

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Case Report
Volume 8, Number 2, April 2017, pages 52-56
Primary Percutaneous Coronary Intervention Angioplasty of Occluded Twin Circumflex Coronary Artery in a Patient of Acute Inferior Wall Myocardial Infarction: A Rare Anomaly
Santosh Kumar Sinhaa, b, Vikas Mishraa, Nasar Abdalia, Mukesh Jitendra Jhaa, Mahmadula Razia, Shravan Singha, Lokendra Rekwala, Vikas Chaturvedia, Chandra Mohan Varmaa, Ramesh Thakura
aDepartment of Cardiology, LPS Institute of Cardiology, G.S.V.M. Medical College, Kanpur, Uttar Pradesh 208002, India
bCorresponding Author: Santosh Kumar Sinha, Department of Cardiology, LPS Institute of Cardiology, G.S.V.M. Medical College, Kanpur, Uttar Pradesh 208002, India
Manuscript accepted for publication March 14, 2017
Short title: Twin Circumflex Coronary Artery
doi: https://doi.org/10.14740/cr530w
| Abstract | ▴Top |
Anomalies of the coronary arteries are reported in 1-2% of patients among diagnostic angiogram. Dual origin of a circumflex from both sinuses is extremely rare among them. We report a case of a patient who underwent primary percutaneous coronary intervention for acute inferior wall myocardial infarction where left coronary injection demonstrated normal obtuse marginal and right coronary injection demonstrated normal right coronary artery (RCA). On further probing, an anomalous left circumflex (LCx) artery was seen arising from RCA ostium which was subsequently cannulated and revascularized by deployment of 2.75 × 26 mm Xience Prime drug-eluting stent (Abott Vascular, USA). Herein, we report for the first time primary percutaneous coronary intervention of twin circumflex and also illustrate that anomalous circumflex can be missed if it arises from RCA ostium and if not probed carefully.
Keywords: Coronary artery anomalies; Twin circumflex arteries; RCA ostium; Primary PCI; Myocardial infarction
| Introduction | ▴Top |
Malformation within coronary buds on the aortic sinuses or vascular plexuses to which they connect during fetal development leads to coronary artery anomalies whose incidence varies from 0.6% to 1.5%, being totally asymptomatic to life threatening [1-3]. Although anomalously originating left circumflex (LCx) artery from the right sinus of Valsalva is one of the most common coronary anomalies, this carries little clinical significance unless it is critically diseased [4]. However, double LCx arteries is an exceedingly rare anomaly with just few cases reported in the literature.
| Case Report | ▴Top |
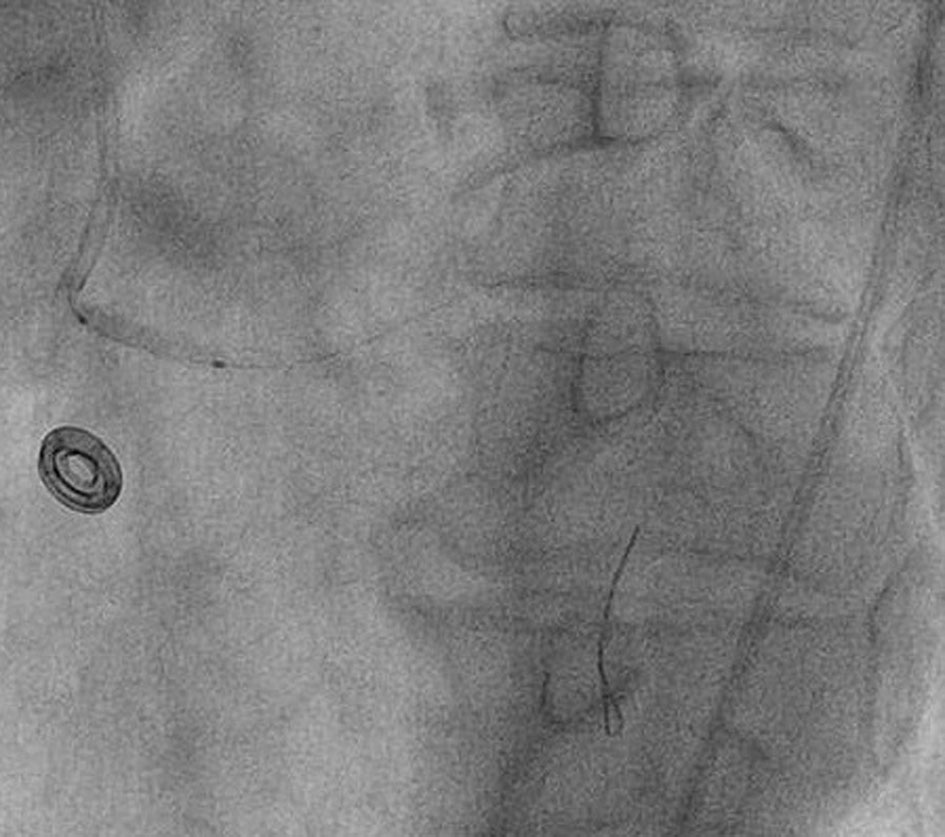
A 49-year-old female with a past history of diabetes mellitus, hypertension, and dyslipidemia presented with retrosternal chest pain and sweating of 3 h duration. Her physical examination and biochemistry were all unremarkable. Echocardiography revealed mild hypokinesia in LCx territory with ejection fraction of 55%. Electrocardiogram revealed ST-elevation in II, III, and aVF and reciprocal changes in I and aVL. She was taken for primary percutaneous coronary intervention (PCI) through femoral route after proper consent. She was preloaded with prsugrel 60 mg, aspirin 325 mg and atorvastatin 80 mg. The 6 F JR3.5 and JL3.5 ProfloTM diagnostic catheters (Medtronic, USA) were used for catheterization after administering 2,500 U of heparin. Angiogram of left system revealed plaque in distal left main, critical lesion in proximal left anterior descending (LAD) artery and normal obtuse marginal branch (Fig. 1). Right coronary artery (RCA) was uneventful showing a smooth, normal coronary artery (Fig. 2). We started looking for LCx as it was incompatible with diagnosis. On gradual pullback of JR diagnostic catheter, LCx was seen arising from RCA ostium showing tubular lesion with 90% stenosis in proximal segment (Figs. 3 and 4). Therefore, angiogram revealed a double LCx: one arising from left and the other originating from RCA ostium. PCI was planned of the culprit artery only and 7,000 U of heparin was given further. As a 6 F JR3.5 guiding catheter (Medtronic, USA) was deeply engaging RCA similar to diagnostic one, it was improvized by slightly straightening its tip (Fig. 5) and LCx was cannulated with counterclock twist (Fig. 6). Amplatzer catheter (AL) was avoided to prevent ostial injury to RCA and double jeopardy in form of injury of RCA and LCx. As support was not adequate, two balance middle weight (BMW) guidewires 0.014″, 190 cm (Abott, USA) were parked beyond the lesion, second acting as buddy wire (Fig. 6). Lesion was pre-dilated with 2 × 10 mm Minitrak balloon (Abott, USA) to 12 atm (Fig. 6). After positioning the stent, buddy wire was pulled into the guiding. Lesion was stented by deploying 2.75 × 33 mm Xience Prime stent (Everolimus drug-eluting stent, Abott, USA) up to 13 atm pressure (Fig. 7) and further post-dilated by 2.75 × 10 mm Minitrak non-compliant balloon up to 24 atm (Abott, USA) achieving TIMI 3 flow in LCx (Figs. 8 and 9). Her symptom and ECG were stabilized. The patient was discharged on the following day with aspirin 150 mg/day, prasugrel 10 mg/day, atorvastatin 80 mg/day, metoprolol 100 mg/day and ramipril 2.5 mg/day. Patient is doing excellent since then with regular follow-up at our institute.
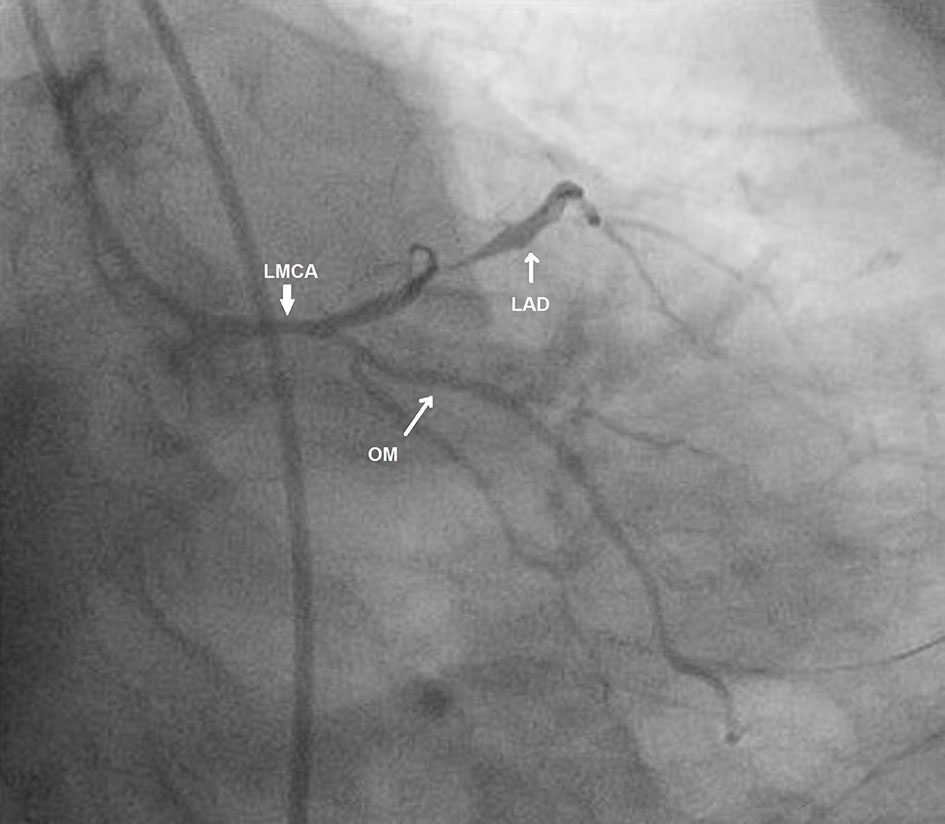 Click for large image | Figure 1. Left main coronary artery with left anterior descending (LAD) and obtuse marginal (OM) artery in antero-posterior caudal view. |
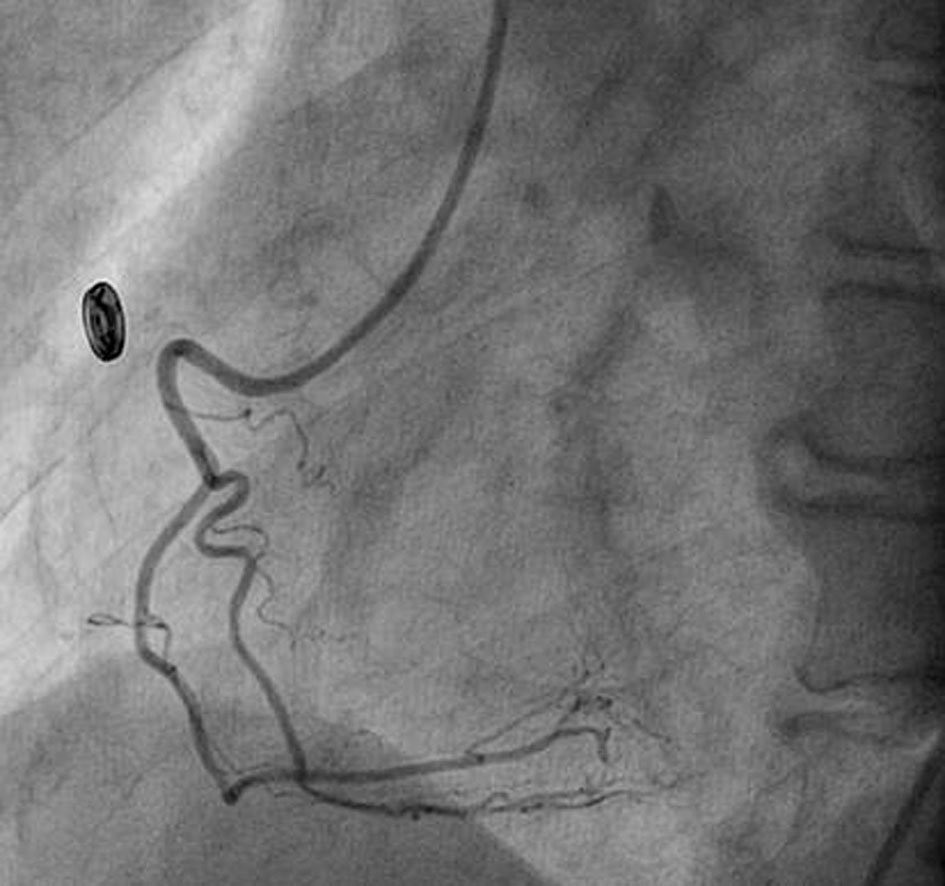 Click for large image | Figure 2. Normal right coronary artery. |
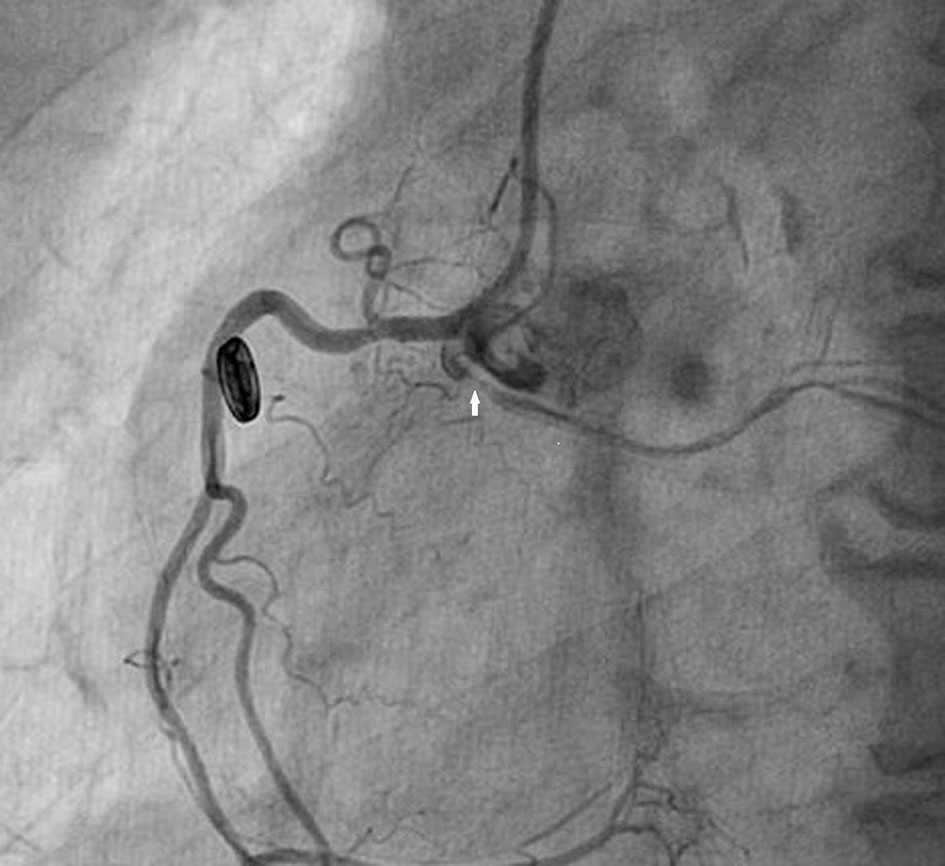 Click for large image | Figure 3. Anomalous LCx from RCA ostium showing critical lesion with haziness in proximal part (white arrow) in left anterior oblique view. |
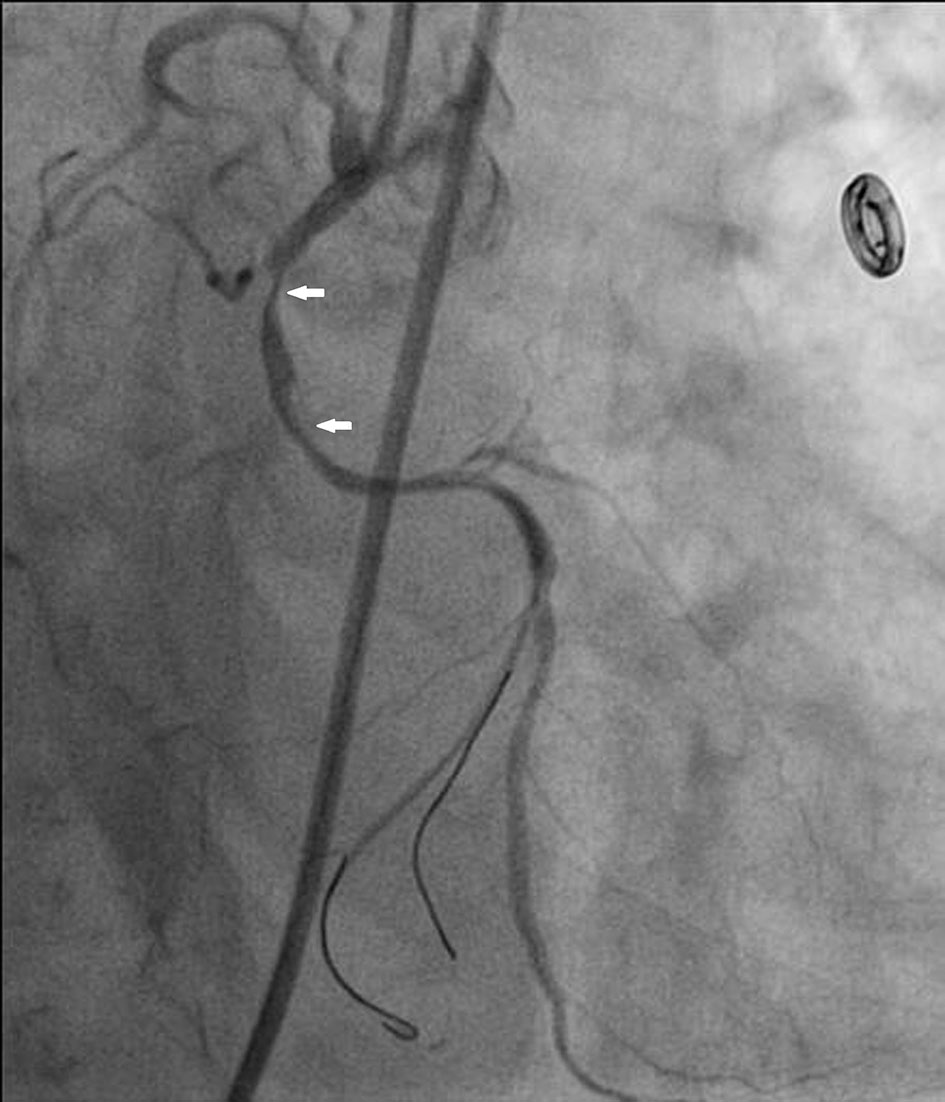 Click for large image | Figure 4. Anomalous LCx from RCA ostium showing critical lesion with haziness in proximal part (white arrow) in left anterior oblique with cranial tilt. |
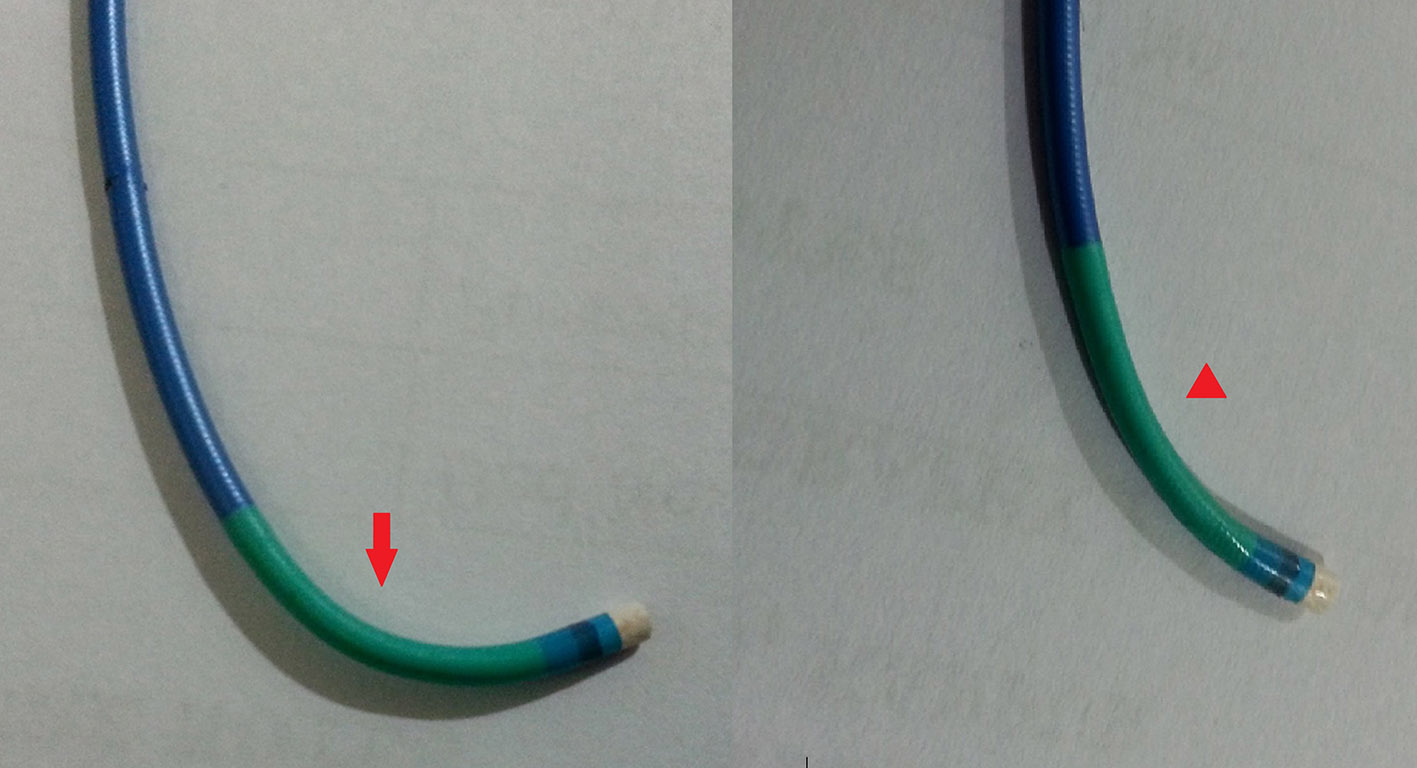 Click for large image | Figure 5. Improvization of Judkins right catheter by straightening its tip. |
 Click for large image | Figure 6. Cannulated LCx with help of buddy wire and lesion being pre-dilated with 2 × 10 mm Minitrak balloon. |
 Click for large image | Figure 7. Lesion being stented by 2.75 × 33 mm Xience Prime drug-eluting stent (Abott, USA). |
 Click for large image | Figure 8. Stent being post-dilated by 2.75 × 10 mm Minitrak non-compliant balloon. |
 Click for large image | Figure 9. TIMI 3 flow in LCx after dilatation. |
| Discussion | ▴Top |
Normally, the left main coronary artery originates from the left sinus of Valsalva and gives rise to the LAD artery and LCx artery. LCx artery courses in the left atrioventricular groove and provides the first obtuse marginal branch. The most frequently found anomalies include a circumflex artery with a separate origin of the LAD and LCx arteries, followed by an LCx artery arising from the right sinus of Valsalva or the RCA [3]. Although there have been few cases of dual origin of an LCx artery, primary PCI has not been ever reported. In a study by Wilkins et al [5], 71% patients with an anomalous circumflex artery had significant coronary atherosclerosis in the proximal portion of anomalous vessel, a finding similarly shown in analysis from the coronary artery surgery study by Click et al [6]. The retro-aortic course of the anomalous circumflex coronary artery may predispose this vessel to atherosclerosis in patients with coronary disease. Anomalous circumflex was infarct-related artery in our case.
The most important problem in diagnosing double circumflex arteries is the separate origin of the two circumflex arteries from different ostia. Thus, we must always keep in mind this possibility as had it not been acute IWMI, we could have missed ectopic LCx as it was originating from RCA ostium and catheter was engaging RCA beyond its ostia. Whenever, intervention is contemplated, support is prime issue as it runs a tortuous curse so delivery of hardware becomes challenging. It can be circumvented by choosing either a guide with additional support as Voda catheter or Amplatzer catheter or buddy wire as in our case.
In conclusion, the diagnosis of coronary artery anomalies (CAAs) is often incidentally, but some CAAs could lead to acute coronary syndrome. Therefore, diagnosis and treatment of these pathologies are very important. The clue of diagnosis is clinical and angiographic suspicion, if the posterolateral left ventricular myocardium has vascular hole during left coronary artery opacification despite wall motion in that area being normal or if the usual coronary arteries are normal in the case of an acute coronary syndrome. Multidetector computed tomography might be an alternative or adjunctive imaging modality to coronary angiography but in setting of acute coronary syndrome, it should be avoided as time is golden.
Conflicts of Interest
None.
Financial Disclosure
None.
| References | ▴Top |
- Bogers AJ, Gittenberger-de Groot AC, Poelmann RE, Peault BM, Huysmans HA. Development of the origin of the coronary arteries, a matter of ingrowth or outgrowth? Anat Embryol (Berl). 1989;180(5):437-441.
doi - Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21(1):28-40.
doi pubmed - Angelini P, Villason S, Chan A V, Jr. Normal and anomalous coronary arteries in humans. In: Angelini P, editor. Coronary Artery Anomalies: A Comprehensive Approach. Philadelphia, PA: Lippincott Williams & Wilkins; 1999. p. 27-79.
- Tedeschi C, De Rosa R, Ratti G, Sacco M, Borrelli F, Runza G, Midiri M, et al. [Anomalous origin of the circumflex artery from the right aortic sinus: assessment with conventional coronary angiography and multislice computed tomography]. G Ital Cardiol (Rome). 2008;9(6):421-424.
- Wilkins CE, Betancourt B, Mathur VS, Massumi A, De Castro CM, Garcia E, Hall RJ. Coronary artery anomalies: a review of more than 10,000 patients from the Clayton Cardiovascular Laboratories. Tex Heart Inst J. 1988;15(3):166-173.
pubmed - Click RL, Holmes DR, Jr., Vlietstra RE, Kosinski AS, Kronmal RA. Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival - a report from the Coronary Artery Surgery Study. J Am Coll Cardiol. 1989;13(3):531-537.
doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.