

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Original Article
Volume 5, Number 6, December 2014, pages 163-170
Clinical Long-Term Response to Cardiac Resynchronization Therapy Is Independent of Persisting Echocardiographic Markers of Dyssynchrony
Barbara Naegelia, c, Hans-Peter Brunner-La Roccab, Christine Attenhofer Josta, Anja Fah-Gunza, Dominik Maurera, Osmund Bertela, Christoph Scharfa
aHerzGefassZentrum, Klinik Im Park, Seestrasse 247, CH-8027 Zurich, Switzerland
bDepartment of Cardiology, Maastricht University Medical Centre, PO Box 5800, NL-6202 AZ Maastricht, The Netherlands
cCorresponding Author: Barbara Naegeli, HerzGefassZentrum, Klinik Im Park, Seestrasse 247, CH-8027 Zurich, Switzerland
Manuscript accepted for publication December 12, 2014
Short title: Dyssynchrony After CRT
doi: https://doi.org/10.14740/cr368w
| Abstract | ▴Top |
Background: The aim of the study was to prove the concept that correction of established parameters of dyssynchrony is a requirement for favorable long-term outcome in patients with cardiac resynchronization therapy (CRT), whereas patients with persisting dyssynchrony should have a less favorable response.
Methods: After CRT implantation and optimization of dyssynchrony parameters, we evaluated whether correction or persistence of dyssynchrony predicted long-term outcome. Primary endpoint was a combination of cardiac mortality/heart transplantation and hospitalization due to worsening heart failure, and secondary endpoint was NYHA class.
Results: One hundred twenty-eight consecutive patients (mean age 68 ± 10 years) undergoing CRT with a mean left ventricular ejection fraction of 27±9% were followed for 27 ± 19 months. All cause mortality was 17.2%, cardiac mortality was 7.8% and 3.1% had to undergo heart transplantation. Rehospitalization due to worsening heart failure was observed in 14.8%. NYHA class before CRT implantation was 2.8 ± 0.8 and improved during follow-up to 2.0 ± 0.8 (P < 0.001). A clinical response was observed in 76% (n = 97) and an echocardiographic response was documented in 66% (n = 85). After individually optimized AV and VV intervals with echocardiography, atrioventricular dyssynchrony was still present in 7.2%, interventricular dyssynchrony in 13.3% and intraventricular dyssynchrony in 16.4%. Despite persistent atrioventricular, interventricular and intraventricular dyssynchrony at long-term follow-up, the combined primary and secondary endpoints did not differ compared to the group without mechanical dyssynchrony (P = ns). QRS duration with biventricular stimulation did not differ between responders vs. nonresponders.
Conclusion: After successful CRT implantation, clinical long-term response is independent of correction of dyssynchrony measured by echocardiographic parameters and QRS width.
Keywords: Heart failure; Cardiac resynchronization therapy; Echocardiography; Doppler; Dyssynchrony; Outcome
| Introduction | ▴Top |
Cardiac resynchronization therapy (CRT) has been successfully introduced into treatment of heart failure patients based on the concept that electromechanical abnormalities resulting from abnormal ventricular activation can be corrected by biventricular stimulation [1-4]. Whereas this therapy improved quality of life and functional status, reduced heart failure hospitalizations and prolonged survival in certain subsets of patients with prolonged QRS duration and reduced left ventricular ejection fraction (LVEF) [5-7], studies in other subgroups with moderate prolonged QRS duration and echocardiographic dyssynchrony were disappointing [8-10].
Even in patients with class I indications for CRT at least 30% do not respond to resynchronization therapy [6, 7]. We therefore studied whether long-term treatment effects are according to the intial concept dependent of correction of established echocardiographic and electrocardiographic parameters of dyssynchrony.
| Methods | ▴Top |
Patient population
All consecutive patients with successfully implanted CRT-P or CRT-D devices at our clinic as part of their clinical management in line with the current guidelines (LVEF ≤ 35%, QRS duration ≥ 120 ms, NYHA class II-IV despite optimal medical therapy) were recruited prospectively [11]. Both ischemic and non-ischemic cardiomyopathies were included. Medical therapy consisted of angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, beta-blockers, diuretics and aldosterone antagonists as clinically tolerated and as deemed appropriate by the physician in charge.
Study endpoints
Primary endpoint was definded as a combination of cardiovascular mortality/heart transplantation and/or hospitalization of worsening heart failure, and secondary endpoint was the change in NYHA class. Primary endpoint adjudication was performed by two experienced heart failure specialists blinded to echocardiographic and other follow-up data.
A clinical response to CRT was predefined as two of the following three criteria: decrease of NYHA class by at least 1 point, freedom of cardiac death within 6 months and freedom of rehospitalization for decompensated heart failure within 6 months. An echocardiographic response was predefined as an absolute increase in LVEF of ≥ 5% and/or a reduction of left ventricular end-systolic volume (LVESV) > 15% [12, 13].
Echocardiographic acquisition
A complete standard transthoracic echocardiographic examination (Vivid 7, General Electric Medical Systems, Horton, Norway) was performed before device implantation. After successful CRT implantation, ventricular dyssynchrony was assessed with established echocardiographic techniques and tissue Doppler imaging (TDI) [12-15]. For each acquisition, three heart cycles were recorded. Doppler myocardial imaging velocity data were acquired using a narrow sector and optimal depth of imaging. The velocity range setting was adjusted in order to avoid aliasing.
Atrioventricular dyssynchrony was assessed by determining left ventricular filling time (LVFT), corrected for variations in different R-R intervals. A corrected LVFT of < 40% was used to indicate atrioventricular dyssynchrony [4]. Interventricular dyssynchrony was defined as an interventricular mechanical delay (IVMD) of > 40 ms and/or by a left ventricular preejection period (LVPEP) of > 140 ms [4]. Intraventricular dyssynchrony was defined as a septal-to-posterior wall motion delay (SPWMD) of ≥ 130 ms, and/or by a delayed activation of the lateral wall (DALW), which was calculated as a percentage of overlap between the end of lateral wall contraction on M-mode echocardiography and the onset of left ventricular filling [4, 6, 16].
The above mentioned parameters were collected in each patient to assess or exclude baseline ventricular dyssynchrony after device implantation (with nominal settings of the device). In patients with persistent ventricular dyssynchrony, individual optimization of atrioventricular (AV) and interventricular (VV) intervals was performed 1 month after device implantation by experienced echocardiographers in our heart failure clinic. Thus, AV interval optimization was done in over 90% with the iterative method, in the remaining patients with the simplified mitral inflow method or with the aortic velocity-time integral (VTI) or with the mitral inflow VTI method [17-19]. VV interval optimization was achieved by programming the settings in a way that would result in least VV mechanical delays (as measured by difference in pulmonary and aortic preejection intervals by pulsed-wave Doppler).
Electrocardiographic measurements
Electrical conduction delays were measured on 12 lead electrocardiogram as QRS duration without biventricular stimulation and in biventricular paced rhythm, respectively.
Study protocol
During long-term follow-up, all patients underwent clinical evaluation (NYHA class) and device interrogation before discharge, at 1, 3, 6 and 12 months, thereafter every 6 months. Under stable conditions, routine echocardiographic evaluation was performed every 6 months.
The study protocol was approved by the local ethical committee and all patients gave informed consent to participate in the study.
Statistical methods
Categorical variables are presented as frequencies and percentages and compared between periods using the χ2 test. Continuous variables are presented as means ± standard deviation or medians with interquartile range (IQR) as appropriate and compared using Student’s t-test or Mann-Whitney U test as appropriate. Repeated measures were tested using paired t-test or Wilcoxon test as appropriate. All analyses were conducted using commercially available statistical software (SPSS version 18.0, SPSS Inc, Chicago, IL, USA). All P values are two-sided and considered statistically significant if ≤ 0.05.
| Results | ▴Top |
A total of 128 consecutive patients (mean age 68 ± 10 years, 71% males) with successfully implanted CRT devices were included. One hundred fourteen (89%) were in sinusrhythm, 14 (11%) had permanent atrial fibrillation, and nine patients (7%) had an implanted pacemaker or ICD device prior to CRT implantation. Baseline charactersistics are shown in Table 1.
 Click to view | Table 1. Baseline Characteristics of the Included Population (n = 128) |
After a mean follow-up of 27 ± 19 months (range 2 - 98 months), all cause mortality was 17.2% (n = 22), cardiac mortality was 7.8% (n = 10) (eight low output and two sudden cardiac death) and 9.4% patients (n = 12) suffered a non-cardiac death (three cancer, four septicemia, two gastrointestinal bleeding, one cerebral hemorrage and two suicide). Four patients (3.1%) had to undergo heart transplantation (HTPL). The rehospitalization rate because of decompensated heart failure was 14.8% (n = 19).
In the entire group, functional NYHA class before CRT implantation was 2.8 ± 0.8 and improved during follow-up to 2.0 ± 0.8, LVEF increased from 27±9% to 37±13%, whereas left ventricular end-diastolic diameter (LVEDD) decreased from 6.7 ± 0.9 cm to 6.2 ± 1.0 cm and left ventricular end-systolic diameter (LVESD) decreased from 5.6 ± 1.1 cm to 5.0 ± 1.2 cm (all P < 0.001). NYHA class improved at least by 1 point in 57.8% (Table 2).
Click to view | Table 2. Clinical and Echocardiographic Response After CRT Implantation in the Entire Group, n = 128 (%) |
Despite individual optimization of the AV and VV interval with echocardiography, atrioventricular dyssynchrony was still present in 7.2% (excluding 14 patients with permanent atrial fibrillation), interventricular dyssynchrony could be documented in 13.3% and intraventricular dyssynchrony was observed in 16.4%.
At follow-up echocardiography, the combined primary and secondary endpoint did not differ between the groups with persistent or completely corrected atrioventricular dyssynchrony: cardiac mortality/heart transplantation and the frequency of rehospitalization due to progressive heart failure was equally distributed, and there was no difference in the distribution of functional NYHA classes between patients with and without atrioventricular dyssynchrony (Fig. 1). Likewise were the findings for persistent or absent interventricular dyssynchrony (Fig. 2) and for persistent or absent intraventricular dyssynchrony (Fig. 3).
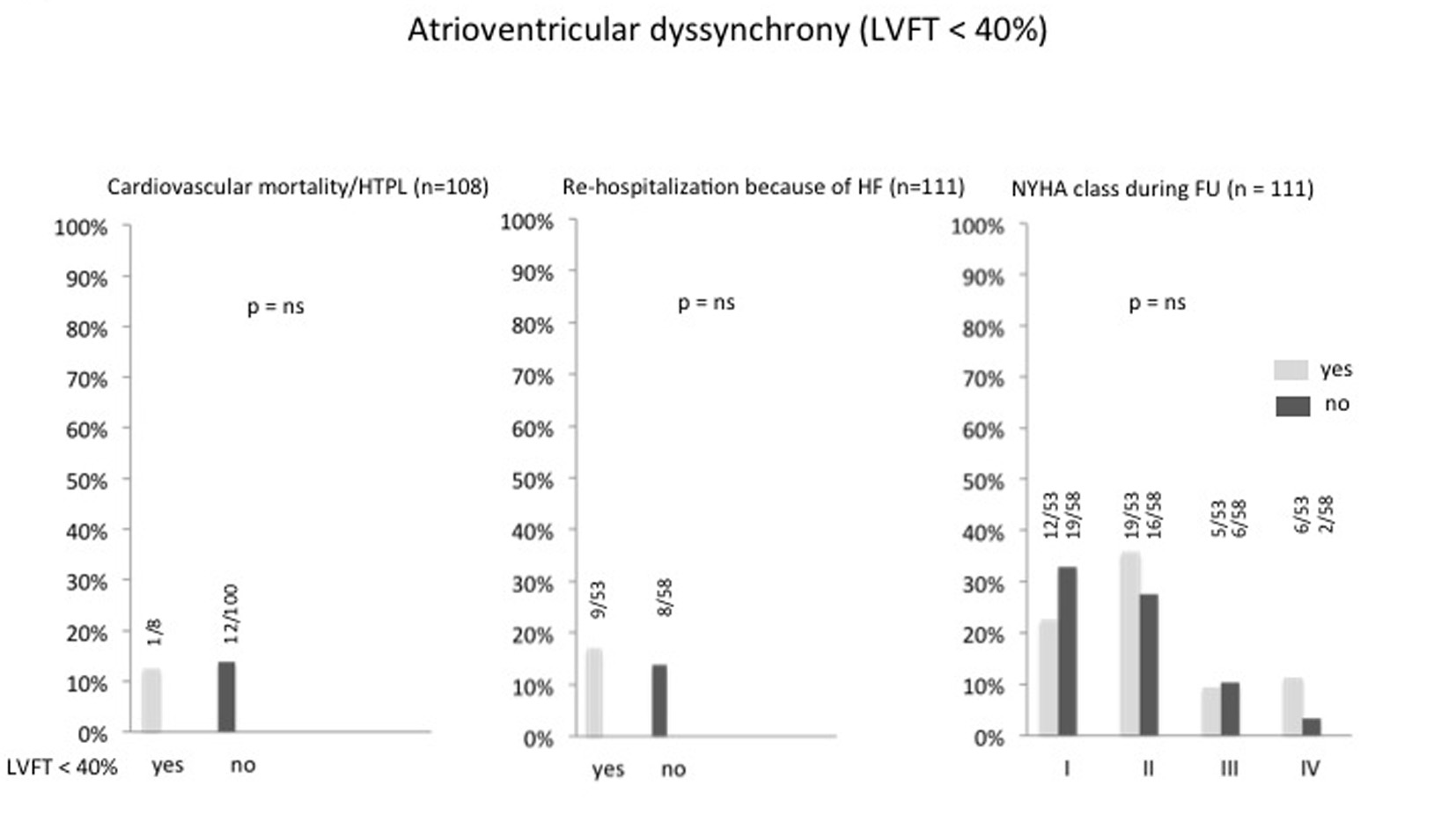 Click for large image | Figure 1. Percentage of atrioventricular dyssynchrony after optimizing the AV and VV intervals and its correlation to cardiac mortality/heart transplantation, re-hospitalization because of heart failure and NYHA class. HTPL: heart transplantation; HF: heart failure; LVFT: left ventricular filling time; FU: follow-up. |
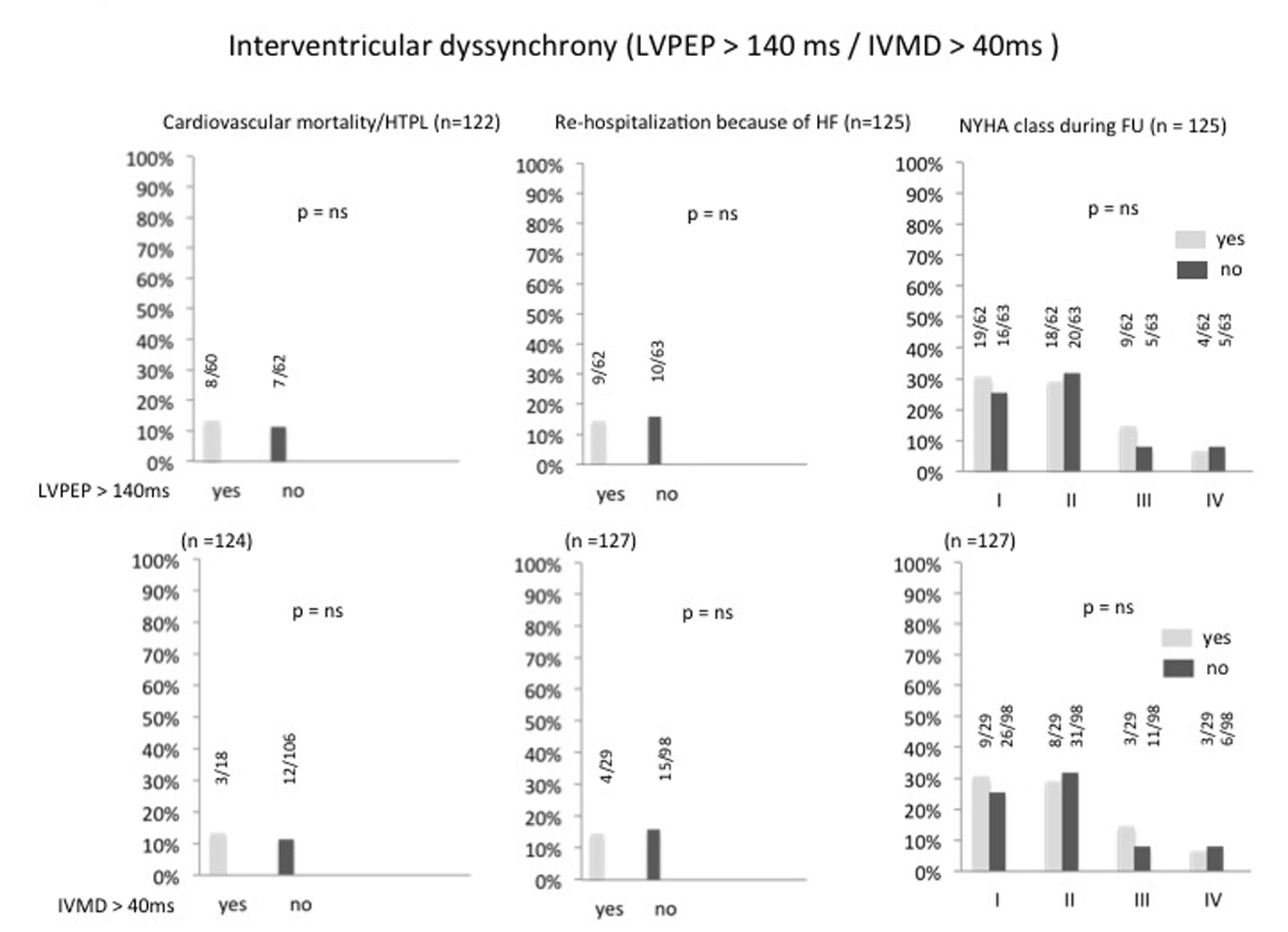 Click for large image | Figure 2. Percentage of interventricular dyssynchrony after optimizing the AV and VV intervals and its correlation to cardiac mortality/heart transplantation, re-hospitalization because of heart failure and NYHA class. HTPL: heart transplantation; HF: heart failure; LVPEP: left ventricular preejection period; IVMD: interventricular mechanical delay; FU: follow-up. |
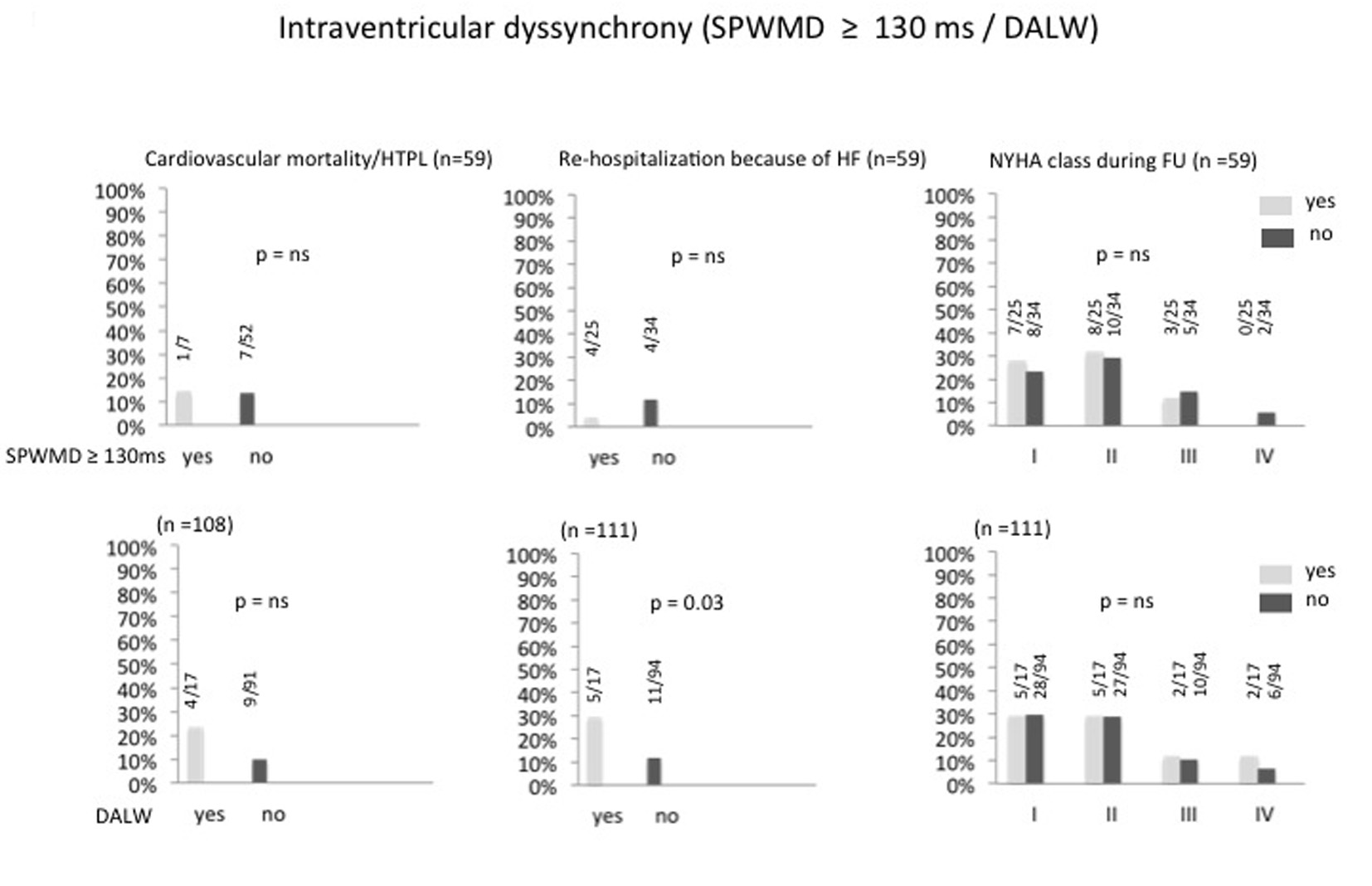 Click for large image | Figure 3. Percentage of intraventricular dyssynchrony after optimizing the AV and VV intervals and its correlation to cardiac mortality/heart transplantation, re-hospitalization because of heart failure and NYHA class. HTPL: heart transplantation; HF: heart failure; SPWMD: septal to posterior wall motion delay; DALW: delayed activation of the lateral wall; FU: follow-up. |
Various clinical as well as echocardiographic parameters during follow-up were indicators of a poor outcome. Table 3 shows the difference in these parameters in patients with and without the combined endpoint of cardiac death and HTPL. However, none of the numerical echocardiographic dyssynchrony parameters were related to outcome and QRS duration after successful device implantation was also not predictive for outcome.
Click to view | Table 3. Clinical, Echocardiographic and Electrocardiographic Characteristics Comparing Patients With and Without Cardiac Death or HTPL |
| Discussion | ▴Top |
Our study confirms that the clinical response with biventricular pacing was independent of successful or unsuccessful correction of established echocardiographic parameters of atrioventricular, interventricular and intraventricular dyssynchrony and was not related to shortening of QRS duration. Since the effects of CRT develop over several months and are thought to be due to ventricular reverse-remodeling, long-term follow-up is necessary to examine the relation between dyssynchrony and clinical response. The extended long-term observations in our study (2.3 years) are in accordance with the results of several other trials with shorter follow-up periods of 6 months to 1 year [20-23]. Given these results of clinical response being not related to established echocardiographic parameters of dyssynchrony, it is not surprising that virtually all trials failed which tried to improve clinical response by optimizing parameters of dyssynchrony either by modulation of AV or VV delays [20-23].
Equally prospective definition of responders vs. nonresponders using these echocardiographic parameters of dyssynchrony before device implantation failed, and only left bundle branch block as a reason for electrical conduction delay, clinical history and severly depressed LVEF remained powerful predictors of a positive treatment response [10]. There are newer attempts to define dyssynchrony and to better predict treatment failures by means of speckle tracking imaging and/or cardiac MRI [24-26]. One important potential of these methods is the identification of the site and extension of scars as well as extensive fibrosis, both of which have been shown to prevent an optimal treatment response to CRT [27, 28]. Whether these newer methods beyond that can better define responders versus nonresponders prospectively remains to be elucidated in long-term studies with larger patient cohorts.
In contrast to the lack of correlation between echocardiographic measurements of dyssynchrony and clinical response, we found several factors indicating poor outcome which are unrelated to cardiac dyssynchrony (Table 3). These included, not surprisingly, several markers of poor cardiac function, a finding which is in concordance with other studies showing that response to CRT is blunted in end-stage heart failure and suggesting the use of CRT implantation in earlier stages of the disease [7, 29]. This is also supported by recent randomized trials in less severe heart failure [7, 30]. On the other hand, diabetes and poor renal function were significantly related to poor outcome and lack of clinical improvement, highlighting the need of device studies in all-comers including patients with significant co-morbidities like in our study. These patients are poorly represented in prospective randomized trials. However, concurrent risks in severely comorbid patients may have a decisive role for outcome prediction on long term.
Study limitations
A main limitation of our study is the heterogeneity of patients, including all patients with biventricular pacing implanted in our center according to current guidelines (all-comers). Therefore, patients with non-ischemic cardiomyopathy as well as patients with coronary artery disease encompassing myocardial scar areas (possibly preventing favorable responses) were included. A substantial part had comorbid conditions which may have influenced outcome predominantely. On the other hand, the study was not powered enough to perform subgroup analyses or to correct for these factors, e.g. by propensity score analyses.
A further limitation is the definition of “responders” to therapy, which, however, is inherent to all similar studies. We tried to overcome this weakness by assessment of the response by experienced specialists blinded for the echocardiographic and electrocardiographic follow-up measurements related to dyssynchrony.
Clinical consequences and conclusions
In many institutions in-depth echocardiographic patient assessment is an integral part for optimal guidance of CRT. Repeated echocardiographic assessment of dyssynchrony and repeated reprogramming of the devices accordingly, is costly, technically challenging and time consuming. In accordance with the evidence from selected patient groups from randomized trials, our results on long term in unselected all-comers show that persistence or absence of dyssynchrony has no impact on outcome. Therefore, it seems reasonable to reduce markedly the complexity and frequency of echocardiographic follow-up examinations in patients with biventricular pacing.
More important, however, seems to be the consequence that the basic concept of “resynchronization” should be re-thought. It seems more appropriate to speak of modulation of dyssynchrony which is predominantely effective in patients with left bundle branch block and right ventricular pacing, whereas biventricular pacing to resynchronize patients with other forms of QRS prolongation or dyssynchrony with narrow QRS complexes is much more often futile.
Acknowledgments
The study was supported by the HerzGefassStiftung, Klinik Im Park, Zurich, Switzerland.
Financial Disclosures
None.
| References | ▴Top |
- Blanc JJ, Etienne Y, Gilard M, Mansourati J, Munier S, Boschat J, Benditt DG,
et al . Evaluation of different ventricular pacing sites in patients with severe heart failure: results of an acute hemodynamic study. Circulation. 1997;96(10):3273-3277.
doi pubmed - Prinzen FW, Vernooy K, De Boeck BW, Delhaas T. Mechano-energetics of the asynchronous and resynchronized heart. Heart Fail Rev. 2011;16(3):215-224.
doi pubmed - Ukkonen H, Sundell J, Knuuti J. Effects of CRT on myocardial innervation, perfusion and metabolism. Europace. 2008;10(Suppl 3):iii114-117.
doi pubmed - Cazeau S, Bordachar P, Jauvert G, Lazarus A, Alonso C, Vandrell MC, Mugica J,
et al . Echocardiographic modeling of cardiac dyssynchrony before and during multisite stimulation: a prospective study. Pacing Clin Electrophysiol. 2003;26(1 Pt 2):137-143.
doi pubmed - Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, Carson P,
et al . Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350(21):2140-2150.
doi pubmed - Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352(15):1539-1549.
doi pubmed - Moss AJ, Hall WJ, Cannom DS, Klein H, Brown MW, Daubert JP, Estes NA
3rd ,et al . Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009;361(14):1329-1338.
doi pubmed - Beshai JF, Grimm RA, Nagueh SF, Baker JH
2nd , Beau SL, Greenberg SM, Pires LA,et al . Cardiac-resynchronization therapy in heart failure with narrow QRS complexes. N Engl J Med. 2007;357(24):2461-2471.
doi pubmed - Ruschitzka F, Abraham WT, Singh JP, Bax JJ, Borer JS, Brugada J, Dickstein K,
et al . Cardiac-resynchronization therapy in heart failure with a narrow QRS complex. N Engl J Med. 2013;369(15):1395-1405.
doi pubmed - Gorcsan J
3rd , Oyenuga O, Habib PJ, Tanaka H, Adelstein EC, Hara H, McNamara DM,et al . Relationship of echocardiographic dyssynchrony to long-term survival after cardiac resynchronization therapy. Circulation. 2010;122(19):1910-1918.
doi pubmed - Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, Cleland J,
et al . 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: the task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Europace. 2013;15(8):1070-1118.
doi pubmed - Lecoq G, Leclercq C, Leray E, Crocq C, Alonso C, de Place C, Mabo P,
et al . Clinical and electrocardiographic predictors of a positive response to cardiac resynchronization therapy in advanced heart failure. Eur Heart J. 2005;26(11):1094-1100.
doi pubmed - Fornwalt BK, Sprague WW, BeDell P, Suever JD, Gerritse B, Merlino JD, Fyfe DA,
et al . Agreement is poor among current criteria used to define response to cardiac resynchronization therapy. Circulation. 2010;121(18):1985-1991.
doi pubmed - Notabartolo D, Merlino JD, Smith AL, DeLurgio DB, Vera FV, Easley KA, Martin RP,
et al . Usefulness of the peak velocity difference by tissue Doppler imaging technique as an effective predictor of response to cardiac resynchronization therapy. Am J Cardiol. 2004;94(6):817-820.
doi pubmed - Sogaard P, Egeblad H, Kim WY, Jensen HK, Pedersen AK, Kristensen BO, Mortensen PT. Tissue Doppler imaging predicts improved systolic performance and reversed left ventricular remodeling during long-term cardiac resynchronization therapy. J Am Coll Cardiol. 2002;40(4):723-730.
doi - Pitzalis MV, Iacoviello M, Romito R, Massari F, Rizzon B, Luzzi G, Guida P,
et al . Cardiac resynchronization therapy tailored by echocardiographic evaluation of ventricular asynchrony. J Am Coll Cardiol. 2002;40(9):1615-1622.
doi - Meluzin J, Novak M, Mullerova J, Krejci J, Hude P, Eisenberger M, Dusek L,
et al . A fast and simple echocardiographic method of determination of the optimal atrioventricular delay in patients after biventricular stimulation. Pacing Clin Electrophysiol. 2004;27(1):58-64.
doi pubmed - Sawhney NS, Waggoner AD, Garhwal S, Chawla MK, Osborn J, Faddis MN. Randomized prospective trial of atrioventricular delay programming for cardiac resynchronization therapy. Heart Rhythm. 2004;1(5):562-567.
doi pubmed - Jansen AH, Bracke FA, van Dantzig JM, Meijer A, van der Voort PH, Aarnoudse W, van Gelder BM,
et al . Correlation of echo-Doppler optimization of atrioventricular delay in cardiac resynchronization therapy with invasive hemodynamics in patients with heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol. 2006;97(4):552-557.
doi pubmed - Ellenbogen KA, Gold MR, Meyer TE, Fernndez Lozano I, Mittal S, Waggoner AD, Lemke B,
et al . Primary results from the SmartDelay determined AV optimization: a comparison to other AV delay methods used in cardiac resynchronization therapy (SMART-AV) trial: a randomized trial comparing empirical, echocardiography-guided, and algorithmic atrioventricular delay programming in cardiac resynchronization therapy. Circulation. 2010;122(25):2660-2668.
doi pubmed - Boriani G, Biffi M, Muller CP, Seidl KH, Grove R, Vogt J, Danschel W,
et al . A prospective randomized evaluation of VV delay optimization in CRT-D recipients: echocardiographic observations from the RHYTHM II ICD study. Pacing Clin Electrophysiol. 2009;32(Suppl 1):S120-S125.
doi pubmed - Abraham WT, Gras D, Yu CM, Guzzo L, Gupta MS. Rationale and design of a randomized clinical trial to assess the safety and efficacy of frequent optimization of cardiac resynchronization therapy: the Frequent Optimization Study Using the QuickOpt Method (FREEDOM) trial. Am Heart J. 2010;159(6):944-948 e941.
- Ritter P, Delnoy PP, Padeletti L, Lunati M, Naegele H, Borri-Brunetto A, Silvestre J. A randomized pilot study of optimization of cardiac resynchronization therapy in sinus rhythm patients using a peak endocardial acceleration sensor vs. standard methods. Europace. 2012;14(9):1324-1333.
doi pubmed - Tanaka H, Nesser HJ, Buck T, Oyenuga O, Janosi RA, Winter S, Saba S,
et al . Dyssynchrony by speckle-tracking echocardiography and response to cardiac resynchronization therapy: results of the Speckle Tracking and Resynchronization (STAR) study. Eur Heart J. 2010;31(14):1690-1700.
doi pubmed - Oyenuga O, Hara H, Tanaka H, Kim HN, Adelstein EC, Saba S, Gorcsan J
3rd . Usefulness of echocardiographic dyssynchrony in patients with borderline QRS duration to assist with selection for cardiac resynchronization therapy. JACC Cardiovasc Imaging. 2010;3(2):132-140.
doi pubmed - Marsan NA, Westenberg JJ, Ypenburg C, van Bommel RJ, Roes S, Delgado V, Tops LF,
et al . Magnetic resonance imaging and response to cardiac resynchronization therapy: relative merits of left ventricular dyssynchrony and scar tissue. Eur Heart J. 2009;30(19):2360-2367.
doi pubmed - Ypenburg C, Schalij MJ, Bleeker GB, Steendijk P, Boersma E, Dibbets-Schneider P, Stokkel MP,
et al . Impact of viability and scar tissue on response to cardiac resynchronization therapy in ischaemic heart failure patients. Eur Heart J. 2007;28(1):33-41.
doi pubmed - Bleeker GB, Kaandorp TA, Lamb HJ, Boersma E, Steendijk P, de Roos A, van der Wall EE,
et al . Effect of posterolateral scar tissue on clinical and echocardiographic improvement after cardiac resynchronization therapy. Circulation. 2006;113(7):969-976.
doi pubmed - van Bommel RJ, Bax JJ, Abraham WT, Chung ES, Pires LA, Tavazzi L, Zimetbaum PJ,
et al . Characteristics of heart failure patients associated with good and poor response to cardiac resynchronization therapy: a PROSPECT (Predictors of Response to CRT) sub-analysis. Eur Heart J. 2009;30(20):2470-2477.
doi pubmed - Linde C, Abraham WT, Gold MR, St John Sutton M, Ghio S, Daubert C. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol. 2008;52(23):1834-1843.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.