

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 15, Number 3, June 2024, pages 144-152

Remnant Cholesterol and Carotid Intraplaque Neovascularization Assessed by Contrast-Enhanced Ultrasonography in Patients With Ischemic Stroke
Yan Songa, Ying Danga, Jun Fengb, Li Tao Ruana, c
aDepartment of Ultrasound, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, China
bDepartment of Vascular Surgery, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, China
cCorresponding Authors: Li Tao Ruan, Department of Ultrasound, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi Province 710061, China
Manuscript submitted March 9, 2024, accepted April 3, 2024, published online June 25, 2024
Short title: Remnant Cholesterol And Carotid IPN
doi: https://doi.org/10.14740/cr1634
| Abstract | ▴Top |
Background: We investigated the relationship between remnant cholesterol and carotid intraplaque neovascularization (IPN) assessed by contrast-enhanced ultrasonography (CEUS) in patients with ischemic stroke.
Methods: This was a single-center study. Remnant cholesterol is calculated as total cholesterol minus low-density lipoprotein cholesterol (LDL-C) minus high-density lipoprotein cholesterol (HDL-C). All patients underwent CEUS. IPN is graded according to the presence and location of microbubbles within each plaque.
Results: The cohort included 110 patients with ischemic stroke. Patients with an IPN grading of 2 had higher triglyceride (TG), non-HDL-C, and remnant cholesterol concentrations than those with an IPN grading of < 2 (TG: 1.45 ± 0.69 vs. 0.96 ± 0.24 mmol/L, P < 0.001; non-HDL-C: 2.63 ± 0.85 vs. 2.31 ± 0.64 mmol/L, P = 0.037; remnant cholesterol: 0.57 ± 0.23 vs. 0.44 ± 0.07 mmol/L, P < 0.001). The multivariate-adjusted odds ratio (95% confidence interval) for remnant cholesterol was 27.728 (2.714 - 283.253) for an IPN grading of 2 in the subset of patients with an optimal LDL-C concentration.
Conclusions: The remnant cholesterol concentration is significantly associated with carotid IPN on CEUS in patients with ischemic stroke with an optimal LDL-C concentration. Remnant cholesterol may be an important indicator of risk stratification in patients with ischemic stroke.
Keywords: Remnant cholesterol; Stroke; Neovascularization; Contrast-enhanced ultrasonography; Plaque
| Introduction | ▴Top |
Numerous studies have suggested that lowering low-density lipoprotein cholesterol (LDL-C) could significantly reduce the risk of cardiovascular disease [1]. However, despite the reduction in LDL-C achieved with statins, there is still a significant residual risk of recurrent cardiovascular events [2]. Part of this residual risk may be related to an increase in the concentration of remnant cholesterol [3], which refers to all triglyceride (TG)-rich lipoproteins. In the fasting state, remnant cholesterol consists of chylomicron remnants, very-low-density lipoprotein (VLDL), and intermediate-density lipoprotein (IDL), while in the non-fasting state, remnant cholesterol consists of only VLDL and IDL [4]. Recent studies have revealed a causal relationship between remnant cholesterol and both cardiovascular disease and all-cause mortality [5, 6]. A recent study noted that a high remnant cholesterol concentration was associated with an increased risk of ischemic stroke [7]. Possible reasons for the atherogenic risk of remnant cholesterol include retention of remnant cholesterol in the intima [8], direct uptake of remnant cholesterol by macrophages [9], and induction of an inflammatory state [10]. However, fewer studies have been conducted on the relationship between remnant cholesterol and the characteristics of vulnerable carotid plaques.
Carotid artery examination is invaluable for atherosclerosis screening. Intraplaque neovascularization (IPN) is one of the characteristics of vulnerable plaques [11], and evidence suggests that contrast-enhanced ultrasonography (CEUS) can be successfully employed to assess and quantify carotid IPN [12, 13], which has led to its widespread use. Studies have shown that carotid IPN assessed by CEUS can predict cardiovascular and cerebrovascular events [14-16]. Therefore, the aim of this study was to assess the association between remnant cholesterol and carotid IPN using CEUS. We also investigated the relationship between remnant cholesterol and carotid IPN in patients with optimal LDL-C concentrations.
| Materials and Methods | ▴Top |
Study design and patients
A total of 155 patients were enrolled at our institution from 2015 to 2018. All patients were hospitalized because of ischemic stroke or transient ischemic attack. All of the patients underwent brain computed tomography (CT) and/or magnetic resonance imaging (MRI) within 1 week. All of the patients also underwent CEUS within 1 week after admission. All of the patients had at least one carotid atherosclerotic plaque.
Forty-five patients without a fasting lipid profile < 7 days prior to CEUS were excluded. The remaining 110 patients were included in the analysis. Figure 1 presents the patient selection and study design. The inclusion criteria were as follows: 1) age ≥ 50 years; and 2) ischemic stroke or transient ischemic attack within 30 days before inclusion. Transient ischemic attack is defined as transient neurological deficits caused by focal cerebral or retinal ischemia lasting less than 1 h without evidence of significant cerebral infarction [17]. The presence of transient ischemic attack was evaluated by clinicians. The exclusion criteria were as follows: 1) previous carotid endarterectomy; 2) cardiogenic shock, acute coronary syndrome, major surgery, pulmonary edema, serious infection or trauma in the previous 4 weeks, and severe liver disease.
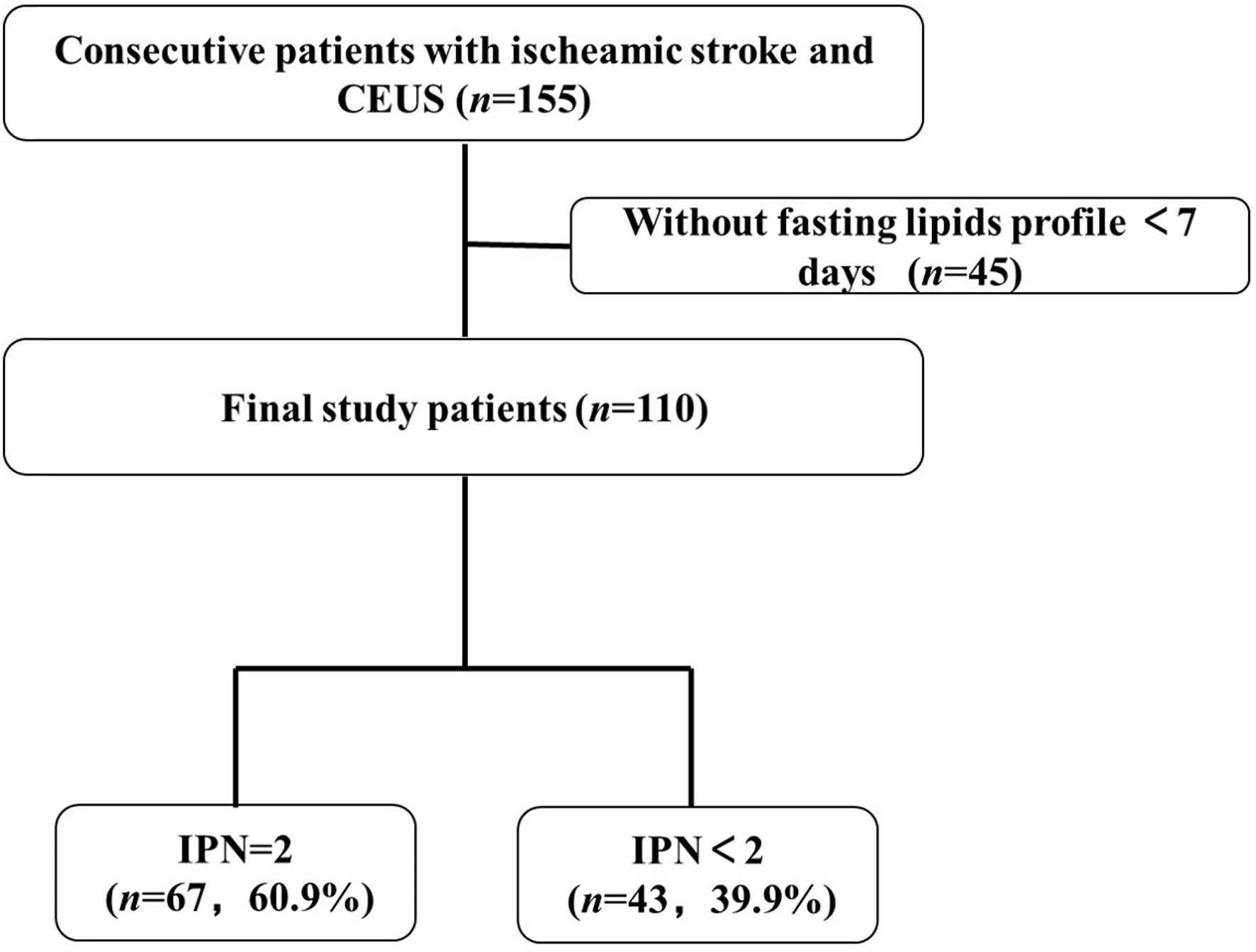 Click for large image | Figure 1. Patient selection and study design. CEUS: contrast-enhanced ultrasonography; IPN: intraplaque neovascularization. |
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institution. This study was approved by our hospital ethics committee, and all participants provided written informed consent (XJTU1AF2020LSK-058).
Data collection
The data on clinical characteristics, lifestyle risk factors (current smoking), medical history (stroke, hypertension, diabetes mellitus), medication use (antihypertensive and lipid-lowering medications), and ASCO (A = atherosclerosis; S = small-vessel disease; C = cardiac source; O = other cause) score [18] were collected. Three grades of likelihood are considered: grade 1, definitely a potential cause of the index stroke; grade 2, causality uncertain; grade 3, unlikely a direct cause of the index stroke (but disease is present). In addition, when no disease is present, patients are graded 0 [18]. Three blood pressure measurements were obtained at baseline by trained nurses according to the protocol adapted from procedures recommended by the American Heart Association [19]. Diabetes mellitus was defined as a hemoglobin A1c of ≥ 6.5% or use of anti-diabetes medications.
Fasting blood samples were drawn from the patients within 24 h of hospital admission. Plasma glucose concentrations were obtained using a modified hexokinase enzymatic method [20]. Serum lipids, including total cholesterol (TC), TG, and high-density lipoprotein cholesterol (HDL-C), were enzymatically measured on an automatic biochemical analyzer (LAbOSPECT 008AS; HITACHI, Japan) with commercial reagents. The LDL-C concentration was calculated using the Friedewald equation when the TG concentration was ≤ 4.5 mmol/L, or it was directly measured when the TG concentration was > 4.5 mmol/L. Remnant cholesterol was calculated as the fasting TC concentration minus the HDL-C concentration minus the LDL-C concentration [3]. Non-HDL-C was calculated as the TC concentration minus the HDL-C concentration [3]. The optimal LDL-C concentration was defined by the guideline-recommended treatment target of < 1.8 mmol/L for patients at a very high risk of cardiovascular disease [21].
Standard carotid artery ultrasonography
Standard carotid ultrasonography was performed in all patients at the screening visit with an 11.0-MHz linear-array transducer (Prosound LOGIQ-E9; GE, Fairfield, CT, US). According to the Mannheim consensus, an atherosclerotic plaque represents a change in the local vessel structure resulting from invasion of the arterial wall of ≥ 1.5 mm in thickness [22]. The type of echo was classified according to the Gray-Weale echogenicity grading classification criteria [23], as follows: uniformly echolucent (class I); predominantly echolucent (class II); predominantly echogenic (class III); or uniformly echogenic or extensively calcified (class IV). Plaque stenosis was divided into three groups according to the guidelines for blood flow velocity: < 50%, 50-69%, and 70-99% [24]. If the plaque was bilateral, the carotid plaque on the side consistent with stroke symptoms was analyzed. In the present study, all patients were diagnosed with stroke on only one side by CT or MRI. In patients with more than one separate plaque in the carotid artery on the side consistent with stroke symptoms, only the thickest plaque was studied.
CEUS and IPN analysis
CEUS was performed as described previously [25]. CEUS scans were performed and analyzed by two researchers with 5 years of experience in CEUS. Carotid CEUS studies were performed with the same machine used for the standard studies, with the addition of a 9L probe with a 7-MHz transmission frequency. Carotid CEUS was performed with ultrasound contrast agent (Sonovue; Bracco, Milan, Italy) suspended in 5 mL saline. A bolus of contrast agent (2.0 mL) was injected into the median cubital vein, followed immediately by 5 mL saline.
For semiquantitative analysis of neovascularization, the rapid movement of echogenic reflectors within the plaque was identified as neovascularization, which was graded as follows [13]: 0 = no visible microbubbles in the plaque; 1 = moderate microbubbles confined to the shoulder and/or adventitial side of the plaque; 2 = extensive microbubbles throughout the plaque (Fig. 2).
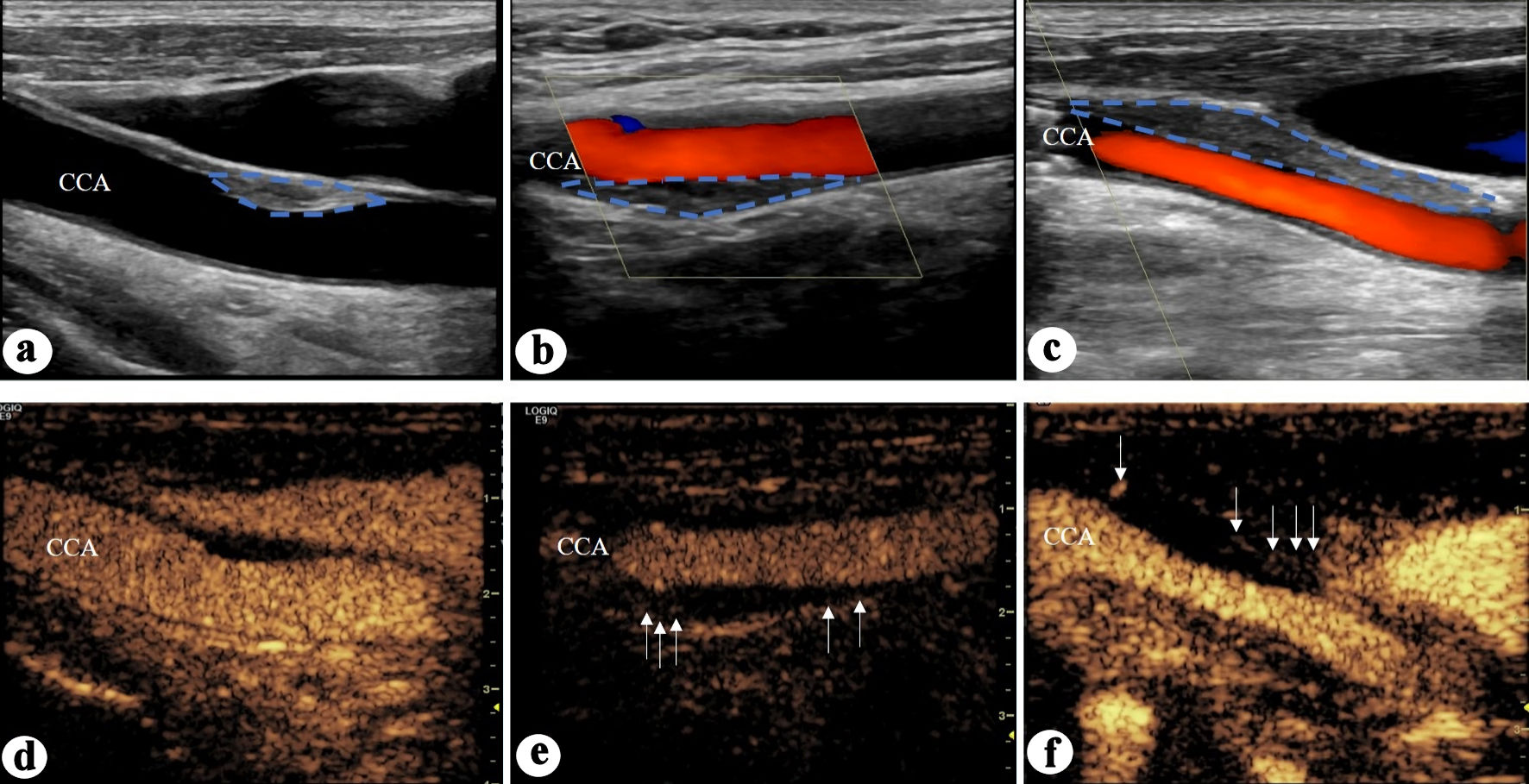 Click for large image | Figure 2. Semiquantitative analysis of neovascularization. IPN grading 0: no visible microbubbles in the plaque; IPN gradingg1: moderate microbubbles confined to the shoulder and/or adventitial side of the plaque; IPN grading 2: extensive microbubbles throughout the plaque. (a-c) Common carotid artery plaques in which the blue dotted line marks the plaque. (d-f) Contrast-enhanced ultrasonography images of the carotid artery. (d) IPN grading 0. (e) IPN grading 1. (f) IPN grading 2 (white arrow marking the continuous microbubble in the plaque (defined as IPN)). CCA: common carotid artery; IPN: intraplaque neovascularization. |
The correlation between the semiquantitative assessments of neovascularization was conducted by two researchers. The IPN analyses of 20 random plaques performed by the two researchers were compared using the Bland-Altman ± intraclass correlation coefficient (Fig. 3).
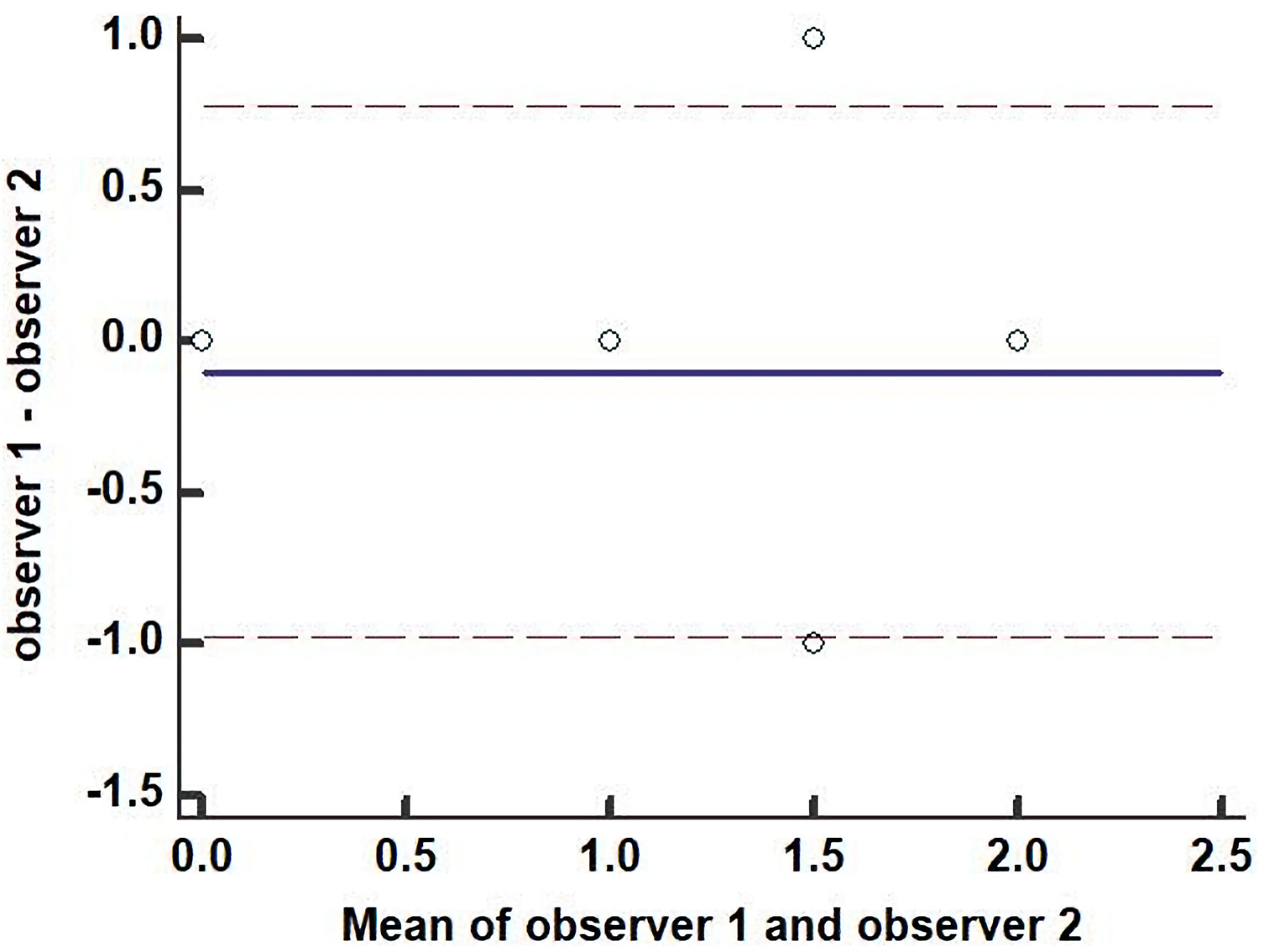 Click for large image | Figure 3. Correlation coefficient of IPN between the two observers. The IPN analyses of 20 random plaques performed by the two researchers were compared using the Bland-Altman ± intraclass correlation coefficient. IPN: intraplaque neovascularization. |
Statistical analysis
Statistical analyses were performed with IBM SPSS Statistics for Windows, version 20.0 (IBM, Armonk, NY, US). Normally distributed information is denoted as mean ± standard deviation, and non-normally distributed information is denoted as interquartile range (25th and 75th percentiles). The parameters were compared between the low and high remnant cholesterol groups and between the IPN grading < 2 and IPN grading = 2 groups using the Chi-square test or Fisher’s exact test for categorical variables and the unpaired t-test or the Mann-Whitney U test for continuous variables, as appropriate. The correlations between lipid parameters were assessed using Spearman’s rank correlation coefficient. The univariate analysis was performed to identify predictors of an IPN grading of 2 among the clinical and lipid variables. The multivariate logistic regression analysis was performed in the subset of patients with an optimal LDL-C concentration to identify predictors of an IPN grading of 2. A P value of < 0.05 was considered statistically significant. In logistic regression, the odds ratio (OR) is used to measure the extent to which two values of an independent variable affect the dependent variable.
| Results | ▴Top |
Patients’ characteristics
A total of 110 patients were included in the study. The mean age of the patients was 68.78 ± 8.65 years, and 98 patients (89.1%) were male. The baseline characteristics of the patients according to an IPN grading of < 2 and an IPN grading of 2 are presented in Table 1. At the time of CEUS, 102 patients (92.7%) were taking statins. The prevalence of existing statin therapy was not significantly different between patients with an IPN grading of < 2 and those with an IPN grading of 2.
 Click to view | Table 1. Clinical Characteristics According to Carotid IPN < 2 and IPN = 2 of Stroke Onset Side |
The mean TG, non-HDL-C, and remnant cholesterol concentrations were 1.26 ± 0.61, 2.50 ± 0.79, and 0.52 ± 0.19 mmol/L, respectively. The TG, non-HDL-C, and remnant cholesterol concentrations were significantly higher in patients with an IPN grading of 2 than in those with an IPN grading of < 2 (Table 1). The remnant cholesterol concentration was strongly correlated with the fasting TG concentration (r = 0.596, P < 0.001), poorly correlated with the non-HDL-C concentration (r = 0.217, P = 0.023), and inversely correlated with the HDL-C concentration (r = -0.314, P = 0.001). The LDL-C concentration was optimal in 51 patients (46.4%), 47 of whom (92.2%) were on statins.
The baseline carotid plaque characteristics according to the IPN grading are presented in Table 1. Of the 110 patients, 83 (75.5%) had bilateral carotid plaques, while the remainder had plaques on one side only, including 13 patients (11.8%) with plaques on the right side and 14 patients (12.7%) with plaques on the left side. Of the 110 patients, 56 (50.9%) had right-sided lesions and 54 (49.1%) had left-sided lesions according to the stroke onset side identified by CT or MRI. There were 17 patients (15.5%) with mild stenosis, 12 patients (10.9%) with moderate stenosis, and 81 patients (60.9%) with severe stenosis on the onset side according to digital subtraction angiography. The mean plaque thickness on the onset side was 4.17 ± 1.02 mm. No patients underwent carotid endarterectomy (CEA). A total of 61 patients underwent carotid artery stenting (CAS), including 25 cases on the right side and 36 cases on the left side. All of the patients underwent CEUS. The average IPN (aIPN) grading of the carotid plaques on both sides was 1.39 ± 0.56. The aIPN was significantly higher in patients with an IPN grading of 2 than in those with an IPN grading of < 2.
Predictors of an IPN grading of 2
In the univariate analysis, an IPN grading of 2 defined by CEUS was associated with the TG, non-HDL-C, remnant cholesterol, and glucose concentrations (Table 2). In the age- and sex-adjusted model, the OR (95% confidence interval (CI)) was 11.092 (3.980 - 30.908) for remnant cholesterol. After further adjustment for smoking history, hypertension, and diabetes mellitus in model 2, the OR (95% CI) was 12.221 (4.043 - 36.940) for remnant cholesterol (Table 2).
Click to view | Table 2. Univariable and Multivariable Analysis for IPN = 2 of Stroke Onset Side in the Study Population (N = 110) |
In the univariate analysis of patients with an optimal LDL-C concentration (n = 51), an IPN grading of 2 was associated with hypertension, TG concentration, and remnant cholesterol concentration (Table 3). In the age- and sex-adjusted model, the OR (95% CI) was 17.565 (3.172 - 97.269) for remnant cholesterol. After further adjustment for smoking history, hypertension, and diabetes mellitus in model 2, the OR (95% CI) was 27.728 (2.714 - 283.253) for remnant cholesterol (Table 3).
Click to view | Table 3. Univariable and Multivariable Analysis for IPN = 2 of Stroke Onset Side in the Subset of Patients With Optimal LDL-C levels (N = 51) |
| Discussion | ▴Top |
In this retrospective study, the remnant cholesterol concentration in patients with ischemic stroke was associated with carotid IPN assessed by CEUS. Furthermore, the relationship between the remnant cholesterol concentration and IPN persisted in patients with ischemic stroke who had an optimal LDL-C concentration. Our findings suggest that the fasting remnant cholesterol concentration is associated with plaque vulnerability in patients with ischemic stroke. Therefore, the remnant cholesterol concentration may be an important indicator of risk stratification in patients with ischemic stroke.
The observational Copenhagen General Population Study involving 102,964 individuals suggested that a progressive increase in remnant cholesterol was associated with a progressive increase in the risk of ischemic stroke [7]. The association between the high remnant cholesterol concentration and the high risk of ischemic stroke may be related to the observation that remnant cholesterol can lead to atherosclerosis [26] and vulnerable plaque development. A previous study suggested that vulnerable carotid plaques are strongly associated with the development of ischemic stroke [27]. To further investigate the relationship between remnant cholesterol and vulnerable plaques, Matsuo et al found that the remnant cholesterol concentration, but not the LDL-C concentration, was highly correlated with the percentage of necrotic cores within vulnerable plaques in patients treated with statins [28]. Puri et al also found that the non-HDL-C concentration was strongly associated with the progression and regression of coronary atherosclerotic plaque volume, but not with LDL-C concentration [29]. These findings suggest that there may be a close relationship between the remnant cholesterol concentration and plaque characteristics (e.g., vulnerability). We also revealed a correlation between the remnant cholesterol concentration and vulnerable carotid plaques.
Our results show significantly higher remnant cholesterol concentrations in patients with IPN-rich plaques than in those without IPN, and we also found that the remnant cholesterol concentration was strongly associated with IPN enrichment. Mechanistically, remnant lipoproteins can penetrate the arterial wall and become trapped in the intima, and they may be bound and retained by the connective tissue matrix [8], leading to atherosclerosis [30]. Unlike LDL-C, remnant lipids can be taken up directly by macrophages without oxidation, leading to foam cell formation [9]. High remnant cholesterol concentrations are also associated with low inflammation [31]. Bernelot Moens et al found that elevated remnant cholesterol caused an inflammatory response in the aortic and carotid artery walls. They also reported that individuals with very high remnant cholesterol concentrations showed increased bone marrow activity, an increased number of monocytes, higher expression of integrins involved in adhesion to the arterial wall, and higher lipid accumulation in monocytes [10]. In turn, the progressive formation of IPN is closely related to the inflammatory response within the arterial wall [32]. Therefore, local infiltration of remnant cholesterol and a multilevel inflammatory response may explain the effects of remnant cholesterol on IPN in vulnerable plaques.
Previous studies have found an association between higher TG concentrations and a higher risk of ischemic stroke [33, 34]. However, as TG is readily metabolized by most cells, the exact role of TG in mediating atherosclerosis remains controversial [30]. Therefore, it is most likely that elevated TG is a marker of elevated remnant cholesterol, and it is the latter that contributes to atherosclerosis [3]. Therefore, focusing on remnant cholesterol carries greater clinical value.
LDL-C reduction is effective in preventing recurrent cardiovascular events in patients with ischemic stroke. The results of the SPARCL (Stroke Prevention by Aggressive Reduction in Cholesterol Levels) trial showed that reducing the LDL-C concentration to < 1.8 mmol/L reduced the risk of stroke recurrence by 28% [35]. However, there remains a substantial residual risk of cardiovascular events. A prospective cohort study found that remnant cholesterol remained an important marker of cardiovascular events when the LDL-C concentration was controlled [36]. Nakamura et al [36] also reported that the remnant cholesterol concentration was independently associated with the coronary atherosclerotic burden in patients with coronary heart disease and an optimal LDL-C concentration. Our study also found a strong association between the remnant cholesterol concentration and IPN in patients with ischemic stroke with an optimal LDL-C concentration. This finding supports the role of the remnant cholesterol concentration in the risk of residual atherosclerosis.
Limitations
The present study has some limitations. First, the study design was cross-sectional and retrospective; therefore, the study is limited in its ability to demonstrate a causal relationship between remnant cholesterol and carotid plaque vulnerability. We did not collect follow-up information on IPN and cardiovascular events, which limited our prospective study of the effect of baseline remnant cholesterol on vulnerable plaque progression after ischemic stroke. Therefore, future prospective cohort studies are still needed to validate our conclusion. Second, we collected lipid data only in the fasting state. Therefore, we were unable to explore the relationship between non-fasting remnant cholesterol concentrations and carotid IPN. Third, we studied the largest atherosclerotic plaque in the ipsilateral carotid artery, but no information was obtained from the other plaques. Thus, we might have missed possible vulnerable plaques that caused stroke. Fourth, our analysis examined plaques without significant acoustic shadowing on ultrasound. Thus, our findings may not be applicable to the general population with highly echogenic plaques who undergo carotid artery ultrasonography. Fifth, our study was single-center, retrospective study, and the sample size was small, with 45 patients being excluded due to lack of blood lipid panels Thus large-sample, multi-center studies are needed to validate our results. Sixth, our study did not consider other causes like arrythmias which can be a factor for embolic phenomenon even while they may have underlying plaque. Therefore, future prospective cohort studies are still needed to validate our conclusion.
Conclusions
In this study, the remnant cholesterol concentration was significantly associated with carotid IPN assessed by CEUS in patients with ischemic stroke with an optimal LDL-C concentration. Remnant cholesterol may be an important indicator of risk stratification in patients with ischemic stroke.
Acknowledgments
None to declare.
Financial Disclosure
This work was supported by the National Natural Science Foundation of China (82001838) and the Key R&D Program of Shaanxi Province (2021SF-140, 2024SF-YBXM-395).
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Patient consent for publication was obtained for the study.
Author Contributions
Yan Song and Li Tao Ruan conceived and designed the project. Yan Song and Ying Dang interpreted the results and wrote the manuscript. Ying Dang and Jun Feng collected data, collated the echocardiographic data. All authors reviewed the manuscript.
Data Availability
Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
| References | ▴Top |
- Cholesterol Treatment Trialist's Collaboration, Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681.
doi pubmed pmc - Mora S, Wenger NK, Demicco DA, Breazna A, Boekholdt SM, Arsenault BJ, Deedwania P, et al. Determinants of residual risk in secondary prevention patients treated with high- versus low-dose statin therapy: the Treating to New Targets (TNT) study. Circulation. 2012;125(16):1979-1987.
doi pubmed pmc - Lin A, Nerlekar N, Rajagopalan A, Yuvaraj J, Modi R, Mirzaee S, Munnur RK, et al. Remnant cholesterol and coronary atherosclerotic plaque burden assessed by computed tomography coronary angiography. Atherosclerosis. 2019;284:24-30.
doi pubmed - Varbo A, Nordestgaard BG. Remnant cholesterol and triglyceride-rich lipoproteins in atherosclerosis progression and cardiovascular disease. Arterioscler Thromb Vasc Biol. 2016;36(11):2133-2135.
doi pubmed - Langsted A, Madsen CM, Nordestgaard BG. Contribution of remnant cholesterol to cardiovascular risk. J Intern Med. 2020;288(1):116-127.
doi pubmed - Castaner O, Pinto X, Subirana I, Amor AJ, Ros E, Hernaez A, Martinez-Gonzalez MA, et al. Remnant cholesterol, not LDL cholesterol, is associated with incident cardiovascular disease. J Am Coll Cardiol. 2020;76(23):2712-2724.
doi pubmed - Varbo A, Nordestgaard BG. Remnant cholesterol and risk of ischemic stroke in 112,512 individuals from the general population. Ann Neurol. 2019;85(4):550-559.
doi pubmed - Nordestgaard BG, Zilversmit DB. Large lipoproteins are excluded from the arterial wall in diabetic cholesterol-fed rabbits. J Lipid Res. 1988;29(11):1491-1500.
pubmed - Goldstein JL, Ho YK, Brown MS, Innerarity TL, Mahley RW. Cholesteryl ester accumulation in macrophages resulting from receptor-mediated uptake and degradation of hypercholesterolemic canine beta-very low density lipoproteins. J Biol Chem. 1980;255(5):1839-1848.
pubmed - Bernelot Moens SJ, Verweij SL, Schnitzler JG, Stiekema LCA, Bos M, Langsted A, Kuijk C, et al. Remnant cholesterol elicits arterial wall inflammation and a multilevel cellular immune response in humans. Arterioscler Thromb Vasc Biol. 2017;37(5):969-975.
doi pubmed - Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque formation and rupture. Circ Res. 2014;114(12):1852-1866.
doi pubmed - Fazelpour S, Mulvagh SL. From cotton candy to diagnosis and monitoring of atherosclerosis: contrast-enhanced ultrasound quantification of intraplaque neovascularization. J Am Soc Echocardiogr. 2021;34(11):1195-1198.
doi pubmed - Deyama J, Nakamura T, Takishima I, Fujioka D, Kawabata K, Obata JE, Watanabe K, et al. Contrast-enhanced ultrasound imaging of carotid plaque neovascularization is useful for identifying high-risk patients with coronary artery disease. Circ J. 2013;77(6):1499-1507.
doi pubmed - Mantella LE, Colledanchise KN, Hetu MF, Feinstein SB, Abunassar J, Johri AM. Carotid intraplaque neovascularization predicts coronary artery disease and cardiovascular events. Eur Heart J Cardiovasc Imaging. 2019;20(11):1239-1247.
doi pubmed pmc - Staub D, Patel MB, Tibrewala A, Ludden D, Johnson M, Espinosa P, Coll B, et al. Vasa vasorum and plaque neovascularization on contrast-enhanced carotid ultrasound imaging correlates with cardiovascular disease and past cardiovascular events. Stroke. 2010;41(1):41-47.
doi pubmed - Camps-Renom P, Prats-Sanchez L, Casoni F, Gonzalez-de-Echavarri JM, Marrero-Gonzalez P, Castrillon I, Marin R, et al. Plaque neovascularization detected with contrast-enhanced ultrasound predicts ischaemic stroke recurrence in patients with carotid atherosclerosis. Eur J Neurol. 2020;27(5):809-816.
doi pubmed - Albers GW, Caplan LR, Easton JD, Fayad PB, Mohr JP, Saver JL, Sherman DG, et al. Transient ischemic attack—proposal for a new definition. N Engl J Med. 2002;347(21):1713-1716.
doi pubmed - Amarenco P, Bogousslavsky J, Caplan LR, Donnan GA, Hennerici MG. New approach to stroke subtyping: the A-S-C-O (phenotypic) classification of stroke. Cerebrovasc Dis. 2009;27(5):502-508.
doi pubmed - Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, Jones DW, et al. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Circulation. 2005;111(5):697-716.
doi pubmed - Lloyd B, Burrin J, Smythe P, Alberti KG. Enzymic fluorometric continuous-flow assays for blood glucose, lactate, pyruvate, alanine, glycerol, and 3-hydroxybutyrate. Clin Chem. 1978;24(10):1724-1729.
pubmed - Authors/Task Force M, Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016;253:281-344.
doi pubmed - Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N, Csiba L, et al. Mannheim carotid intima-media thickness and plaque consensus (2004-2006-2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc Dis. 2012;34(4):290-296.
doi pubmed pmc - Gray-Weale AC, Graham JC, Burnett JR, Byrne K, Lusby RJ. Carotid artery atheroma: comparison of preoperative B-mode ultrasound appearance with carotid endarterectomy specimen pathology. J Cardiovasc Surg (Torino). 1988;29(6):676-681.
pubmed - Brott TG, Halperin JL, Abbara S, Bacharach JM, Barr JD, Bush RL, Cates CU, et al. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/ SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery. Vasc Med. 2011;16(1):35-77.
doi pubmed - Song Y, Feng J, Dang Y, Zhao C, Zheng J, Ruan L. Relationship between plaque echo, thickness and neovascularization assessed by quantitative and semi-quantitative contrast-enhanced ultrasonography in different stenosis groups. Ultrasound Med Biol. 2017;43(12):2947-2953.
doi pubmed - Nordestgaard BG, Varbo A. Triglycerides and cardiovascular disease. Lancet. 2014;384(9943):626-635.
doi pubmed - Bos D, Arshi B, van den Bouwhuijsen QJA, Ikram MK, Selwaness M, Vernooij MW, Kavousi M, et al. Atherosclerotic carotid plaque composition and incident stroke and coronary events. J Am Coll Cardiol. 2021;77(11):1426-1435.
doi pubmed - Matsuo N, Matsuoka T, Onishi S, Yamamoto H, Kato A, Makino Y, Kihara S. Impact of remnant lipoprotein on coronary plaque components. J Atheroscler Thromb. 2015;22(8):783-795.
doi pubmed - Puri R, Nissen SE, Shao M, Elshazly MB, Kataoka Y, Kapadia SR, Tuzcu EM, et al. Non-HDL cholesterol and triglycerides: implications for coronary atheroma progression and clinical events. Arterioscler Thromb Vasc Biol. 2016;36(11):2220-2228.
doi pubmed - Nordestgaard BG. Triglyceride-rich lipoproteins and atherosclerotic cardiovascular disease: new insights from epidemiology, genetics, and biology. Circ Res. 2016;118(4):547-563.
doi pubmed - Varbo A, Benn M, Tybjaerg-Hansen A, Nordestgaard BG. Elevated remnant cholesterol causes both low-grade inflammation and ischemic heart disease, whereas elevated low-density lipoprotein cholesterol causes ischemic heart disease without inflammation. Circulation. 2013;128(12):1298-1309.
doi pubmed - Jaipersad AS, Lip GY, Silverman S, Shantsila E. The role of monocytes in angiogenesis and atherosclerosis. J Am Coll Cardiol. 2014;63(1):1-11.
doi pubmed - Emerging Risk Factors Collaboration, Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, Thompson A, et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302(18):1993-2000.
doi pubmed pmc - Varbo A, Nordestgaard BG, Tybjaerg-Hansen A, Schnohr P, Jensen GB, Benn M. Nonfasting triglycerides, cholesterol, and ischemic stroke in the general population. Ann Neurol. 2011;69(4):628-634.
doi pubmed - Amarenco P, Goldstein LB, Szarek M, Sillesen H, Rudolph AE, Callahan A, 3rd, Hennerici M, et al. Effects of intense low-density lipoprotein cholesterol reduction in patients with stroke or transient ischemic attack: the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial. Stroke. 2007;38(12):3198-3204.
doi pubmed - Nakamura T, Obata JE, Hirano M, Kitta Y, Fujioka D, Saito Y, Kawabata K, et al. Predictive value of remnant lipoprotein for cardiovascular events in patients with coronary artery disease after achievement of LDL-cholesterol goals. Atherosclerosis. 2011;218(1):163-167.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.