

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 15, Number 3, June 2024, pages 189-197

Selection Criteria in the Era of Perfect Competition for Drug-Eluting Stents in Association With Operator Volumes: An Operator-Volume Analysis of the Selection DES Study
Satoru Hashimotoa, b, e ![]() , Yoshihiro Motozawaa, c, d, Toshiki Manob, d
, Yoshihiro Motozawaa, c, d, Toshiki Manob, d
aDepartment of Strategic Management, TCROSS Co., Ltd., Tokyo, Japan
bChuo Graduate School of Strategic Management, Tokyo, Japan
cDepartment of Internal Medicine, San-ikukai Hospital, Tokyo, Japan
dThese authors contributed equally to this article.
eCorresponding Author: Satoru Hashimoto, Department of Strategic Management, TCROSS Co., Ltd., Shinjuku-ku, Tokyo 160-0022, Japan
Manuscript submitted April 25, 2024, accepted May 27, 2024, published online June 25, 2024
Short title: Selection Criteria for Drug-Eluting Stents
doi: https://doi.org/10.14740/cr1651
| Abstract | ▴Top |
Background: This study aimed to explore the factors influencing the drug-eluting stent (DES) selection criteria of cardiologists in association with percutaneous coronary intervention (PCI) volumes and to determine whether they value further DES improvements and modifications.
Methods: The survey was conducted on a group of cardiologist operators from April 10 to 30, 2023.
Results: The analysis included 126 operators who answered the questions. Of these, low-, intermediate-, and high-volume operators accounted for 49 (38.9%), 47 (37.3%), and 30 (23.8%), respectively. Overall, Xience™ everolimus-eluting stent (CoCr-EES) was most frequently used, with > 70% of cardiologists using it in > 20% of their PCI practice. The percentage of selection by low-, intermediate-, and high-volume operators among the DESs used demonstrated no difference, except for dual-therapy sirolimus-eluting and CD34+ antibody-coated Combo® stent (DTS). Logistic regression analysis revealed that low-volume operators are less likely to be affected in terms of company/sales representative (odds ratio (OR): 0.402, P = 0.031) and bending lesions (OR: 0.339, P = 0.037) for selecting DES. Low-volume operators less frequently selected Resolute Onyx™ zotarolimus-eluting stents (OR: 0.689, P = 0.043) and DTS (Drug-Eluting Stents) (OR: 0.361, P = 0.006) for PCI.
Conclusions: The current study results indicate that patient background, DES performance, and product specifications were not criteria for DES selection in cardiologists with different PCI volumes in routine PCI.
Keywords: Annual operator volume; Drug-eluting stent; Percutaneous coronary intervention
| Introduction | ▴Top |
Since the first drug-eluting stents (DESs) were introduced in Europe, restenosis rates, which had once been the Achilles heel of percutaneous coronary intervention (PCI), have decreased dramatically [1]. PCI indications in ischemic heart disease have expanded to include complex lesions, and the need for coronary artery bypass graft surgery has diminished [2, 3]. Subsequently, continuous evidence was reported globally, and the weakness of PCI shifted from restenosis to late stent thrombosis. Additionally, the introduction of second- and third-generation DES to overcome this problem, as well as the establishment of antiplatelet therapy, brought the incidence of postoperative events within an acceptable range [4].
Outcomes after PCI has been reported to be affected by the annual volume of PCI procedures performed and the operator in the hospital. Catheterization has affected initial outcomes due to the annual hospital volume and the volume experienced by its operators. Patients treated at low-volume hospitals have had higher in-hospital mortality rates than those treated at high-volume hospitals, and this effect has been observed in patients with acute myocardial infarction and chronic coronary disease [5, 6]. PCI is a procedure that improves with experience, and operators with more experience with the procedure have better outcomes than inexperienced operators. Today, the number of PCI cases in the United States is declining for various reasons [7-9]. Hence, the 2013 American College of Cardiology (ACC)/American Heart Association (AHA)/Society for Cardiovascular Angiography and Intervention (SCAI) clinical competency statement recommended a reduced minimum number of PCI procedures performed annually by each operator from an average of 75 to 50 cases over 2 years [10, 11].
Data extracted from the Japanese PCI Registry (J-PCI), which is a national registry of the Japanese Association of Cardiovascular Intervention and Therapeutics, demonstrated unclear associations between the annual PCI volumes performed by the operator and outcome, although low-volume hospitals have poorer in-hospital outcomes than those high-volume hospitals [12]. Approximately 250,000 cases of PCI are performed annually at approximately 1,500 hospitals in Japan, where PCI is not as centralized as in other countries, and operators at low-volume hospitals have difficulty maintaining their skills; however, the J-PCI registry data demonstrated no association between operator volume and outcome indicating the influence of device evolution, especially DES, as well as PCI technique development.
Johnson & Johnson (New Brunswick, NJ) first introduced DES in 2002, over 20 years ago [13]. The company dominated the market until 2005, after which Boston Scientific (Boston, MA), Abbott Vascular (Santa Clara, CA), Medtronic (Minneapolis, MN), and Terumo (Tokyo, Japan) entered the market, moving from monopoly to oligopoly and from oligopoly to perfect market. DES technology is believed to have reached physical limitations although competing companies have improved their DESs under regulatory approval. However, companies competing in the DES market continue to make slight improvements to their products, each time using the improvements as a sales advantage to promote the strengths of their products to healthcare professionals. Therefore, DES has become a commodity and is considered in a price competition 20 years after its launch.
The current study, an operator-volume analysis of the Selection DES study, aimed to explore 1) the proportions; 2) factors influencing the DES selection criteria of operators in terms of PCI volumes (low-, medium-, and high-volumes); and 3) to determine if operators require and value further DES improvements and modifications.
| Materials and Methods | ▴Top |
Study population
The main analysis of the study focusing more on patient characteristics and lesion factors has already been reported in a previous publication titled the Selection DES study [14]. In berief, the survey was conducted on all Japanese cardiologist members of TCROSS NEWS who agreed to receive the e-newsletter. TCROSS NEWS is a highly specialized website that was launched in January 2010. The details of TCROSS NEWS’ survey panel have been described elsewhere [15, 16].
Data collection
Questions consisting of 14 categories were filled out on Google Forms. The survey included 43 items regarding 1) the responder’s background; 2) the hospital status; and 3) the criteria for selecting DES(s). Responder’s background (seven items) includes hospital type, age distribution, PCI volume either in a hospital or by the operator, and years of PCI experience. The operator volume at the hospital was divided into tertiles, for this study, following the ACC/AHA/SCAI clinical competence statement [11], from low-volume operators (< 50 PCIs per year) to intermediate-volume operators (50 - 100 PCIs per year) to high-volume operators (> 100 PCIs per year). Hospital status (three items) includes the position in the hospital, selection criteria, and individual right to select DESs. Details of selecting devices (32 items) include device selection criteria, device use rate for each DES, expectations from a DES company, selection criteria by lesion background, and selection criteria by patient background.
Statistics analysis
Descriptive statistics were calculated for each survey item. The Chi-square test for discrete variables was used to compare low-, intermediate-, and high-volume operators, standard statistical methods. The proportion of DES use in the operator practice was classified into low (< 5%), medium (5-20%), and high (> 20%) following each DES included in the study, and the difference between the annual PCI volume performed by operators and DES proportion used in their practice were examined. Multivariate logistic regression analysis estimated the odds ratio (OR) and 95% confidence intervals (CIs) assessing the factors that affect DES selection criteria. The logistic regression analysis classified each operator group, either the low-, intermediate-, or high-volume, into dichotomous categories (0 or 1). Each operator group was used as the dependent variable, with 32 items of details of device selection criteria serving as independent variables for analysis. Significance was accepted at P values of < 0.05 in all analyses. IBM Statistical Package for the Social Sciences Statistics Version 28.0 was used for statistical analysis.
Types of DES
Abbott’s Xience™ cobalt chromium everolimus-eluting stent (CoCr-EES), Boston Scientific’s Synergy™ platinum chromium everolimus-eluting stent (PtCr-EES), Medtronic’s Resolute Onyx™ zotarolimus-eluting stent (ZES), Terumo’s Ultimaster™ sirolimus-eluting stent with bioresorbable polymer (BP-SES), Biosensors’s BioFreedom™ biolimus-coated stent (BCS), B.Braun’s Coroflex® ISAR Neo sirolimus-eluting stent (UPF-SES), and OrbusNeich’s dual-therapy sirolimus-eluting and CD34+ antibody-coated Combo® stent (DTS) were the DES types available in Japan that the present study investigated.
Ethical considerations
To avoid the identification of individuals, this study was conducted through an anonymous survey, and the data obtained were statistically processed. The responses were not used for any purpose other than this survey, and no third-party access to the survey was provided. The participants were informed that the responses would not affect the individual’s institutional affiliation. Submission of the web-based questionnaire was considered as providing informed consent. This was clearly written in the survey form and was in accordance with the requirements of the Ethics Committee of TCROSS Co., Ltd. All authors had access to information that could identify individual participants during or after data collection. Those terms and conditions were included in the survey form in accordance with the instructions of the Ethics Committee. The study complies with the principles and requirements of the Declaration of Helsinki and was conducted following the approval of the Ethics Committee (January 23, 2023, approval number: 2023001).
| Results | ▴Top |
Participant demographics
The survey was conducted among all cardiologist members of TCROSS NEWS who agreed to receive the e-newsletter from April 10, 2023, to April 30, 2023. Overall, 126 who responded were included in the analysis. Table 1 shows the details of the study participants. Of these, low-, intermediate-, and high-volume operators accounted for 49 (38.9%), 47 (37.3%), and 30 (23.8%), respectively. Age, PCI procedure history, position in the hospital, or device selection rights were not different among the three groups.
 Click to view | Table 1. Backgrounds of the Study Participant |
A higher percentage of low-volume and high-volume operators worked in public and private general-city hospitals, respectively. The percentage of low-volume operators working in cardiovascular hospitals was lower than that of intermediate- and high-volume operators. Over 80% of intermediate- and high-volume operators recorded > 200 PCI cases in the annual hospital volume, while low-volume operators accounted for approximately 60% of the hospital volume of < 200 PCI cases. The highest percentage of emergency/urgent PCI procedures (> 200 per year) were performed at hospitals with high-volume operators. Conversely, the percentage of emergency/urgent PCIs of 21 - 50 cases per year was higher at hospitals with low-volume operators.
The selection criteria for DESs
The study divided the percentage of each DES into three categories: low- (< 5% of the cases), medium- (5-20%), and high-volume (> 20%), and the association with the low-, intermediate-, and high-volume operators were examined in Table 2. Overall, CoCr-EES was used most frequently, with > 70% of operators using CoCr-EES in > 20% of their cases, followed by PtCr-EES, BP-SES, and ZES used by a higher percentage of operators in 38.9%, 31.7%, and 23.8% of cases on average, respectively. The percentage of selection by low-, intermediate-, and high-volume operators among the DESs used demonstrated no difference, except for DTS. The percentage of low-volume operators choosing DTS for > 5% of their PCIs was 4.1%, while for intermediate- and high-volume operators, the percentages choosing DTS were higher in 21.3% (12.8 + 8.5%) and 30% (26.7 + 3.3%), respectively. The main results of Table 2 were clearly illustrated in Figure 1.
Click to view | Table 2. The Use of Drug-Eluting Stent Rate in Relation to the Operator Volume |
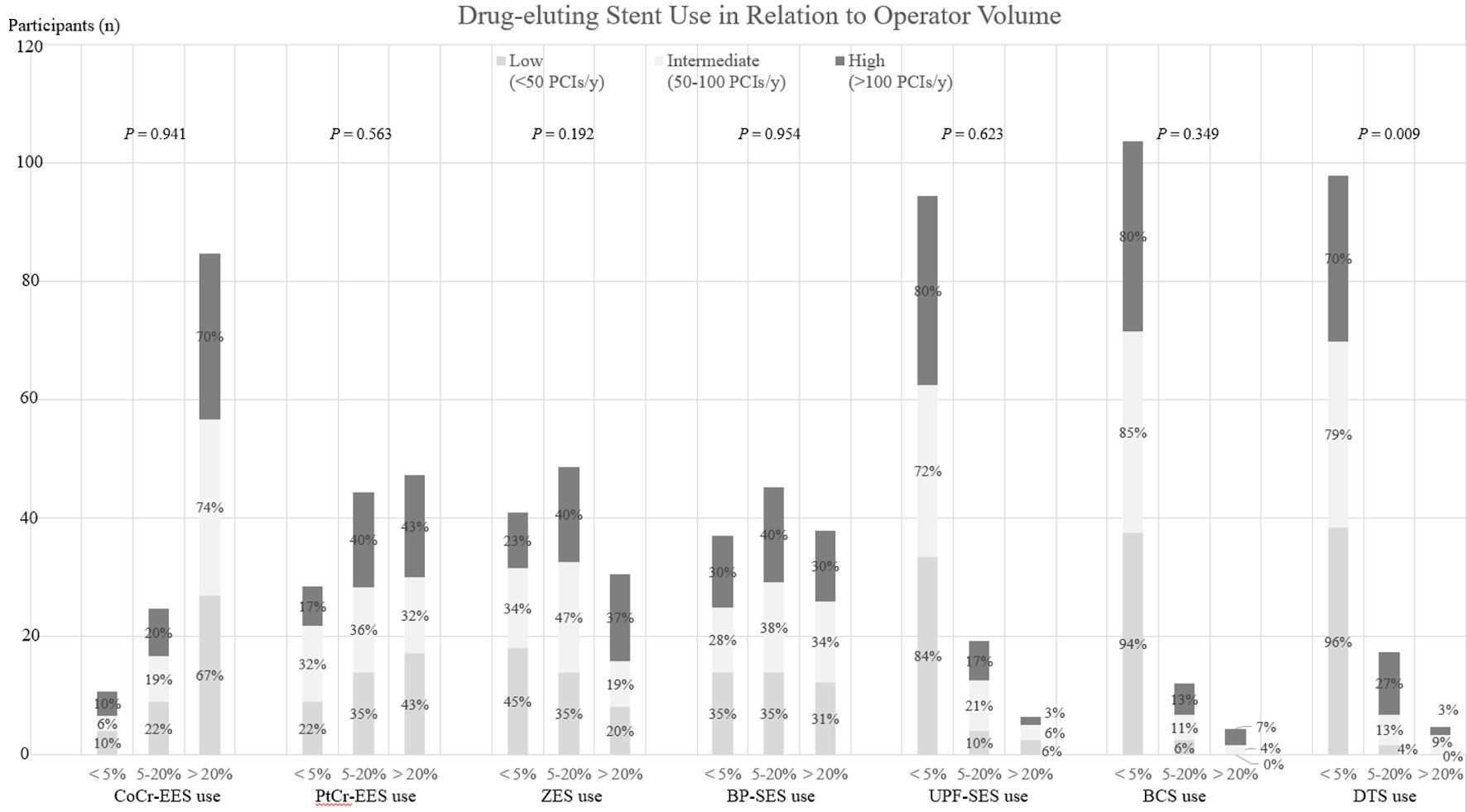 Click for large image | Figure 1. The main results of Table 2. This figure represents the current drug-eluting stent market share in Japan where CoCr-EES was selected by more than 70% of respondents in different operator volumes in > 20% of their percutaneous coronary intervention (PCI) procedures. On the other hand, UPF-SES, BCS, and DTS were less likely to be selected, indicating that more than 70% of respondents select < 5% of these in their procedures. The percentage of selection by low-, intermediate-, and high-volume operators among the DESs used demonstrated no difference, except for DTS. CoCr-EES: Abbott’s Xience™ cobalt chromium everolimus-eluting stent; PtCr-EES: Boston Scientific’s Synergy™ platinum chromium everolimus-eluting stent; ZES: Medtronic’s Resolute Onyx™ zotarolimus-eluting stent; BP-SES: Terumo’s Ultimaster™ sirolimus-eluting stent with bioresorbable polymer; BCS: Biosensors’s BioFreedom™ biolimus-coated stent; UPF-SES: B.antibody-coated Combo® ISAR Neo sirolimus-eluting stent; DTS: OrbusNeich’s dual-therapy sirolimus-eluting and CD34+ antibody-coated Combo® stent. |
Factors affecting the DES selection
Logistic regression analysis was performed for each group of low-, intermediate-, and high-volume operators in terms of factors affecting DES selection. Results revealed that low-volume operators are less likely to be affected by the company/sales representative (OR: 0.402, 95% CI: 0.175 - 0.922, P = 0.031) and bending lesions (OR: 0.339, 95%CI: 0.123 - 0.938, P = 0.037) in selecting DESs. ZES (OR: 0.689, 95% CI: 0.48 - 0.989, P = 0.043) and DTS (OR: 0.361, 95% CI: 0.175 - 0.744, P = 0.006) were less likely to be selected by low-volume operators (Table 3). Intermediate-volume operators used PtCr-EES (OR: 0.733, 95% CI: 0.543 - 0.991, P = 0.044) less frequently in their practice but demonstrated an increased use of DTS (OR: 1.64, 95% CI: 1.026 - 2.507, P = 0. 038) as shown in Table 3. High-volume operators used ZES more frequently (OR: 1.768, 95% CI: 1.131 - 2.766, P = 0.012), whereas UPF-SES usage decreased inversely (OR: 0.437, 95% CI: 0.205 - 0.931, P = 0.032).
Click to view | Table 3. Internal and External Factors that Affect the Different Operator Volume |
| Discussion | ▴Top |
The present study revealed that the PCI volume by the operator did not affect the proportion of an individual DES use (low- (< 5% use), medium- (5-20% use), or high- (> 20% use) ), except for DTS as shown in Table 2. Additionally, the DES selection criteria were less related to patient background, DES performance, and sales and marketing activities, regardless of the operator’s annual volume. Conversely, the influence of bending lesions on DES selection criteria was less pronounced only for low-volume operators, and low-volume operators were less likely to select DES based upon the relationship with the company or sales representative.
Differences in the annual volume and perceptions among operators
Major manufacturers began to focus on evolving bare-metal stents and fundamentally rethinking the mechanisms of restenosis to overcome restenosis, which had been considered the greatest limitation of PCI. The idea was to use the stent as a vehicle to deliver the maximum tolerated dose of anti-restenotic agent to terminate the cascade locally because restenosis is caused by an immune reaction in vivo. Immunosuppressive agents, antiplatelet agents, growth inhibitors, and endothelial healing agents were candidates because anti-restenosis agents, and among these, limus-based immunosuppressive agents, such as sirolimus and everolimus, were the primary focus from the perspective of efficacy and safety for DES used for coronary artery stenosis [17]. Stent thrombosis emerged as a new issue and reportedly involved polymers that release drugs from the stent, which causes the development or introduction of biocompatible polymers by the suppliers, thereby leading to acceptable thrombosis levels. Manufactures have focused their development efforts on improving delivery performance as DESs are now being implanted for more complex lesions. In particular, superior delivery performance is required for bending lesions, and differences have been compared in bench tests [18].
The present study revealed that bending lesions had less influence on DES selection in the low-volume operators. Conversely, the DES selection was more likely to be affected by bending lesions in intermediate- and high-volume operators, although the effect was not statistically significant. Despite not reaching significance, 22.4% of low-volume operators had < 5 years of experience with PCI, compared to intermediate- (4.3%) and high-volume operators (10.0%), indicating that differences in PCI perception for complex lesions with severe bending may have affected the results. The hospital performing the PCI has an experienced supervising operator who performs PCI on complex lesions, such as bending lesions. Younger operators begin with simple lesions to gain experience and then move on to complex lesions with bending lesions under the observation of a supervising operator. The difference in perception may be seen in the discrepancy between the views of lower-volume younger operators and intermediate- and high-volume operators in the present study.
Impact of differences in DES structure
The present study revealed a higher rate of selection by intermediate- and high-volume operators than did the low-volume operators in DTS. DTS differs from other DESs in structure, with three components of a DES, including platform, drug, and polymer, plus anti-CD34 + antibody inner surface of the stent. The structure has more easily facilitated stent endothelialization than other DES [19]. The performance and outcomes have not been differentiated from standard DES, as no efficacy or safety results were demonstrated for post-procedure or late outcomes compared to other DESs, despite the distinctive characteristics [20, 21]. A lower percentage (4.1%) of low-volume operators used DTS in > 5% of their cases due to the less importance of company and sales relationships in the DES selection criteria of low-volume operators (OR: 0.402, P = 0.031). Conversely, the proportion of intermediate- and high-volume operators using DTS in > 5% of cases was 21.3% and 30%, respectively, indicating other reasons beyond performance and evidence for this DES selection criterion. A similar trend was observed for intermediate- and high-volume operators, and logistic regression results confirmed that DES itself, rather than patient or lesion background, influenced the choice of the operator in each group (Tables 3).
Limitations
The present study has some limitations. First, the study is the result of a survey of cardiologists, and the accuracy of the data is dependent on the respondents since the responses generated data from self-reported results. Second, business practices and other factors are unique to the Japanese market, thus adaptation to other markets must be considered based on the current situation in the target country. Third, further research is required to conclude the results are representative of an entire population since the sample size was limited to 126 participants.
Conclusions
The current study results indicate that in routine PCI, patient background, lesion characteristics, DES performance, and DES specifications were not criteria for DES selection in operators with different annual PCI volumes. Therefore, the development of DES has already reached its physical limitations and has become commoditized, with results that challenge the need for further improvement and modification of the DES.
Acknowledgments
The authors would like to thank Ms. Keiko Takahashi for her help in the preparation of the figures and tables, Ms. Rie Arai for her research assistance.
Financial Disclosure
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained.
Author Contributions
S. Hashimoto made a concept, research, design, statistical analysis, and drafted the article. Y. Motozawa contributed for collection and interpretation of data. T. Mano was responsible for the final approval of the article to be submitted.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
ACC: American College of Cardiology; AHA: American Heart Association; BCS: Biosensors’s BioFreedom™ biolimus-coated stent; BP-SES: Terumo’s Ultimaster™ sirolimus-eluting stent with bioresorbable polymer; CoCr-EES: Abbott’s Xience™ cobalt chromium everolimus-eluting stent; CI: confidence interval; DES: drug-eluting stent; DTS: OrbusNeich’s dual-therapy sirolimus-eluting and CD34+ antibody-coated Combo® stent; J-PCI: Japanese PCI Registry; OR: odds ratio; PCI: percutaneous coronary intervention; PtCr-EES: Boston Scientific’s Synergy™ platinum chromium everolimus-eluting stent; SCAI: Society for Cardiovascular Angiography and Intervention; UPF-SES: B.Braun’s Coroflex® ISAR Neo sirolimus-eluting stent; ZES: Medtronic’s Resolute Onyx™ zotarolimus-eluting stent
| References | ▴Top |
- Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Perin M, Colombo A, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346(23):1773-1780.
doi pubmed - Park DW, Yun SC, Lee SW, Kim YH, Lee CW, Hong MK, Kim JJ, et al. Long-term mortality after percutaneous coronary intervention with drug-eluting stent implantation versus coronary artery bypass surgery for the treatment of multivessel coronary artery disease. Circulation. 2008;117(16):2079-2086.
doi pubmed - Hannan EL, Wu C, Walford G, Culliford AT, Gold JP, Smith CR, Higgins RS, et al. Drug-eluting stents vs. coronary-artery bypass grafting in multivessel coronary disease. N Engl J Med. 2008;358(4):331-341.
doi pubmed - Navarese EP, Andreotti F, Schulze V, Kolodziejczak M, Buffon A, Brouwer M, Costa F, et al. Optimal duration of dual antiplatelet therapy after percutaneous coronary intervention with drug eluting stents: meta-analysis of randomised controlled trials. BMJ. 2015;350:h1618.
doi pubmed pmc - Fanaroff AC, Zakroysky P, Dai D, Wojdyla D, Sherwood MW, Roe MT, Wang TY, et al. Outcomes of PCI in relation to procedural characteristics and operator volumes in the United States. J Am Coll Cardiol. 2017;69(24):2913-2924.
doi pubmed pmc - McGrath PD, Wennberg DE, Dickens JD, Jr., Siewers AE, Lucas FL, Malenka DJ, Kellett MA, Jr., et al. Relation between operator and hospital volume and outcomes following percutaneous coronary interventions in the era of the coronary stent. JAMA. 2000;284(24):3139-3144.
doi pubmed - Howard DH, Shen YC. Trends in PCI volume after negative results from the COURAGE trial. Health Serv Res. 2014;49(1):153-170.
doi pubmed pmc - Maroney J, Khan S, Powell W, Klein LW. Current operator volumes of invasive coronary procedures in Medicare patients: implications for future manpower needs in the catheterization laboratory. Catheter Cardiovasc Interv. 2013;81(1):34-39.
doi pubmed - Kim LK, Feldman DN, Swaminathan RV, Minutello RM, Chanin J, Yang DC, Lee MK, et al. Rate of percutaneous coronary intervention for the management of acute coronary syndromes and stable coronary artery disease in the United States (2007 to 2011). Am J Cardiol. 2014;114(7):1003-1010.
doi pubmed - Harold JG, Bass TA, Bashore TM, Brindis RG, Brush JE, Jr., Burke JA, Dehmer GJ, et al. ACCF/AHA/SCAI 2013 update of the clinical competence statement on coronary artery interventional procedures: a report of the American College of Cardiology Foundation/American Heart Association/American College of Physicians Task Force on Clinical Competence and Training (Writing Committee to Revise the 2007 Clinical Competence Statement on Cardiac Interventional Procedures). J Am Coll Cardiol. 2013;62(4):357-396.
doi pubmed - Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58(24):e44-122.
doi pubmed - Inohara T, Kohsaka S, Yamaji K, Amano T, Fujii K, Oda H, Uemura S, et al. Impact of institutional and operator volume on short-term outcomes of percutaneous coronary intervention: a report from the Japanese nationwide registry. JACC Cardiovasc Interv. 2017;10(9):918-927.
doi pubmed - Cordis. European cypher stent launch showing mixed initial results. Pharma Intelligence. July 22, 2022 [cited April 25, 2023]. Available from: https://invivo.pharmaintelligence.informa.com/MT016889/Cordis-European-Cypher-Stent-Launch-Showing-Mixed-Initial-Results.
- Hashimoto S, Motozawa Y, Mano T. Selection criteria in the era of perfect competition for drug-eluting stents - a survey of interventional cardiologists in Japan: the selection-DES study. Expert Rev Med Devices. 2023;20(12):1235-1242.
doi pubmed - Hashimoto S, Motozawa Y, Mano T. Effect of the Japanese medical office system on job satisfaction, loyalty, engagement, and organizational commitment of medical practitioners: a survey of cardiologists in the acute care setting. BMC Health Serv Res. 2024;24(1):139.
doi pubmed pmc - Hashimoto S, Motozawa Y, Mano T. Effects of the Japanese medical office system on the creation of innovation among medical doctors: a survey of cardiologists in the acute care setting. Int J Healthc Manag. 2024.
doi - Yamaguchi T, Tamura T, Ako J, Kozuma K, Tanabe K, Morino Y. Drug-eluting stent. Tokyo: Igaku-shoin Ltd. 2004.
- Schmidt W, Lanzer P, Behrens P, Topoleski LD, Schmitz KP. A comparison of the mechanical performance characteristics of seven drug-eluting stent systems. Catheter Cardiovasc Interv. 2009;73(3):350-360.
doi pubmed - Kalkman DN, Chandrasekhar J, de Winter RJ, Mehran R. Current evidence for the safety and efficacy of the bio-engineered dual therapy COMBO stent. Minerva Cardioangiol. 2018;66(3):262-272.
doi pubmed - Jaguszewski M, Aloysius R, Wang W, Bezerra HG, Hill J, De Winter RJ, Karjalainen PP, et al. The REMEDEE-OCT study: an evaluation of the bioengineered COMBO dual-therapy CD34 antibody-covered sirolimus-eluting coronary stent compared with a cobalt-chromium everolimus-eluting stent in patients with acute coronary syndromes: insights from optical coherence tomography imaging analysis. JACC Cardiovasc Interv. 2017;10(5):489-499.
doi pubmed - Jakobsen L, Christiansen EH, Freeman P, Kahlert J, Veien K, Maeng M, Raungaard B, et al. Impact of diabetes on clinical outcomes after revascularization with the dual therapy CD34 antibody-covered sirolimus-eluting Combo stent and the sirolimus-eluting Orsiro stent. Catheter Cardiovasc Interv. 2022;99(7):1965-1975.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.