

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 15, Number 1, February 2024, pages 12-17

Preliminary Experience With Remimazolam for Procedural Sedation and as an Adjunct to General Anesthesia During Diagnostic and Interventional Cardiac Procedures
Holly Gillisa, c, Christopher McKeea, b, Kristin Chenaulta, b, Marco Corridorea, b, Joseph D. Tobiasa, b
aDepartment of Anesthesiology and Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA
bDepartment of Anesthesiology and Pain Medicine, The Ohio State University College of Medicine, Columbus, OH, USA
cCorresponding Author: Holly Gillis, Department of Anesthesiology and Pain Medicine, Nationwide Children’s Hospital, Columbus, OH 43205, USA
Manuscript submitted November 27, 2023, accepted January 12, 2024, published online February 28, 2024
Short title: Remimazolam and Cardiac Catheterization
doi: https://doi.org/10.14740/cr1595
| Abstract | ▴Top |
Background: Remimazolam is a benzodiazepine which, like midazolam, has sedative, anxiolytic, and amnestic properties. Ester metabolism results in a half-life of 5 - 10 min, a limited context sensitive half-life, and rapid recovery when the infusion is discontinued.
Methods: Following the Institutional Review Board (IRB) approval, we performed a retrospective chart review of patients who received remimazolam in the cardiac catheterization, cardiac magnetic resonance imaging (MRI), and electrophysiology suites. The primary objective was to assess efficacy and safety. The secondary objective was to describe bolus and infusion dosing of remimazolam and the need for adjunctive agents to optimize procedural sedation conditions.
Results: The study cohort included 26 patients with a median age of 18 years and a total of 33 anesthetic encounters. The most common procedures were endomyocardial biopsy or isolated hemodynamic assessment (right or left heart catheterization). Remimazolam was the primary agent for sedation in 82% of the procedures. The majority of cases (25 encounters, 76%) included a bolus dose of remimazolam prior to the start of an infusion. For those patients who received a starting bolus dose, dosing typically ranged between 30 and 110 µg/kg. Continuous infusion rates of remimazolam varied from 5 to 20 µg/kg/min. No adverse hemodynamic or respiratory effects were noted. Midazolam, fentanyl, and dexmedetomidine were the most frequently used adjunctive agents. One patient required transition to general anesthesia due to the need for a surgical intervention based on the findings of the cardiac catheterization. All other patients were effectively sedated.
Conclusions: Our preliminary experience demonstrates that remimazolam effectively provided sedation for diagnostic and therapeutic cardiovascular procedures. Future studies are needed to further define dosing parameters for both bolus dosing and continuous infusion as well as to compare remimazolam to other commonly used for procedural sedation in patients with congenital and acquired heart disease.
Keywords: Cardiac catheterization; Remimazolam; Total intravenous anesthesia; Congenital heart disease
| Introduction | ▴Top |
Remimazolam is a novel, ester metabolized derivative of the intravenous benzodiazepine, midazolam [1-3]. Like midazolam, it has sedative, anxiolytic, and amnestic properties and can be used as a primary agent or adjunct for procedural sedation and general anesthesia [4-7]. Remimazolam undergoes metabolism by tissue esterase with a half-life of 5 - 10 min thereby limiting its context sensitive half-life. These properties allow for its administration by bolus and continuous infusion, providing a deep level of sedation/anesthesia while allowing for rapid awakening when the infusion is discontinued. Preliminary experience in adults has demonstrated remimazolam to be an effective and safe agent for procedural sedation during upper and lower gastrointestinal endoscopy [1-3]. Success in these clinical arenas suggests its potential utility for other types of procedures.
Patients undergoing diagnostic or therapeutic procedures in the cardiac catheterization, operating rooms (ORs), and radiology areas may require procedural sedation to provide patient comfort and facilitate timely completion of the procedure. We present preliminary experience with the use of the novel benzodiazepine, remimazolam, as a primary agent for sedation or as an adjunct to general anesthesia in a cohort of pediatric and adult patients with acquired or congenital heart disease undergoing cardiac diagnostic and therapeutic procedures.
| Materials and Methods | ▴Top |
This study was approved by the Institutional Review Board of Nationwide Children’s Hospital (Columbus, Ohio). All study procedures were conducted in accordance with the guidelines of the Declaration of Helsinki. As a retrospective study with minimal risk, the need for individual written informed consent was waived. Patient confidentiality was maintained by the use of deidentified data and storage of data in a secure location on a password-protected network. Access to data was available only to collaborators directly involved in the study.
Prior to the addition of remimazolam to the OR formulary, departmental education was completed including discussion of the medication at a faculty and staff meeting, dissemination of published reports regarding its clinical use, and the development of departmental guidelines for preparation by pharmacy and dosing. For clinical use, remimazolam was dispensed from the OR pharmacy in a concentration of 20 mg/8 mL (2.5 mg/mL). It was reconstituted using normal saline from a lyophilized powder according to the manufacturer’s recommendations. After an order was placed using the electronic medical record for intraoperative use, the medication was delivered to the OR in a syringe and administered by an infusion pump.
Dosing recommendations for bolus and infusions rates were determined from the available literature and provided in µg/kg or µg/kg/min based on our usual practice for OR infusions in a tertiary care pediatric hospital, not mg/kg or mg/kg/h as initially reported in the adult literature. Preliminary guidelines included a bolus dose of 50 - 200 µg/kg (maximum of 5 mg) and an infusion starting at 3 - 5 µg/kg/min with an increase up to 30 µg/kg/min as needed. As part of an ongoing departmental quality assurance program, patients who received remimazolam for procedural sedation or as an adjunct to general anesthesia were identified by the pharmacy department on a quarterly basis. This list was reviewed to ensure adherence to initial departmental guidelines. This list of patients was used as the basis for the retrospective review reported in this manuscript.
The following demographic data were obtained by manual chart review: age, weight, body mass index and gender. Procedural information included the type of procedure, duration, intraoperative concerns, anesthetic and sedative agents used, and mode of administration (continuous or intermittent). Intraoperative and postoperative adverse effects including hypotension requiring intervention, bradycardia, respiratory arrest, apnea, or hypoventilation were identified. Additionally, the use of rescue medications including anticholinergic agents (atropine or glycopyrrolate), or vasoactive agents (epinephrine, phenylephrine, vasopressin, or ephedrine) was noted, or the need to pause the infusion was observed in association with hemodynamic changes. Information regarding remimazolam dosing included the dose, changes in dosing during the intraoperative period, mode of administration (intermittent or continuous), and duration of infusion. Efficacy was determined by a review of subjective assessments from the electronic medical record, including the need for adjunctive sedatives, analgesic agents, recall and/or need to convert to general anesthesia. Descriptive study statistics for this retrospective study include the number, mean ± standard deviation (SD), median, and range.
| Results | ▴Top |
The study cohort included 26 individual patients who required procedural sedation and anesthesia care for 33 procedures. The patients ranged in age from 0 to 59 years (median age 18 years) and in weight from 5.9 to 185 kg (Table 1). The most common procedures were endomyocardial biopsy following a heart transplant or isolated hemodynamic assessment (right and/or left heart catheterization) in the cardiac catheterization suite.
 Click to view | Table 1. Demographic Date of the Retrospective Study Cohort |
Remimazolam was the primary agent for sedation during 27 of the 33 encounters (82%) (Table 2). In the remaining six instances, remimazolam was used as an adjunct to either a volatile anesthetic agent (n = 3) or dexmedetomidine (n = 3). The majority of cases (25 encounters, 76%) included a bolus dose of remimazolam prior to the start of an infusion. For those patients who received a bolus dose, doses typically ranged between 30 and 110 µg/kg. However, in two patients, the bolus dose provided (490 and 250 µg/kg) was 2.5 - 5 times higher than the typical bolus dose. The highest bolus dose (490 µg/kg) was the result of a pump programing error that resulted in a 10-fold increase of the intended dose. The infusion in both patients was started immediately after the bolus, although at mid to lower ranges (10 and 8 µg/kg/min, respectively). Neither patient experienced hemodynamic or respiratory compromise related to the higher bolus dose.
Click to view | Table 2. Remimazolam Dosing and Use of Adjuncts |
Remimazolam infusion rates varied widely from 2 to 20 µg/kg/min (Fig. 1). Infusions were rarely started at less than 10 µg/kg/min (12%) while approximately one-third (39%) were started at 10 µg/kg/min. Adjunct sedative or analgesic agents were used in the majority of cases, most commonly fentanyl and/or dexmedetomidine (Table 2). Over time, following its addition to our hospital formulary, remimazolam was used in patients of younger ages. The two youngest patients that received remimazolam were during the last 2 months of the retrospective review period of this report.
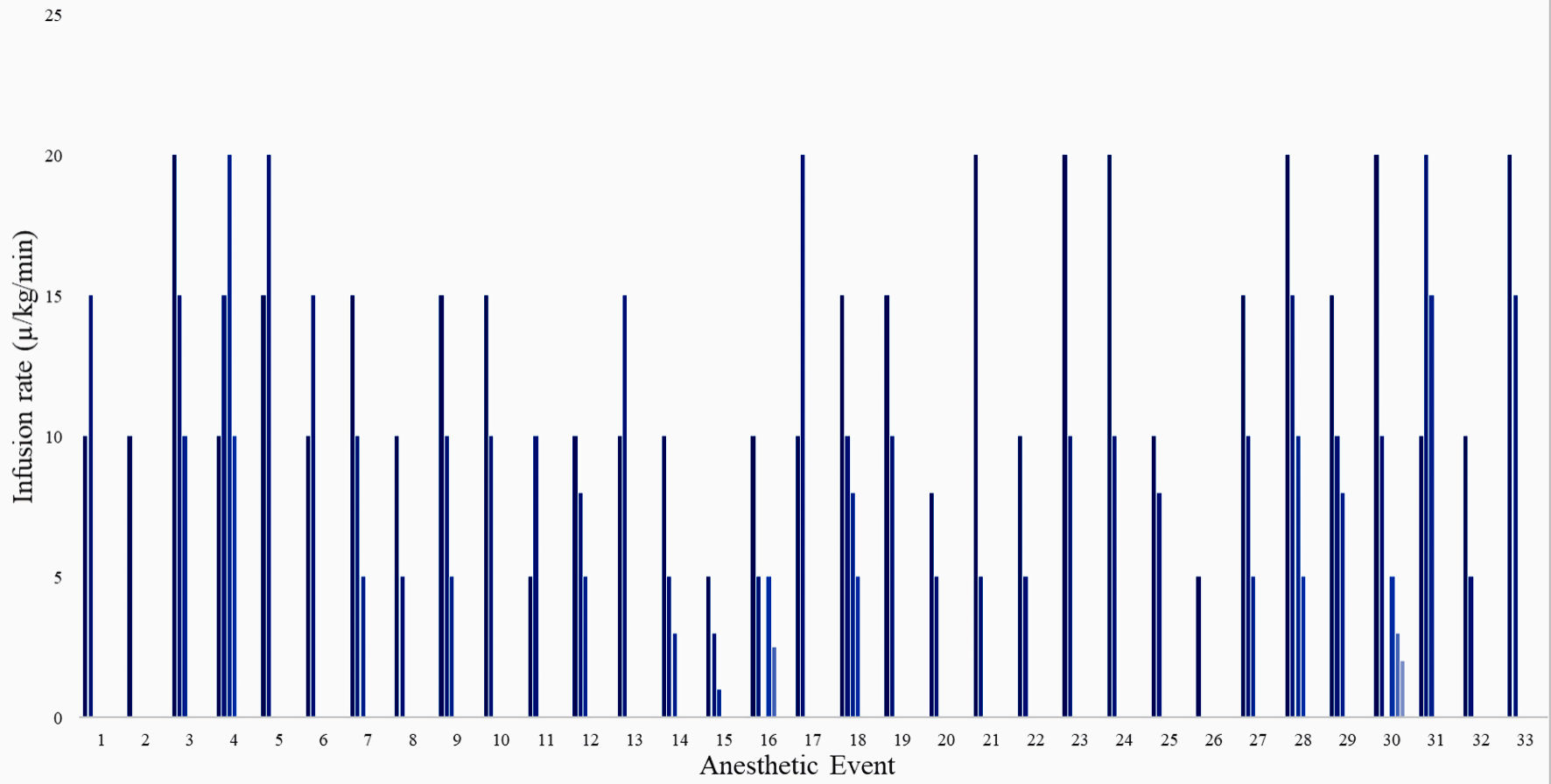 Click for large image | Figure 1. Remimazolam infusion rates by procedural sedation encounter. |
No significant hemodynamic or respiratory adverse effects were noted in any patient. For 28 of the procedures, a native airway with a nasal canula was the only airway support provided. In three of the procedures, there was pre-existing airway support (endotracheal intubation, a tracheostomy, or bilevel positive airway pressure). One patient, who received remimazolam as an adjunct to general anesthesia, required endotracheal intubation to tolerate transcatheter aortic valve replacement. One patient required endotracheal intubation after initial procedural sedation with remimazolam and a native airway due to findings during the cardiac catheterization assessment that required surgical intervention. One patient required placement of a nasal trumpet for upper airway obstruction. In this patient, adjuncts included ketamine and dexmedetomidine. No other change in airway management was required due to the depth of sedation. No patient required the administration of vasoactive agents, anticholinergic agents, or fluid to treat hemodynamic changes. There was no documented report of recall in any patient regardless of age. Conversion to general anesthesia was required only if the requirements of the procedure itself changed and not based on an inadequate level of sedation.
| Discussion | ▴Top |
Our preliminary experience demonstrates that remimazolam is an effective agent for procedural sedation and as an adjunct to general anesthesia during investigative and diagnostic cardiac procedures, including cardiac catheterization in patients with congenital or acquired heart disease. The median bolus dose was 50 µg/kg, followed by an infusion at 2 - 20 µg/kg/min. In the majority of patients, remimazolam was the primary sedative agent during a variety of diagnostic and therapeutic cardiac procedures with maintenance of spontaneous ventilation and a native airway. No significant hemodynamic or respiratory adverse events were noted.
Pediatric cardiac catheterization was first reported in 1947 and has seen increased use beginning in 1968 with the advent of balloon atrial septostomy [8, 9]. Over the past two decades, there has been a significant increase in the availability of interventional procedures in lieu of open surgical procedures. During cardiac catheterization and other diagnostic and therapeutic cardiac procedures, there are a wide variety of practice models and a diverse array of agents that have been used to provide sedation, analgesia, and general anesthesia [10, 11]. In addition to providing sedation and analgesia, a limited impact on hemodynamic and electrophysiologic function is a key component of agents chosen during cardiac catheterization and other procedures in patients with congenital and acquired heart disease [11, 12]. As many of these procedures are performed with a native airway, a limited impact on respiratory function and upper airway parent is mandatory.
In July 2020, remimazolam received approval from the United States Food and Drug Administration (FDA) for the induction and maintenance of procedural sedation in adults. To date, published studies outlining the use of remimazolam for sedation during cardiac catheterization procedures are limited. This may be a result of the use of limited sedation for cardiac catheterization in adults and the lack of familiarity with remimazolam use in pediatric-aged patients. However, there is a growing body of literature outlining the use of remimazolam as an adjunct to general anesthesia in patients with acquired cardiac disease [13-18]. Hu et al compared etomidate with remimazolam for the induction of anesthesia prior to cardiac surgery [13]. In addition to its hemodynamic stability, there was less pain on injection and decreased myoclonus with remimazolam compared to etomidate. Similar hemodynamic stability has been noted by other authors. When compared to propofol in a prospective trial of 67 adult, American Society of Anesthesiologists (ASA) physical status III surgical patients undergoing general anesthesia, there was less hypotension with remimazolam compared to propofol when used as part of the regimen for general anesthesia [14]. In an open label prospective trial, Nakanishi et al reported effective anesthesia and hemodynamic stability with remimazolam for anesthetic induction in a cohort of 20 adult patients (ASA physical classification IV) with aortic stenosis [15]. An additional reported benefit of remimazolam is a decreased incidence of postoperative delirium when compared to propofol [16-18].
Aside from its sedative properties, previous work has investigated the effects of remimazolam on electrophysiologic function [19, 20]. Kleiman et al reported no effect of remimazolam (bolus doses of 10 mg and 20 mg administered over 1 min) on repolarization and the QT/QTc ratio in healthy control subjects [19]. We have previously reported anecdotal experience with the use of remimazolam for procedural sedation in the cardiac catheterization suite in three patients with conduction abnormalities including first-degree heart block and pacemaker dependency with right bundle branch block [20]. In these patients, we postulated that remimazolam would be advantageous over dexmedetomidine and propofol given their negative effects on chronotropic and dromotropic function.
Limitations to the current study include its retrospective design without a comparator or control group. As such, we are not able to make superiority comparisons between traditional sedative agents and remimazolam-based sedation. Additionally, as a retrospective study, specific adverse effects may not be readily available from chart review. Furthermore, specific indications of the efficacy of the medication such as sedation scores or information from depth of anesthesia monitors may not be available for all patients. However, our clinical experience provides preliminary experience with the efficacy of remimazolam and supports its limited effects on respiratory and hemodynamic function as these procedures were accomplished with a native airway and spontaneous ventilation. As our clinical experience has demonstrated the efficacy of remimazolam in this clinical scenario, we believe that future prospective, randomized trials with a direct comparison to other commonly used agents for procedural sedation may be indicated. Given the retrospective nature of the report, definitive recommendations regarding dosing cannot be made as we noted variability in dosing among the anesthesia providers. Most providers chose to use a bolus dose followed by an infusion. The starting infusion was 5 - 20 µg/kg/min with dosing titration in increments of 2 - 5 µg/kg/min. Finally, as a large tertiary care pediatric cardiac center, we care for a significant number of adult patients with congenital heart disease. As such, there was significant variation in the ages of the patients reported. Although the median age was 18 years, the patients ranged in age from infancy to 59 years of age. Future studies are also needed to evaluate remimazolam dosing parameters, efficacy, and adverse effects across various age ranges and procedure types in pediatric and adult patients with congenital or acquired heart disease. Over the course of the retrospective time frame of this study, our group used remimazolam in younger and younger patients. However, we did not specifically compare efficacy, dosing parameters or adverse effect profile across age ranges given the limited size of the various age groups.
The role of pediatric cardiac anesthesiologist in the cardiac catheterization suite has evolved over the last 20 years [19, 20]. With the ability to perform endovascular assessment and, more recently, treatment options, this role will continue to grow. Commonly chosen agents for sedation include propofol, α2-adrenergic agonists such as dexmedetomidine, ketamine, and opioids. As clinical experience increases, it is apparent that there may be a role for remimazolam with its limited context sensitive half-life and non-organ dependent metabolism and elimination [21]. It may offer rapid emergence times due to its novel tissue esterase-based metabolism. Clinical experience has demonstrated limited effects on hemodynamic function, electrophysiologic properties, and respiratory function within FDA outlined dosing guidelines [22]. Its limited effects on airway and respiratory function generally allows maintenance of a native airway and spontaneous ventilation during procedural sedation.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
As a retrospective study, the need for individual written informed consent was waived.
Author Contributions
Data collection and analysis, preparation of initial and subsequent drafts, review of final manuscript, patient care: HG. Clinical care of patients, review of drafts and final manuscript: CM, KC, and MC. Study oversight, review of drafts and final manuscript: JDT.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Lee A, Shirley M. Remimazolam: a review in procedural sedation. Drugs. 2021;81(10):1193-1201.
doi pubmed - Morimoto Y. Efficacy and safety profile of remimazolam for sedation in adults undergoing short surgical procedures. Ther Clin Risk Manag. 2022;18:95-100.
doi pubmed pmc - Xiao X, Xiao N, Zeng F, Chen H, Zhang L, He X. Gastroscopy sedation: clinical trial comparing propofol and sufentanil with or without remimazolam. Minerva Anestesiol. 2022;88(4):223-229.
doi pubmed - Zhang Y, Dai G, Xu H, Liu Y, Liao M, Zhang X. Safety and efficacy of remimazolam compared with propofol in induction of general anesthesia: a reply. Minerva Anestesiol. 2022;88(3):194-195.
doi pubmed - Hari Y, Satomi S, Murakami C, Narasaki S, Morio A, Kato T, Tsutsumi YM, et al. Remimazolam decreased the incidence of early postoperative nausea and vomiting compared to desflurane after laparoscopic gynecological surgery. J Anesth. 2022;36(2):265-269.
doi pubmed - Kim KM. Remimazolam: pharmacological characteristics and clinical applications in anesthesiology. Anesth Pain Med (Seoul). 2022;17(1):1-11.
doi pubmed pmc - Sato T, Nishiwaki K. Comparison of remimazolam and propofol in anesthetic management for awake craniotomy: a retrospective study. J Anesth. 2022;36(1):152-155.
doi pubmed - Bing RJ, Vandam LD, et al. Catheterization of the coronary sinus and the middle cardiac vein in man. Proc Soc Exp Biol Med. 1947;66(1):239.
doi pubmed - Rashkind WJ, Miller WW. Transposition of the great arteries. Results of palliation by balloon atrioseptostomy in thirty-one infants. Circulation. 1968;38(3):453-462.
doi pubmed - Motas D, McDermott NB, VanSickle T, Friesen RH. Depth of consciousness and deep sedation attained in children as administered by nonanaesthesiologists in a children's hospital. Paediatr Anaesth. 2004;14(3):256-260.
doi pubmed - Bernard PA, Ballard H, Schneider D. Current approaches to pediatric heart catheterizations. Pediatr Rep. 2011;3(3):e23.
doi pubmed pmc - Lam JE, Lin EP, Alexy R, Aronson LA. Anesthesia and the pediatric cardiac catheterization suite: a review. Paediatr Anaesth. 2015;25(2):127-134.
doi pubmed - Hu B, Zhang M, Wu Z, Zhang X, Zou X, Tan L, Song T, et al. Comparison of remimazolam tosilate and etomidate on hemodynamics in cardiac surgery: a randomised controlled trial. Drug Des Devel Ther. 2023;17:381-388.
doi pubmed pmc - Doi M, Hirata N, Suzuki T, Morisaki H, Morimatsu H, Sakamoto A. Safety and efficacy of remimazolam in induction and maintenance of general anesthesia in high-risk surgical patients (ASA Class III): results of a multicenter, randomized, double-blind, parallel-group comparative trial. J Anesth. 2020;34(4):491-501.
doi pubmed - Nakanishi T, Sento Y, Kamimura Y, Tsuji T, Kako E, Sobue K. Remimazolam for induction of anesthesia in elderly patients with severe aortic stenosis: a prospective, observational pilot study. BMC Anesthesiol. 2021;21(1):306.
doi pubmed pmc - Hirata N. Remimazolam for cardiovascular anesthesia. J Anesth. 2023;37(6):825-827.
doi pubmed - Aoki Y, Kurita T, Nakajima M, Imai R, Suzuki Y, Makino H, Kinoshita H, et al. Association between remimazolam and postoperative delirium in older adults undergoing elective cardiovascular surgery: a prospective cohort study. J Anesth. 2023;37(1):13-22.
doi pubmed - Kaneko S, Morimoto T, Ichinomiya T, Murata H, Yoshitomi O, Hara T. Effect of remimazolam on the incidence of delirium after transcatheter aortic valve implantation under general anesthesia: a retrospective exploratory study. J Anesth. 2023;37(2):210-218.
doi pubmed - Kleiman RB, Darpo B, Thorn M, Stoehr T, Schippers F. Potential strategy for assessing QT/QTc interval for drugs that produce rapid changes in heart rate: Electrocardiographic assessment of the effects of intravenous remimazolam on cardiac repolarization. Br J Clin Pharmacol. 2020;86(8):1600-1609.
doi pubmed pmc - Kalsotra S, Khan S, McKee C, Tobias JD. Remimazolam as the primary agent for sedation during cardiac catheterization in three patients with comorbid cardiac conduction abnormalities. Cardiol Res. 2023;14(1):86-90.
doi pubmed pmc - Stohr T, Colin PJ, Ossig J, Pesic M, Borkett K, Winkle P, Struys M, et al. Pharmacokinetic properties of remimazolam in subjects with hepatic or renal impairment. Br J Anaesth. 2021;127(3):415-423.
doi pubmed - US Food and Drug Administration, Center for Drug Evaluation and Research. Byfavo NDA 212295/S-002 approval letter, October 9, 2020. Retrieved January 4, 2024, from https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2021/212295Orig1s002ltr.pdf and https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/212295s000lbl.pdf.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.