

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Case Report
Volume 6, Number 4-5, October 2015, pages 332-335
Myopericarditis: A Diagnosis of Uncertainty
Rafay Khana, b, Nneka Irokaa, Sunil Tulpulea, Sabrina Arsheda, Mohammad Ansaria, Puneet Sahgala, Abdalla Yousifa
aDepartment of Internal Medicine, Raritan Bay Medical Center, 530 New Brunswick Ave., Perth Amboy, NJ, USA
bCorresponding Author: Rafay Khan, 11 Hop Brook Lane, Holmdel, NJ 07733, USA
Manuscript accepted for publication October 15, 2015
Short title: Myopericarditis
doi: http://dx.doi.org/10.14740/cr428w
| Abstract | ▴Top |
Myocarditis can present in many different forms and can be overlooked by more life-threatening conditions. At times it may mimic conditions such as acute myocardial infarction and although it may have features highly suggestive of myocarditis, other etiologies need to be excluded. Thus, due to its clinical presentation, lab findings, and electrocardiogram analysis, it often can be confused with other conditions, making it a diagnostic dilemma of uncertainty. Myopericarditis is normally caused by viral infections, most common of which is coxsackievirus. Here we report a case of a 52-year-old gentleman who presented with a clinical picture of acute myocardial ischemia versus dissection, which overlooked a rather less threatening etiology of myopericarditis.
Keywords: Myocarditis; Pericarditis; Myopericarditis; Ischemia; Myocardial; Diagnosis
| Introduction | ▴Top |
As an acute inflammatory disease that mainly impacts the myocardium, acute myopericarditis can be caused by viruses, systemic conditions, drugs, or toxins. Pericarditis and myocarditis at times can present together and coexist as they share common underlying causes such as coxsackievirus [1-3]. The dilemma arises however in the diagnosis of this disorder as it mimics myocardial infarction and in this case report also had features of acute aortic dissection and pulmonary embolism. Few reports have demonstrated myopericarditis presenting not only as acute myocardial infarction but also a symptomatic picture suggesting aortic dissection.
| Case Report | ▴Top |
A 52-year-old male with a past medical history of hypertension, hypercholesterolemia, and smoking presented to the emergency room with complaints of chest pain, insidious in onset, and getting progressively worse. The pain was relieved when lying on his back and radiated to the left side of his chest, arm, and upper back. The patient stated the pain was a 10/10 and felt like a tearing pain down his back. Initially, patient believed the symptoms were secondary to acid reflux and took Tums. Overnight, the symptoms failed to resolve and he thus presented to the hospital. Patient denied any palpitations but had shortness of breath upon deep inhalation.
Vital signs demonstrated a blood pressure of 159/89, heart rate of 107, respiratory rate of 19, temperature of 98 °F, and pulse oximetry of 93% saturation. Physical examination findings were significant for only chest wall tenderness upon palpation and the patient was in clear distress and discomfort secondary to the severity of his chest and back pain. No friction rub was evident. Initial laboratory data showed a hemoglobin of 14.1, hematocrit of 43.1, white blood cell count of 10.4, and platelets of 230. Basic metabolic panel illustrated a sodium of 140, potassium of 4.4, chloride of 98, bicarbonate of 30, blood urea nitrogen of 24, creatinine of 1.7, and glucose of 99. His CKMB was 9.41 and his first troponin was elevated at 11.54. EKG (Fig. 1) illustrated ST elevations in multiple leads and thus Code Heart was called and patient was taken for cardiac catheterization.
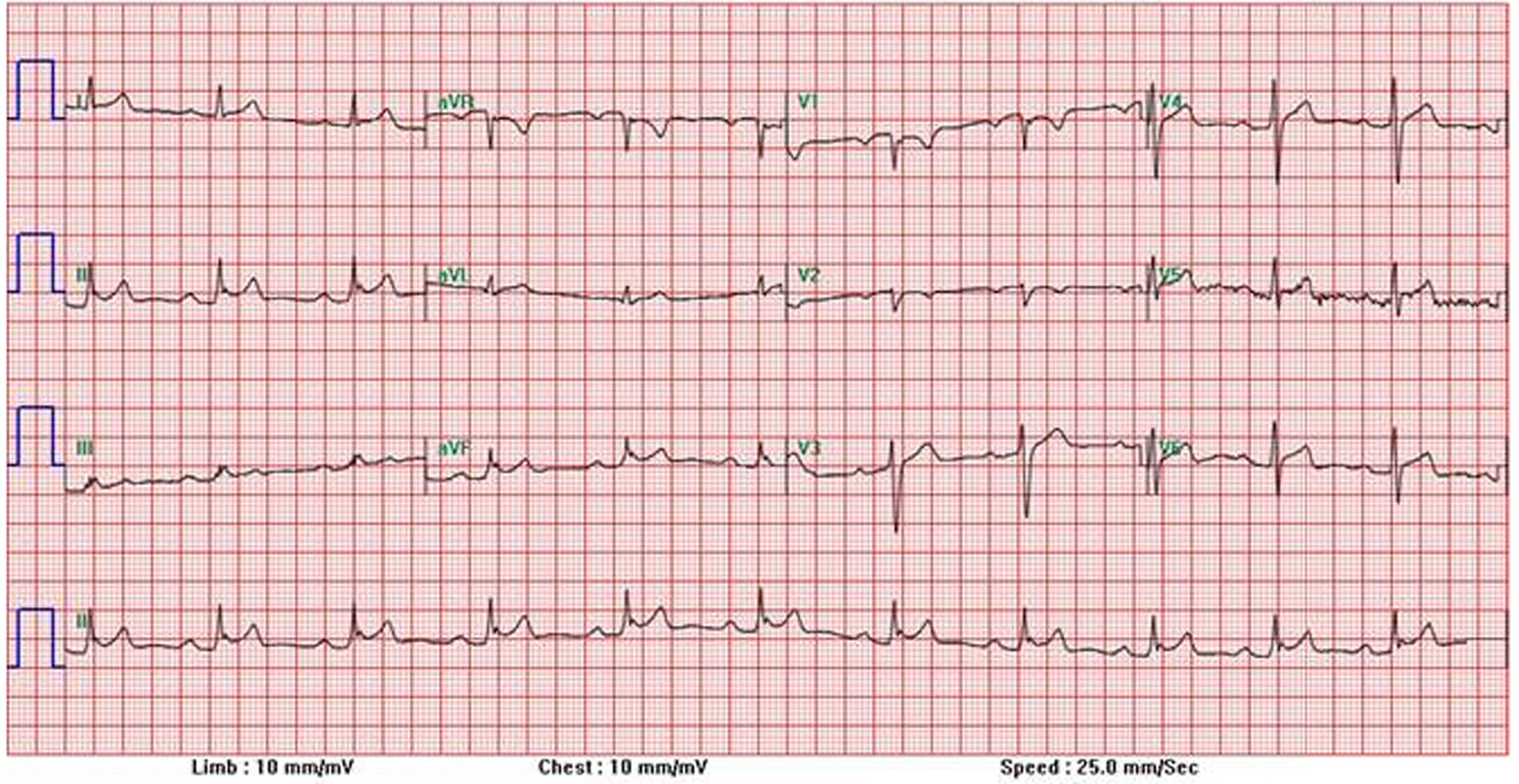 Click for large image | Figure 1. 12-Lead EKG demonstrating diffuse ST elevations. |
Cardiac catheterization revealed patent arteries and no occlusions were noted (Fig. 2). Post catheterization, patient continued to remain tachycardic and in significant distress from back pain. Aortic dissection and pulmonary embolism remained in the differentials at the time. Due to an elevated creatinine, a ventilation/perfusion (V/Q) scan was conducted while intravenous hydration was given. V/Q scan demonstrated indeterminate probability of pulmonary embolism. The following day with improvement in his creatinine, the patient underwent computed tomography angiography (CTA), which concluded that there was negative for dissection or embolism (Fig. 3). The clinical picture of the patient over the next few days improved with the use of NSAIDs. Serology later returned suggesting the presence of Coxsackie B virus.
 Click for large image | Figure 2. Cardiac catheterization illustrating patent arteries without any signs of occlusion or ischemia. |
 Click for large image | Figure 3. CT angiogram conducted showing absence of pulmonary embolism. |
| Discussion | ▴Top |
Although there are multiple causes of myocarditis, pericarditis, and myopericarditis, viruses are one of the most common (Table 1). Coxsackie B virus, as seen in our patient, is the most commonly associated viral cause of myocarditis.
 Click to view | Table 1. List of Viral Causes of Myocarditis |
The diagnosis and management of acute myopericaditis as early as possible is important, however may be limited by symptoms and signs suggesting a different cardiopulmonary process. It is also important to distinguish pericarditis from myocarditis as myocarditis has significant complications such as ventricular arrhythmia, cardiac dilation, and cardiac collapse which can develop rather abruptly [4, 5].
The gold standard of diagnosis, though not used commonly, is endomyocardial biopsy. It remains limited in its role due to a poor sensitivity and is not commonly used unless the patient is not responding well to medical treatment [1]. Endomyocardial biopsy shows a sensitivity of 43-64% and an overall complication rate of 6% with a 0.4% incidence of death due to perforation [6]. Another diagnostic modality that has been used is radiolabeled antimyosin antibody which can identify myocarditis but is non-specific as it detects myocardial necrosis from any cause and has a sensitivity of 67% and specificity of 63% [7, 8]. A third option involves the use of cardiac magnetic resonance imaging (CMR). This modality can find myocardial edema and myocyte damage non-invasively showing a characteristic pattern of contrast enhancement in patients with myocarditis [8]. However, in patients with infraction, it will show sub-endocardial enhancement, rather than enhancement originating from the epicardium and sparing the sub-endocardial layer as seen in myocarditis [8]. Unfortunately, the use of these diagnostic tests is not at all times beneficial, not available at many facilities, and only necessary when medical management does not show a clinical improvement in the patient’s symptoms.
A diagnosis of myocarditis is essential with the exclusion of other conditions, as myocarditis can be fatal and also lead to dilated cardiomyopathy and chronic heart failure as well. A better understanding of the pathophysiology and destructive nature of myocarditis through heart muscle destruction and development of dilated cardiomyopathy is important as it may improve the ease of its diagnosis and decrease the need for other diagnostic procedures. With a better understanding, interventions such as cardiac catheterization, CT angiograms, biopsy, and other diagnostic tests can be avoided.
Viruses mediate toxicity through focal necrosis of myocytes in the absence of inflammatory cell infiltrate within 3 days of infection and NK cells, protective antiviral antibodies, and infiltrating macrophages clear the virus from the myocardium [9]. The dilemma arises however as many symptoms and lab studies show overlapping features of ischemia and myocarditis. Myocarditis can demonstrate a rise in creatine kinase and electrocardiographic abnormalities as well. Along with ST elevations that may be diffuse, diffuse T wave abnormalities are a frequent feature on 12 lead ECK, with even 20% of patients developing a left bundle branch block [10]. As many of these features overlap with findings found in acute myocardial ischemia, it becomes difficult for a physician to make a clinical judgment in whether cardiac catheterization as a method of exclusion is necessary.
Conclusion
To summarize, patients with myocarditis present with several symptoms, clinical and laboratory findings that may coincide with other diagnoses such as ischemia. In our case report, due to the severity of the patient’s presentation, significant back pain, tachycardia, respiratory distress, and other diagnoses such as aortic dissection and pulmonary embolism also need to be excluded. Thus, awareness of myocarditis presenting similar to these other conditions, can help physicians avoid unnecessary examinations and rapidly correct the underlying cause to prevent long-term risks. However, it is vital to keep other conditions in mind as the risk of long-term complications can be detrimental to a patient’s outcome.
Acknowledgement
Internal Medicine Department and Cardiology Department, Raritan Bay Medical Center.
Competing Interests
There are no competing interests for this article.
Funding
No funding was provided for this article.
| References | ▴Top |
- Lee WS, Lee KJ, Kwon JE, Oh MS, Kim JE, Cho EJ, Kim CJ. Acute viral myopericarditis presenting as a transient effusive-constrictive pericarditis caused by coinfection with coxsackieviruses A4 and B3. Korean J Intern Med. 2012;27(2):216-220.
doi pubmed - Imazio M, Trinchero R. Myopericarditis: Etiology, management, and prognosis. Int J Cardiol. 2008;127(1):17-26.
doi pubmed - Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004;351(21):2195-2202.
doi pubmed - Oakley CM. Myocarditis, pericarditis and other pericardial diseases. Heart. 2000;84(4):449-454.
doi pubmed - Roubille F, Gahide G, Moore-Morris T, Granier M, Davy JM, Vernhet H, Piot C. Epstein Barr virus (EBV) and acute myopericarditis in an immunocompetent patient: first demonstrated case and discussion. Intern Med. 2008;47(7):627-629.
doi pubmed - Deckers JW, Hare JM, Baughman KL. Complications of transvenous right ventricular endomyocardial biopsy in adult patients with cardiomyopathy: a seven-year survey of 546 consecutive diagnostic procedures in a tertiary referral center. J Am Coll Cardiol. 1992;19(1):43-47.
doi - Sarda L, Colin P, Boccara F, Daou D, Lebtahi R, Faraggi M, Nguyen C, et al. Myocarditis in patients with clinical presentation of myocardial infarction and normal coronary angiograms. J Am Coll Cardiol. 2001;37(3):786-792.
doi - Chrysohoou C, Tsiamis E, Brili S, Barbetseas J, Stefanadis C. Acute myocarditis from coxsackie infection, mimicking subendocardial ischaemia. Hellenic J Cardiol. 2009;50(2):147-150.
pubmed - Kearney MT, Cotton JM, Richardson PJ, Shah AM. Viral myocarditis and dilated cardiomyopathy: mechanisms, manifestations, and management. Postgrad Med J. 2001;77(903):4-10.
doi pubmed - Toshima H, Ohkita Y, Shingu M. Clinical features of acute coxsackie B viral myocarditis. Jpn Circ J. 1979;43(5):441-444.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.