lipid profiles and reduce the risk of STEMI in this age group. Implementing lifestyle modifications, such as adopting a healthy diet, engaging in regular physical activity, and considering pharmacological interventions when necessary, could significantly contribute to preventing adverse cardiovascular events in young adults with poor lipid profiles.
Hypertension
Hypertension and STEMI occurring at a young age are concerning health issues with significant implications. The occurrence of hypertension in young adults has been rising in recent years [3]. According to a study published in the Journal of Heart, Lung, and Circulation, hypertension in young adults significantly increases the risk of developing CVDs, including STEMI. In line with angiographic findings related to CAD among young individuals, there is a higher tendency towards single-vessel disease, specifically the left main disease [3, 4].
Diabetes mellitus
Individuals with diabetes had a significantly higher risk of developing STEMI at a younger age compared to those without diabetes [4]. This suggests that diabetes mellitus may be a contributing factor to the early onset of STEMI in this population. Moreover, few other studies found that diabetic patients with STEMI had a higher incidence of multivessel disease, indicating a more severe form of CAD [8]. This finding suggests that the presence of diabetes may influence the extent and severity of coronary artery involvement in young patients with STEMI.
The researchers also analyzed various risk factors associated with the correlation between diabetes and STEMI in young age. They found that poor glycemic control, prolonged duration of diabetes, and the presence of other cardiovascular risk factors such as hypertension and dyslipidemia further increased the likelihood of developing STEMI in diabetic individuals [7, 8]. The result data above provide evidence for a strong correlation between diabetes mellitus and STEMI in young age. It highlights the need for increased awareness, screening, and comprehensive management of diabetes in young patients to prevent the early onset and severity of STEMI, thereby reducing the burden of CVD in this population.
Family history
Familial history has long been recognized as a significant risk factor for CAD [2, 5, 6]. Individuals with a family history of premature CAD, particularly in first-degree relatives, are at an elevated risk of developing the disease. Several genes associated with CAD susceptibility have been identified, including those involved in lipid metabolism, inflammation, and endothelial dysfunction. These genetic variations, combined with environmental factors, can significantly increase the likelihood of CAD manifestation at a young age [9].
While genetic factors contribute to CAD development, lifestyle choices also play a crucial role and can further augment the risk conferred by familial history. The interaction between genetic predisposition and modifiable lifestyle factors highlights the importance of comprehensive preventive strategies in individuals with a family history of CAD [6, 8]. The underlying mechanisms responsible for early-onset CAD are still being elucidated, with studies focusing on exploring the interplay between genetic factors, traditional risk factors, and the impact of lifestyle modifications [9].
Coagulation issue
Coagulation issues refer to abnormalities in the blood clotting process, which can lead to both bleeding disorders and clotting disorders. While these conditions are commonly associated with older individuals, there is emerging evidence of coagulation issues occurring in younger age groups [6]. A study published in a reputable medical journal found that an increasing number of young adults are being diagnosed with coagulation disorders, such as factor V Leiden mutation or protein C deficiency. These conditions disrupt the delicate balance of blood clotting, increasing the risk of abnormal bleeding or thrombosis [5, 6].
There is a growing body of evidence indicating a potential link between coagulation issues and CAD, particularly in young individuals. A comprehensive review highlighted the intricate interplay between these two conditions [6]. It is suggested that coagulation abnormalities, such as increased platelet aggregation or impaired fibrinolysis, could contribute to the development and progression of CAD. The presence of coagulation issues in young individuals may further accelerate the process of atherosclerosis, leading to premature CAD.
Substance use
Substance use can have a significant impact on myocardial infarction, particularly in young individuals [10]. Myocardial infarction, commonly known as a heart attack, occurs when the blood flow to the heart muscle is severely reduced or blocked, leading to damage or death of the heart tissue. While myocardial infarction is typically associated with older individuals, substance use can increase the risk of heart attack even among the young [2, 10].
Besides tobacco as the famous substance causing myocardial infarction, substances that pose a significant risk to the cardiovascular system, particularly in young people, are illicit drugs. Certain drugs, such as cocaine and amphetamines, can cause a sudden increase in blood pressure and heart rate, leading to a condition known as acute coronary syndrome. Cocaine use is increasingly being portrayed as a factor accountable for an increasing number of AMIs in the younger population. This drug causes transient arterial vasospasm associated with elevated heart rate and systolic blood pressure culminating in compromised coronary flow, which results in imbalance between oxygen demand and supply. Augmented thrombocyte aggregation stimulated by cocaine may be a direct factor triggering coronary artery thrombosis. Furthermore, cocaine is directly toxic to the myocardium, resulting in focal necrosis [10, 11].
Alcohol abuse is yet another substance-related factor that can impact myocardial infarction risk in young individuals [3, 10]. Furthermore, heavy drinking can contribute to the accumulation of fat in the blood, an increase in blood clotting factors, and an elevation in triglyceride levels, all of which can contribute to the development of atherosclerosis and subsequent heart attacks [7, 8, 10].
In conclusion, substance use can have a significant impact on the occurrence of myocardial infarction in young individuals. Tobacco, illicit drugs, and excessive alcohol consumption can all contribute to the development of cardiovascular risk factors, such as atherosclerosis and high blood pressure, which increase the likelihood of experiencing a heart attack. Young people must be aware of these risks and make informed decisions regarding substance use to protect their cardiovascular health.
Acknowledgments
We are deeply grateful to all those who contributed to the success of this case report project. This research project would not have been possible without the support and contributions of so many people. We are deeply grateful to all of those who helped to make this project a reality, and we hope that our findings will make a meaningful contribution to the field.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Informed consent has been obtained from the patient.
Author Contributions
Meutia Putri Aristya, Nada Putri Pranidya and Mery Natalia Hutapea: writers of the manuscript and data collectors. Afdhalun Anwar Hakim: mentoring and guiding throughout the writing process, patient’s doctor, source of patient’s information, and final editor.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Zasada W, Bobrowska B, Plens K, Dziewierz A, Siudak Z, Surdacki A, Dudek D, et al. Acute myocardial infarction in young patients. Kardiol Pol. 2021;79(10):1093-1098.
doi pubmed - Bajaj S, Shamoon F, Gupta N, Parikh R, Parikh N, Debari VA, Hamdan A, et al. Acute ST-segment elevation myocardial infarction in young adults: who is at risk? Coron Artery Dis. 2011;22(4):238-244.
doi pubmed - Michos ED, Choi AD. Coronary artery disease in young adults: a hard lesson but a good teacher. J Am Coll Cardiol. 2019;74(15):1879-1882.
doi pubmed - Sinha SK, Krishna V, Thakur R, Kumar A, Mishra V, Jha MJ, Singh K, et al. Acute myocardial infarction in very young adults: A clinical presentation, risk factors, hospital outcome index, and their angiographic characteristics in North India-AMIYA Study. ARYA Atheroscler. 2017;13(2):79-87.
pubmed pmc - Hill D, Waldman A, Vivek D. A 16-year-old with ST elevation myocardial infarction: case report and review of the literature. Cardiol Young. 2016;26(2):230-236.
doi pubmed - Liori S, Pappas C, Rallidis L. ST-elevation myocardial infarction in a 39-year-old patient with "normal" coronary arteries as a thrombotic complication of COVID-19. J Cardiol Cases. 2022;25(6):335-337.
doi pubmed pmc - Fotedar S, Garg A, Arora A, Chawla S. Study of lipid profile in young patients (age 40 years or below) with acute coronary syndrome. J Family Med Prim Care. 2022;11(6):3034-3039.
doi pubmed pmc - Akin F, Altun I, Ayca B, Kose N, Altun I. Associations of non-HDL-C and triglyceride/HDL-C ratio with coronary plaque burden and plaque characteristics in young adults. Bosn J Basic Med Sci. 2022;22(6):1025-1032.
doi pubmed pmc - Shah N, Kelly AM, Cox N, Wong C, Soon K. Myocardial infarction in the "Young": risk factors, presentation, management and prognosis. Heart Lung Circ. 2016;25(10):955-960.
doi pubmed - Lee HS, Pai R, Nazzal S, Mukherjee A. STEMI mimicker in a 26-year-old man. BMJ Case Rep. 2019;12(2):bcr-2018-224894.
doi pubmed pmc - Gallucci G, Tartarone A, Lerose R, Lalinga AV, Capobianco AM. Cardiovascular risk of smoking and benefits of smoking cessation. J Thorac Dis. 2020;12(7):3866-3876.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.