Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access
Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc
Journal website http://www.cardiologyres.org
Case Report
Volume 8, Number 3, June 2017, pages 123-127
Ticagrelor-Associated Conduction Disorder: A Case Report and Review of the Literature
Mustafa Yurtdasa, c, Mahmut Ozdemirb
aDepartment of Cardiology, Sevgi Hospital, Balikesir, Turkey bDepartment of Cardiology, Cihanpol Hospital, Mardin, Turkey cCorresponding Author: Mustafa Yurtdas, Department of Cardiology, Sevgi Hospital, Pasaalani Mah. 10020, Balikesir, Turkey
Manuscript submitted May 11, 2017, accepted May 24, 2017 Short title: Ticagrelor and Conduction Disorder doi: https://doi.org/10.14740/cr556w
A 47-year-old female presented to emergency clinic due to non-ST-elevation myocardial infarction (NSTEMI). After receiving acetylsalicylic acid, a loading dose of ticagrelor 180 mg and intravenous unfractionated heparin, she underwent successful placement of drug eluting stent on the distal part of non-dominant left circumflex artery. The patient had no pre-existing atrioventricular (AV) block and did not use AV blocking agent. Approximately 10 h after taking a loading dose of ticagrelor, baseline normal rhythm degenerated to the first and then complete AV block, with mild dizziness. Following cessation of ticagrelor, cardiac rhythm returned to normal level within 2 days. The close monitoring of patients after starting ticagrelor is imperative, so ticagrelor may result in advanced conduction disorders. Here, we report a patient who developed various types of AV block associated with the ticagrelor taken during successful percutaneous coronary intervention for NSTEMI. We also reviewed the literature on the association between ticagrelor use and conduction abnormalities.
P2Y12 platelet receptor inhibitors (i.e., clopidogrel, ticagrelor and prasugrel) are the mainstay of therapy in acute coronary syndrome (ACS) at the moment [1, 2]. Ticagrelor is preferred over clopidogrel for ACSs due to their more rapid and more potent antiplatelet activation [3]. As well as its beneficial effects, ticagrelor may give rise to adverse events such as dyspnea and symptomatic or asymptomatic arrhythmias [4]. Herein, we report a patient who developed the first degree and then complete atrioventricular (AV) block (AVB) with mild dizziness approximately 10 h after taking a loading dose of 180 mg ticagrelor during successful percutaneous intervention of the distal occlusion of non-dominant left circumflex artery (ndLCx) for ACS (non-ST-elevation myocardial infarction, NSTEMI). We also reviewed the literature on the association between ticagrelor use and conduction abnormalities.
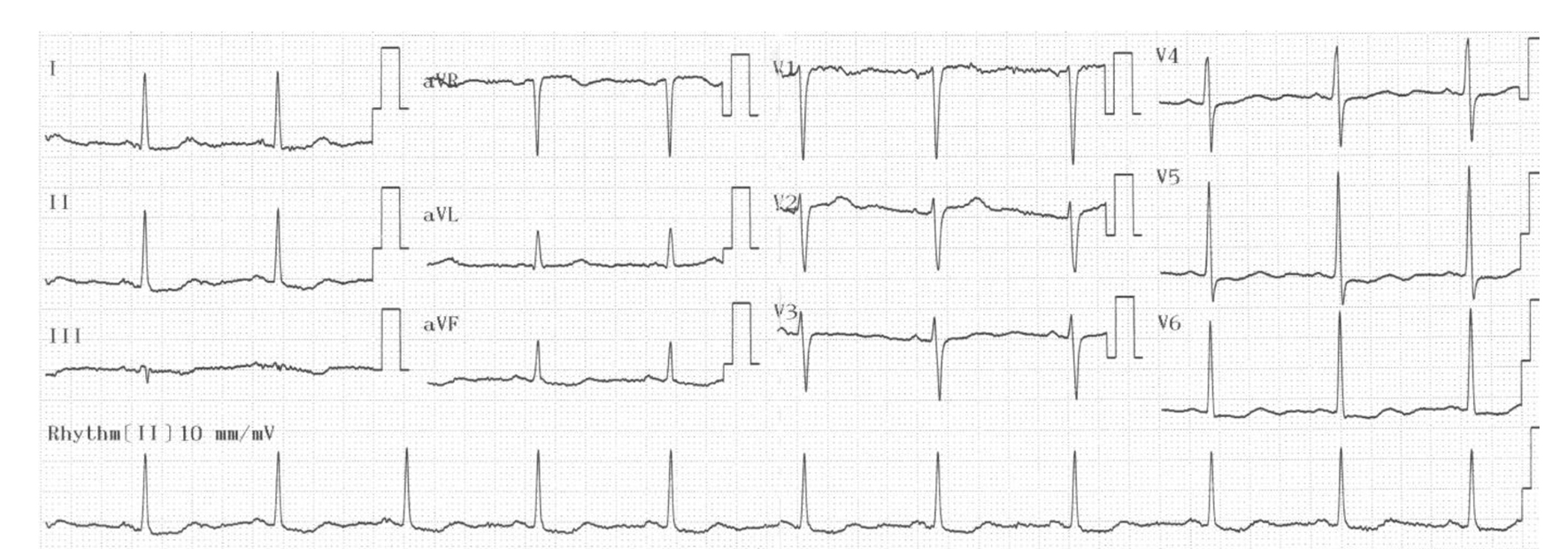
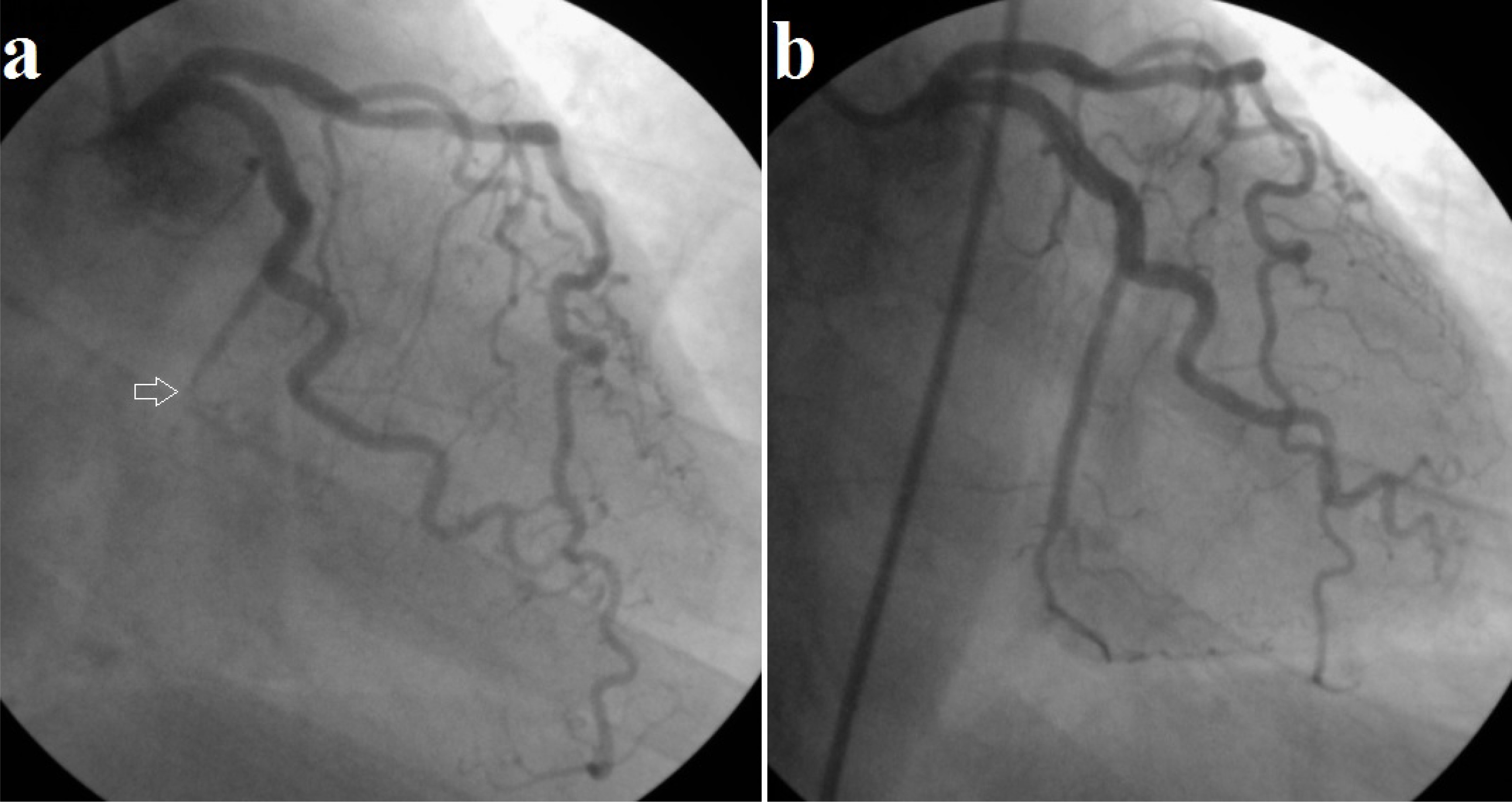
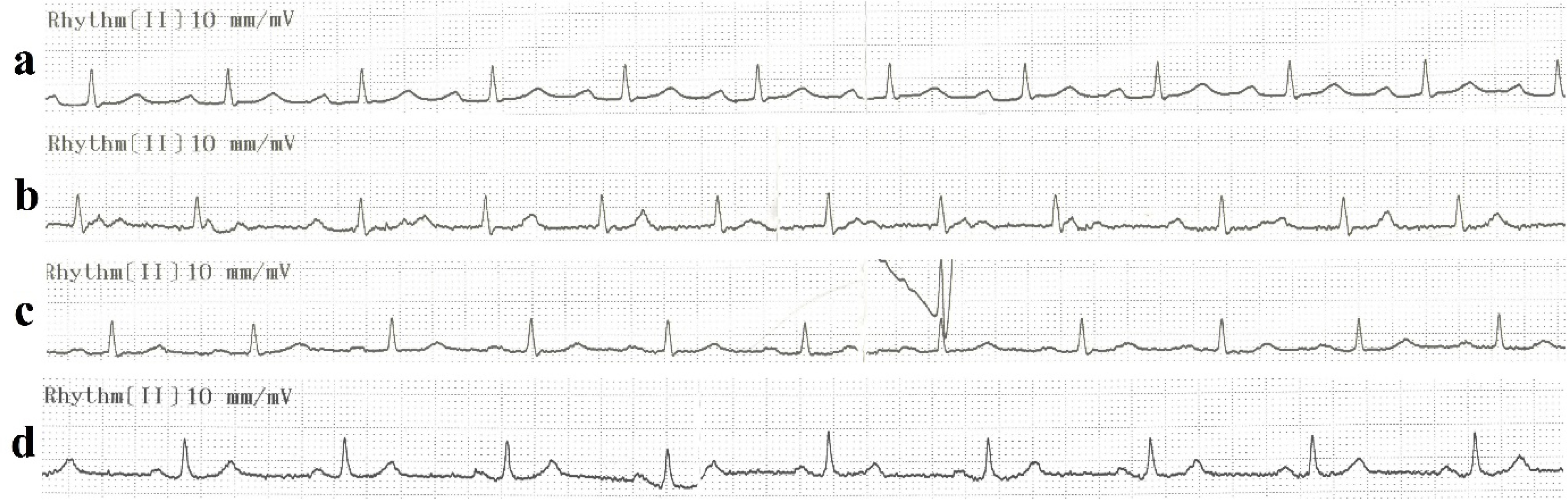
A 47-year-old female with hypertension and hyperlipidemia was admitted to emergency department due to typical angina lasting 2 days. Her blood pressure was 150/80 mm Hg. On electrocardiogram (ECG), there was a sinus rhythm with heart rate of 67 bpm, along with ST depression of 0.5 mm on inferolateral derivations (Fig. 1). Echocardiography showed hypokinesis of mid-lateral wall with an ejection fraction of 48%. We detected slightly increased cardiac troponin level. Because of ACS (NSTEMI), acetylsalicylic acid (300 mg), ticagrelor (a loading dose of 180 mg and maintenance dose of 90 mg twice a day) and intravenous unfractionated heparin (10,000 IU) were given to the patient and then her coronary angiography was performed, which revealed a total occlusion of the distal ndLCx (Fig. 2a). After the lesion was predilated with 2.0 × 15 mm sized balloon catheter, a drug eluting stent of 2.5 × 23 mm was implanted and full patency was achieved (Fig. 2b). Thereafter, her symptoms dramatically improved. Since her heart rate was 67 beats/min, beta blocker therapy was not started. Approximately 10 h later, ECG showed first degree AVB without symptom (Fig. 3a). Her therapy consisting of ASA, ticagrelor, ramipril and statin was continued unchanged. On the next (second) day, the patient experienced mild dizziness with complet AVB, without hemodynamic impairment (Fig. 3b). Ticagrelor was stopped and prasugrel was initiated instead. On the third day, her ECG showed again first degree AVB without symptom (Fig. 3c). On the fourth day, she had normal sinus rhythm without AVB and symptom (Fig. 3d). On the fifth day, the patient was salubriously discharged from the hospital with therapy of ASA, prasugrel, rosuvastatin and ramipril. We did not observe any heart block and/or bradyarrhythmia during the 3 months of follow-up.
Figure 2. Coronary angiography showing distal occlusion of the ndLCx artery (a, white arrow), and full patency of the relevant thrombotic lesion after successful percutaneous coronary intervention (b). ndLCx: non-dominant left circumflex.
Figure 3. ECGs showing a sinus rhythm with prolonged PR interval of 260 ms approximately 10 h after taking ticagrelor loading dose (a), complete atrioventricular block on the next (second) day (b), mild first degree atrioventricular block at 220 ms after the cessation of ticagrelor on the third day (c), and normal sinus rhythm without evidence of conduction disorder on the fourth day (d).
Ticagrelor is a cyclopentyltriazolopyrimidine, with a plasma half-life of approximately 6 - 12 h and, requires a dual daily orally administration and binding reversibly to the P2Y12 receptor [4]. It provides faster and more efficacious P2Y12 inhibition, culminating in significant reductions in cardiovascular events and improved survival in patients with ACS when compared to clopidogrel [3]. Recently, there have been several reports showing that ticagrelor may be associated with conduction abnormalities. After performing a detailed PubMed search, we were able to find only nine cases on topic of ticagrelor-related conduction abnormalities [5-13]. Table 1 [5-13] shows characteristics of the patients in the formerly reported those cases. The mean age of patients was 57.5 years, with 100% being male, except for one case, whose age and gender were not mentioned [10]. All patients developed various degrees of AVB and sinusal arrest or ventricular pause [5-12], except for one case who developed atrial fibrillation (AF) [13]. Of nine patients, six had pre-existing AV conduction disorder, eight were on AV blocking agents. The time from ticagrelor intake to onset of cardiac arrhythmia (or related symptoms) ranged from 1 h to 2 months.
Table 1. Characteritics of Patients in the Cases of Ticagrelor-Induced Cardiac Arrhythmia Reported in the Literature [5-13]
AVB is partial or complete failure of impulse conduction from the atria to the ventricles. Idiopathic fibrosclerosis of the conduction system, also called Lenegre-Lev disease, is the most common cause of non-ischemic AVB. Acute or chronic ischemic coronary disease, myocarditis, infiltrative and infectious diseases, autoimmune disorders, surgical procedures, and some drugs such as negative chronotropic agents may lead to various degrees of AVB [14]. Lenegre-Lev disease is age-related defect and characterized by progressive deterioration of cardiac conduction system, leading to complete AVB, syncope and sudden death. The fact that our patient is young and AVB is reversible, indicating that the underlying pathology is not the Lenegre-Lev disease. No laboratory and physical examination findings were found to suggest the other diseases above-mentioned. The arterial blood supply of sinoatrial (SA) and AV nodes is procured by the SA and AV nodal branches, respectively, most commonly originating from the right coronary arter (RCA), although it can rarely be a branch of the LCx in patients with left coronary artery dominance. Therewithal, infranodal conduction system is nourished almost completely by the septal perforator branches of the left anterior descending (LAD) artery, with variable dual supply provided by either the RCA or LCx artery. Reduced aterial blood flow to the septal branches or RCA is therefore associated with a variety of conduction disturbances [15]. Our patient had a total thrombotic occlusion of the distal part of ndLCx, with minimal atherosclerotic disease on LAD and RCA. So it is not logical to think that the ndLCx artery lesion in our case is responsible for this conduction disturbance. Because our patient had an ischemia not associated with the blood supply of conduction system, no pre-existing conduction disease and no other diseases above-mentioned, and did not use AV blocking agents, we concluded that the ticagrelor was the responsible agent. Ticagrelor was discontinued, and the prasugrel was reloaded with a 60 mg dose, followed by standard daily maintenance dose of 10 mg.
In the DISPERSE-2 (Dose Confirmation Study Assessing Anti-Platelet Effects of AZD6140 vs. Clopidogrel in Non-ST-Segment Elevation Myocardial Infarction) trial, a phase IIb dose-ranging study in patients with ACS, a post hoc analysis of cardiac arrhythmias revealed an unexpected increase in the incidence of predominately asymptomatic ventricular pauses in patients treated with ticagrelor compared with those treated with clopidogrel [16]. For this reason, a prospective continuous ECG evaluation was carried out within the PLATO trial, and this new study (the PLATO ECG assessment) showed that those receiving ticagrelor were more likely to experience ventricular pauses than those treated with clopidogrel with no clinical importance [17]. Since this study excluded patients at an increased risk of bradicardia (known as sick sinus syndrome, first-, second- or third-degree AVB, etc.), it could not be possible to understand the actual relationship between ticagrelor use and arrhythmic events.
Although the mechanism by which ticagrelor paves the way for arrhythmias is not fully known, several potential hypotheses have been proposed. The first hypothesis is a direct effect of ticagrelor on cardiac automaticity and conduction, but this has never been noticed in pre-clinical and clinical trial on ticagrelor [17]. A second hypothesis is that ticagrelor inhibits cellular uptake and increases plasma concentration of adenosin [17, 18]. In in vitro and in vivo experiments, ticagrelor has been demonstrated to inhibit adenosine metabolism and elevate adenosine levels through prevention of adenosine uptake by eryhtrocytes [18]. Therefore, ticagrelor-induced increases in adenosin levels can be a reasonable explanation for the arrhythmic events observed in the cases reported. The another data supporting this hypothesis is that ticagrelor may give rise to AF. Zhang et al reported a patient with unstable angina and a history of paroxysmal AF who developed recurrent AF following ticagrelor use, and speculated that ticagrelor might provoke dormant pulmonary vein conduction and AF reccurence via increasing the levels of adenosin [12].
After the start of ticagrelor, the most important point is on the development of its side effects. There is consensus on the careful observation of patients, particularly those with already conduction disorder or those treated with one or more AV blocking drugs, after initiating of ticagrelor. Also, we recommend follow-up of patients who do not have compromised conduction system and/or do not use AV blocking agents at least during the hospital stay, because it has been shown that sinusal arrest with high-degree AVB occurred in a healthy volunteer following a large dose of ticagrelor [19].
Another important point relates to what should be done after the arrhythmic adverse event due to the use of ticagrelor is observed. In general, after the drug is stopped and appropriate P2Y12 receptor inhibitor (prasugrel or clopidogrel) is started instead, the heart rhythm is observed until the normal ECG findings return. During this period, hemodynamic follow-up and/or support are provided to the patient. There is no clear information on whether or not and when the pacemaker should be inserted, if the heart rhythm does not return to normal despite this practice. In the majority of published cases, ticagrelor has been stopped with the close hemodynamic monitoring, and significant improvements have been shown on patient’s symptoms and ECG findings, as observed in our case. So far, temporary pacemaker has been required for three patients [6-8], and permanent pacemaker has been implanted for only one patient who has unresolved AVB persisting for 10 days after the discontinuation of ticagrelor [10].
In conclusion, our report deals with the importance of awareness of the ticagrelor-related arrhythmic events such as sinusal arrest, ventricular pause, various degrees of AVB, and AF. Extreme caution and close monitoring after initiation of ticagrelor are needed in terms of development of cardiac arrhythmias in all patients, particularly with pre-existing conduction system disorder and/or on AV nodal blocking agents.
Conflicts of Interest
There are no conflicts of interest related to this manuscript.
Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Jr., Ganiats TG, Holmes DR, Jr., Jaffe AS, et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139-228. doipubmed
Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, Bax JJ, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(3):267-315. doipubmed
Wallentin L, Becker RC, Budaj A, Cannon CP, Emanuelsson H, Held C, Horrow J, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009;361(11):1045-1057. doipubmed
Nicol M, Deblaise J, Choussat R, Dubourg O, Mansencal N. Side effects of ticagrelor: Sinus node dysfunction with ventricular pause. Int J Cardiol. 2015;191:56-57. doipubmed
Goldberg A, Rosenfeld I, Nordkin I, Halabi M. Life-threatening complete atrioventricular block associated with ticagrelor therapy. Int J Cardiol. 2015;182:379-380. doipubmed
Goldberg A, Rosenfeld I, Nordkin I, Halabi M. Ticagrelor therapy in patients with advanced conduction disease: Is it really safe? Int J Cardiol. 2016;202:948-949. doipubmed
Baker NC, Nadour W, Friehling M. Clinically significant ticagrelor induced conduction abnormalities following percutaneous coronary intervention. Int J Cardiol. 2016;214:21-22. doipubmed
Ozturk C, Unlu M, Yildirim AO, Erdogan S, Demir M, Balta S, Demirkol S, et al. The progressed atrioventricular block associated with ticagrelor therapy may not require permanent pacemaker after acute coronary syndrome; it may be reversible. Int J Cardiol. 2016;203:822-824. doipubmed
Unlu M, Demirkol S, Yildirim AO, Balta S, Ozturk C, Iyisoy A. Atrioventricular block associated with ticagrelor therapy may require permanent pacemaker. Int J Cardiol. 2016;202:946-947. doipubmed
Sharma M, Mascarenhas DA. Ticagrelor Associated Heart Block: The Need for Close and Continued Monitoring. Case Rep Cardiol. 2017;2017:5074891. doi
Zhang N, Chen KY, Zhao J, Xu G, Li G, Liu T. Another side effect of ticagrelor: Atrial fibrillation. Int J Cardiol. 2016;212:242-244. doipubmed
Di Serafino L, Rotolo FL, Boggi A, Colantonio R, Serdoz R, Monti F. Potential additive effects of ticagrelor, ivabradine, and carvedilol on sinus node. Case Rep Cardiol. 2014;2014:932595. doi
Barra SN, Providencia R, Paiva L, Nascimento J, Marques AL. A review on advanced atrioventricular block in young or middle-aged adults. Pacing Clin Electrophysiol. 2012;35(11):1395-1405. doipubmed
Futami C, Tanuma K, Tanuma Y, Saito T. The arterial blood supply of the conducting system in normal human hearts. Surg Radiol Anat. 2003;25(1):42-49. doipubmed
Cannon CP, Husted S, Harrington RA, Scirica BM, Emanuelsson H, Peters G, Storey RF. Safety, tolerability, and initial efficacy of AZD6140, the first reversible oral adenosine diphosphate receptor antagonist, compared with clopidogrel, in patients with non-ST-segment elevation acute coronary syndrome: primary results of the DISPERSE-2 trial. J Am Coll Cardiol. 2007;50(19):1844-1851. doipubmed
Scirica BM, Cannon CP, Emanuelsson H, Michelson EL, Harrington RA, Husted S, James S, et al. The incidence of bradyarrhythmias and clinical bradyarrhythmic events in patients with acute coronary syndromes treated with ticagrelor or clopidogrel in the PLATO (Platelet Inhibition and Patient Outcomes) trial: results of the continuous electrocardiographic assessment substudy. J Am Coll Cardiol. 2011;57(19):1908-1916. doipubmed
Cattaneo M, Schulz R, Nylander S. Adenosine-mediated effects of ticagrelor: evidence and potential clinical relevance. J Am Coll Cardiol. 2014;63(23):2503-2509. doipubmed
Teng R, Butler K. Safety, tolerability, pharmacokinetics and pharmacodynamics of high single-ascending doses of ticagrelor in healthy volunteers. Int J Clin Pharmacol Ther. 2013;51(10):795-806. doipubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.