Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access
Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc
Journal website http://www.cardiologyres.org
Case Report
Volume 8, Number 3, June 2017, pages 134-138
Thyrotoxic Valvulopathy: Case Report and Review of the Literature
Keniel Pierrea, Sushee Gaddea, Bassam Omara, b, G. Mustafa Awana, Christopher Malozzia
aDivision of Cardiology, University of South Alabama, Mobile, AL 36617, USA bCorresponding Author: Bassam Omar, Division of Cardiology, University of South Alabama, Mobile, AL 36617, USA
Manuscript submitted June 4, 2017, accepted June 8, 2017 Short title: Thyrotoxic Valvulopathy doi: https://doi.org/10.14740/cr564w
We report a 42-year-old female who was admitted for abdominal pain, and also endorsed dyspnea, fatigue and chronic palpitations. Past medical history included asthma, patent ductus arteriosus repaired in childhood and ill-defined thyroid disease. Physical examination revealed blood pressure of 136/88 mm Hg and heart rate of 149 beats per minute. Cardiovascular exam revealed an irregularly irregular rhythm, and pulmonary exam revealed mild expiratory wheezing. Abdomen was tender. Electrocardiogram revealed atrial fibrillation with rapid ventricular response which responded to intravenous diltiazem. Labs revealed TSH of < 0.1 mU/L and free T4 of 2.82 ng/dL, a positive TSH-receptor and thyroid peroxidase antibodies suggesting Grave’s thyrotoxicosis. A transthoracic echocardiogram reported an ejection fraction of 55-60%, with mild to moderate mitral regurgitation (MR) and moderate to severe tricuspid regurgitation (TR) and dilated right heart chambers. Pulmonary artery systolic pressure was 52 mm Hg. Transesophageal echocardiogram revealed a myxomatous tricuspid valve with thickening and malcoaptation of the leaflets and moderate to severe TR, mild to moderate MR with mild thickening of the mitral valve leaflets. Abdominal ultrasound revealed wall thickening of the gall bladder concerning for acute cholecystitis. She underwent laparoscopic cholecystectomy and was discharged in stable condition on methimazole for her thyroid disease, and on oral diltiazem for rate control and anticoagulation for atrial fibrillation. Follow-up visit with her cardiologist few months later documented absence of cardiac symptoms, and no murmurs were reported on physical examination. This case underscores the importance of maintaining a high index of suspicion for hyperthyroidism when faced with significant newly diagnosed pulmonary hypertension and TR, as treatment of the thyroid abnormalities can reverse these cardiac findings.
The effect of the thyroid on the cardiovascular system has been unequivocally demonstrated at the molecular, cellular and organ levels [1]. Wu et al [2] reported right heart enlargement and pulmonary hypertension in approximately 45% of 75 patients with thyrotoxicosis and heart disease. Brauman et al [3] reported a three-fold higher incidence of mitral valve prolapse (16.3%) in 126 patients with Grave’s disease compared to 111 healthy controls (5.4%). We present a case of a young female with significant tricuspid regurgitation (TR) associated with hyperthyroidism, together with review of pertinent literature.
A 42-year-old white female was admitted to our institution for evaluation of right upper quadrant (RUQ) abdominal pain, which worsened with food and was accompanied by intermittent nausea and vomiting. She also reported dyspnea on exertion, fatigue and chronic palpitations. Past medical history included asthma, patent ductus arteriosus repaired in childhood and ill-defined thyroid disease.
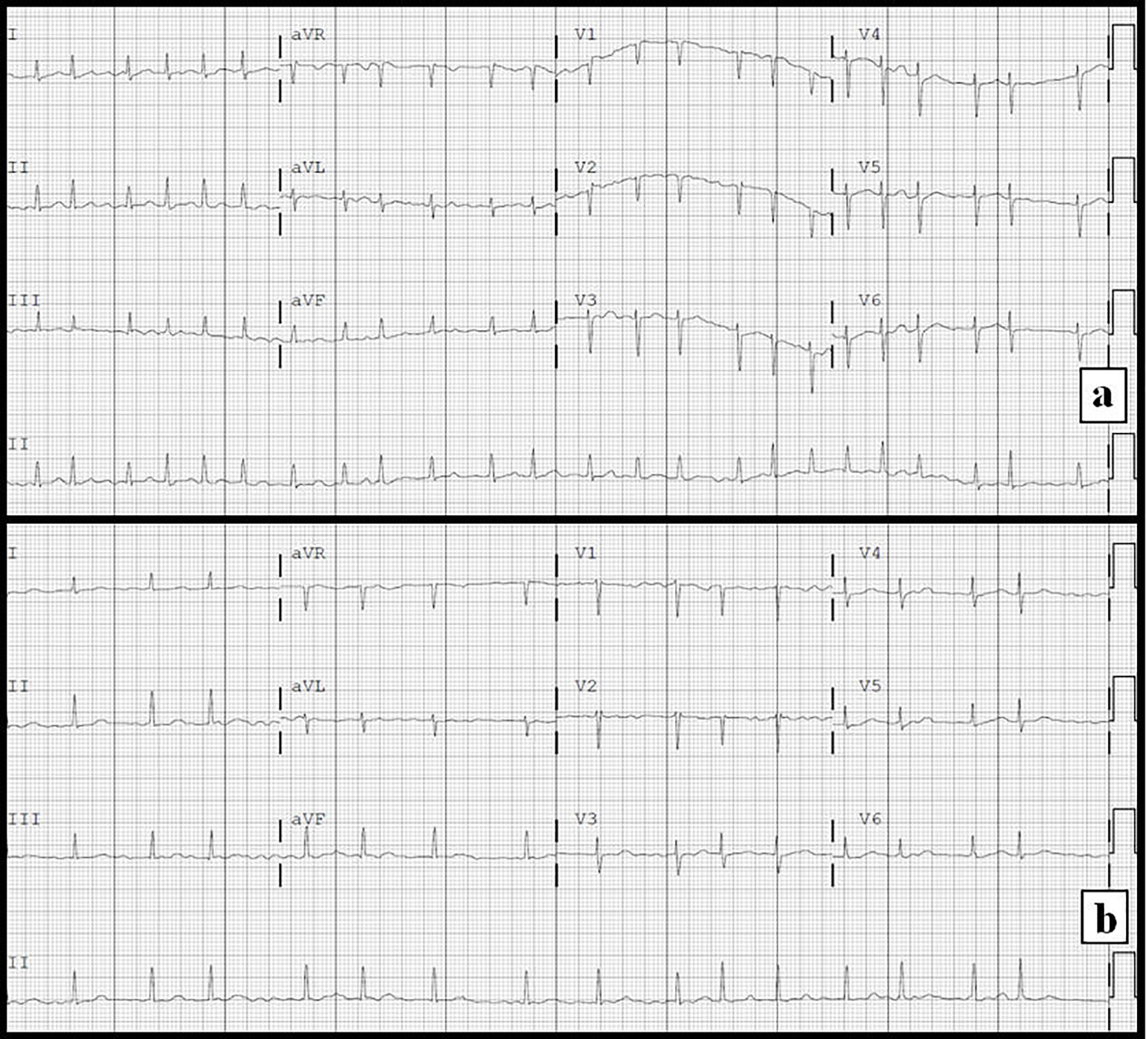
Physical examination revealed a blood pressure (BP) of 136/88 mm Hg and a heart rate (HR) of 149 beats per minute (bpm); she was afebrile. Cardiovascular exam revealed an irregularly irregular rhythm, and pulmonary exam revealed mild expiratory wheezing. Abdominal exam was positive for RUQ tenderness. Chest radiograph displayed no acute pathology. Electrocardiogram revealed atrial fibrillation with rapid ventricular response at 149 bmp (Fig. 1a). Laboratory investigations revealed a white blood cell count of 13,300/µL, creatinine of 0.78 mg/dL, troponin I of 0.05 ng/mL, TSH of < 0.1 mU/L and free T4 of 2.82 ng/dL. The patient received a loading dose of diltiazem 20 mg IV, and was initially placed on a diltiazem drip at 10 mg/h, and later transitioned to oral diltiazem with adequate HR control (Fig. 1b). Further thyroid studies revealed a positive TSH-receptor and thyroid peroxidase antibodies suggesting Grave’s thyrotoxicosis; therefore, she was started methimazole.
Figure 1. Electrocardiograms. (a) On admission demonstrating atrial fibrillation with rapid ventricular response. (b) Following administration of intravenous diltiazem demonstrating atrial fibrillation with a more controlled ventricular response.
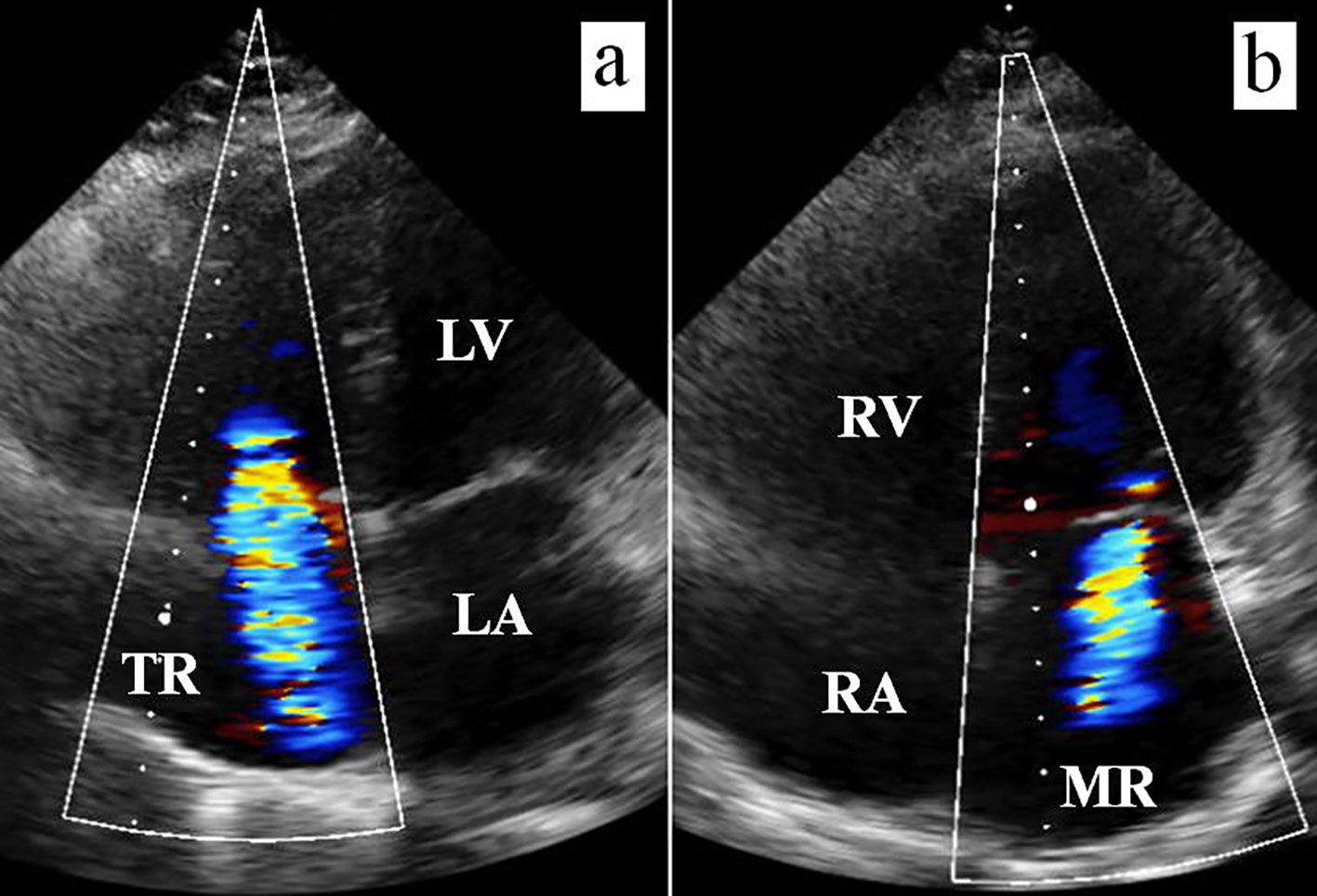
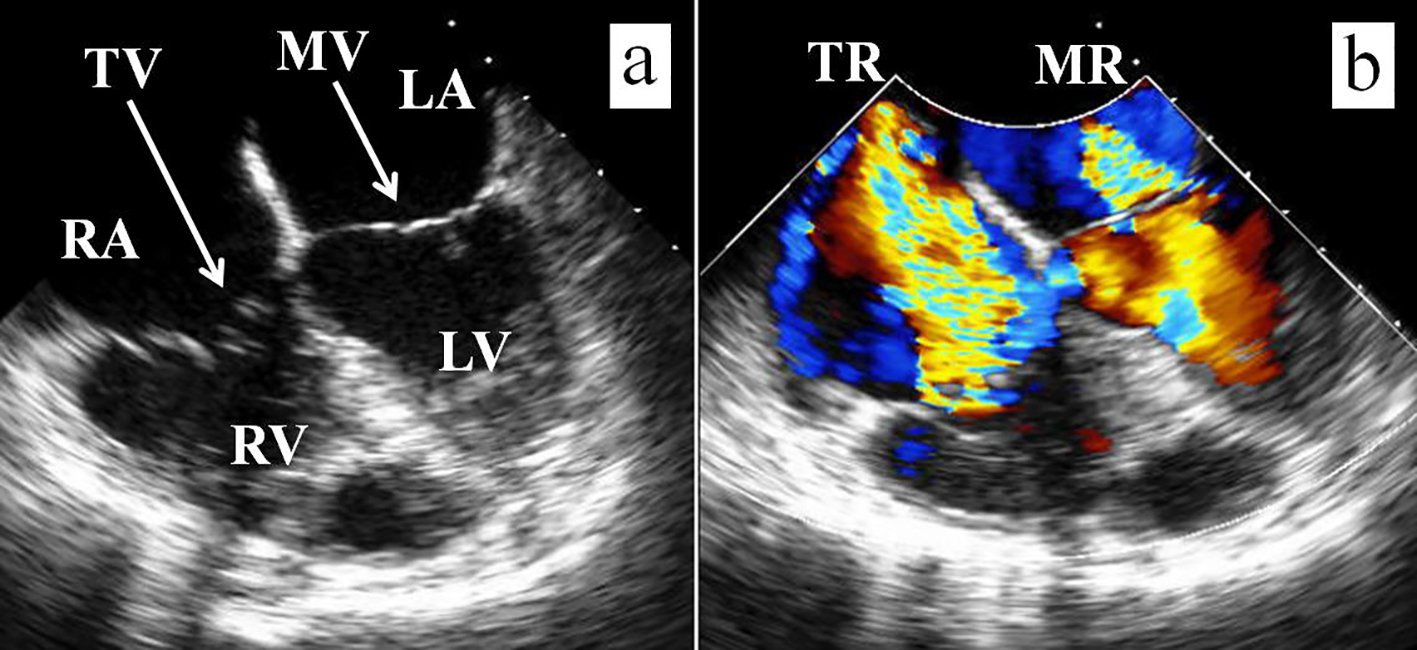
The patient underwent a transthoracic echocardiogram, which was technically difficult and reported an ejection fraction of 55-60%, with mild to moderate mitral regurgitation (MR) and moderate to severe TR with dilated right heart chambers (Fig. 2), a new finding compared to a prior echocardiographic study few years earlier. Pulmonary artery systolic pressure was elevated at 52 mm Hg. She underwent a transesophageal echocardiogram (Fig. 3) to further evaluate the valve abnormalities, and this revealed a myxomatous tricuspid valve with thickening and malcoaptation of the leaflets and moderate to severe TR; mild to moderate MR with mild thickening of the mitral valve leaflets was also noted. RUQ ultrasound revealed wall thickening of the gall bladder concerning for acute cholecystitis. She underwent uneventful laparoscopic cholecystectomy and was later discharged in stable condition on oral diltiazem for rate control and anticoagulation for atrial fibrillation, with outpatient follow-up of her thyroid abnormalities. Follow-up visit with her cardiologist few months later documented absence of cardiac symptoms, and no murmurs were reported on physical examination.
Figure 2. Transthoracic 2D echocardiographic images with color Doppler. (a) Color Doppler across the tricuspid valve demonstrating moderate to severe TR. (b) Color Doppler across the mitral valve demonstrating mild to moderate MR.
Figure 3. Transesophageal echocardiographic images. (a) Thickening and incomplete coaptation of the tricuspid valve leaflets compared with the mitral valve leaflets. (b) Color Doppler images demonstrate moderate to severe TR and mild to moderate MR.
Over 200 years ago, Dr. Caleb Parry, an English physician, was first to recognize the cardiovascular effects of hyperthyroidism [4]. Out of the myriad of systemic manifestations of Grave’s disease, our patient presented with a myxomatous tricuspid valve with significant TR.
TR in association with hyperthyroidism can be isolated or accompanied by pulmonary hypertension, and has been the subject of many case reports as will be detailed.
Dougherty and Craige [5] reported two elderly women with apathetic hyperthyroidism presenting with severe TR, which resolved following thyroid treatment. Iranzo Vazquez et al [6] reported a 60-year-old hyperthyroid female with heart failure attributed to severe TR, which resolved after adequate treatment of her hyperthyroidism. They suggested that when confronted with TR of unclear etiology, the possibility of hyperthyroidism must be investigated. Lozano and Sharma [7] reported a 29-year-old hyperthyroid female with heart failure symptoms for 4 weeks and severe TR (4+), whose symptoms and TR near completely resolved after thyroid therapy. Whitner et al [8] reported a previously healthy 43-year-old female who was evaluated for progressive lower extremity edema and was found to have hyperthyroidism and moderate to severe TR by echocardiography (echo); her symptoms and echo findings resolved following thyroid ablation. Park et al [9] reported a 71-year-old female with hyperthyroidism and heart failure who had severe TR due to incomplete systolic coaptation of the tricuspid leaflets causing pulmonary hypertension; her symptoms and echo findings resolved with heart failure and thyroid treatment. Ismail [10] reported a previously health 56-year-old female with a 3-month history of heart failure symptoms and Grave’s disease, found to have severe TR and severe pulmonic insufficiency on echo; her symptoms and echo findings improved after treatment with methimazole. Syriou et al [11] reported a 48-year-old female with resistant heart failure treated for several months, who had severe TR and pulmonary hypertension by echo; she was found to be hyperthyroid and her symptoms and echo findings resolved after adequate treatment of her hyperthyroidism. Saad et al [12] reported a 34-year-old female with Graves-Basedow disease who developed right-sided heart failure with severe TR, but no pulmonary hypertension, by echo, which resolved following appropriate medical therapy. Giovambattista [13] reported significant heart failure in a 54-year-old female with overt hypothyroidism found to have severe TR and pulmonary hypertension on echo; her symptoms and echo findings normalized after 6 weeks of antithyroid therapy. Bonou et al [14] reported a 34-year-old hyperthyroid female with 3 months of heart failure symptoms and severe TR due to incomplete systolic coaptation of the tricuspid valve leaflets, whose symptoms and echo findings did not completely resolve until 10 months of treatment, despite normalization of the thyroid function after the first month of therapy.
In patients with hyperthyroidism, TR has often been thought to be functional and caused by right ventricular dilatation secondary to increased venous return, as in many of the cases described above. However, our patient had a myxomatous tricuspid valve likely causing a combination of primary and secondary significant TR. Myxomatous degeneration is characterized by a markedly disordered appearance of collagen bundles leading to tissue that is more easily stretched and ruptured at lower stress than normal tissue [15]. Thyrotoxicosis, specifically Grave’s disease, has numerous documented effects on connective tissue. For example, Grave’s ophthalmopathy has been attributed to fibroblast growth and inflammatory cell infiltrates within the soft tissue of extraocular muscles [16]. Moreover, Grave’s dermopathy is caused by glycosaminoglycan deposition into the skin dermis [17]. Thus, thyrotoxicosis may also have a direct effect on the connective tissue of tricuspid valves leading to myxomatous degeneration. Kage et al [18] compared 24 Grave’s disease patients with age-matched controls and reported that patients with Grave’s disease had a higher prevalence of TR. The mitral valve can also be afflict by similar myxomatous changes resulting in significant primary MR due to leaflet prolapse [3], intrinsic papillary muscle dysfunction [19], chordal rupture [20], and in association with rheumatic valve disease [21] and secondary to heart failure [22].
The association between pulmonary hypertension and hyperthyroidism has been widely reported, with or without significant TR. Yanai-Landau et al [23] reported that 30% out of 40 patients with primary pulmonary hypertension were found to have antithyroglobulin antibodies. Marvisi et al [24] reported even a higher prevalence of pulmonary hypertension in newly diagnosed hyperthyroid patients compared with patients taking methimazole or those who were clinically euthyroid. The most intriguing aspect of this association is the resolution of these findings as a patient becomes clinically euthyroid, while other causes of heart failure are excluded or addressed, as illustrated in the previously described case reports and by other investigators [25-31]. While the exact mechanism of pulmonary hypertension in hyperthyroidism remains unclear, potential explanations include direct action of thyroid hormone at the plasma membrane and endoplasmic reticulum influencing the activity of Ca2+ ATPase and the transcellular flux of substrates and cations [24], autoimmune-mediated endothelial damage; endothelial injury caused by increased cardiac output, increased metabolism of intrinsic (prostacyclin and nitric oxide) and extrinsic (acetylcholine) pulmonary vasodilating substances [29], and impaired metabolism of vasoconstrictors including serotonin, endothelin 1, and thromboxane [25-29]. While pulmonary hypertension often coexists with significant TR, cases of isolated pulmonary hypertension have been reported in the presence of only mild to moderate TR [32].
Hyperthyroidism should be considered in the differential diagnosis not only of heart failure in general [33], but also in pulmonary hypertension and TR. While the prognosis of pulmonary hypertension remains poor and its treatment options continue to be limited, identification of associated thyroid disease is of paramount importance, as its treatment can lead to resolution of pulmonary hypertension.
The phenotype of Grave’s disease varies widely among patients. While symptoms of palpitations, weight loss and heat intolerance often dominate, other serious cardiopulmonary symptoms can have deleterious effects on patients’ health. Our patient demonstrated significant TR which was likely a combination of primary TR due to myxomatous degeneration of the leaflets, in addition to a secondary TR component related to the dilatation of the right heart chambers.
Conclusion
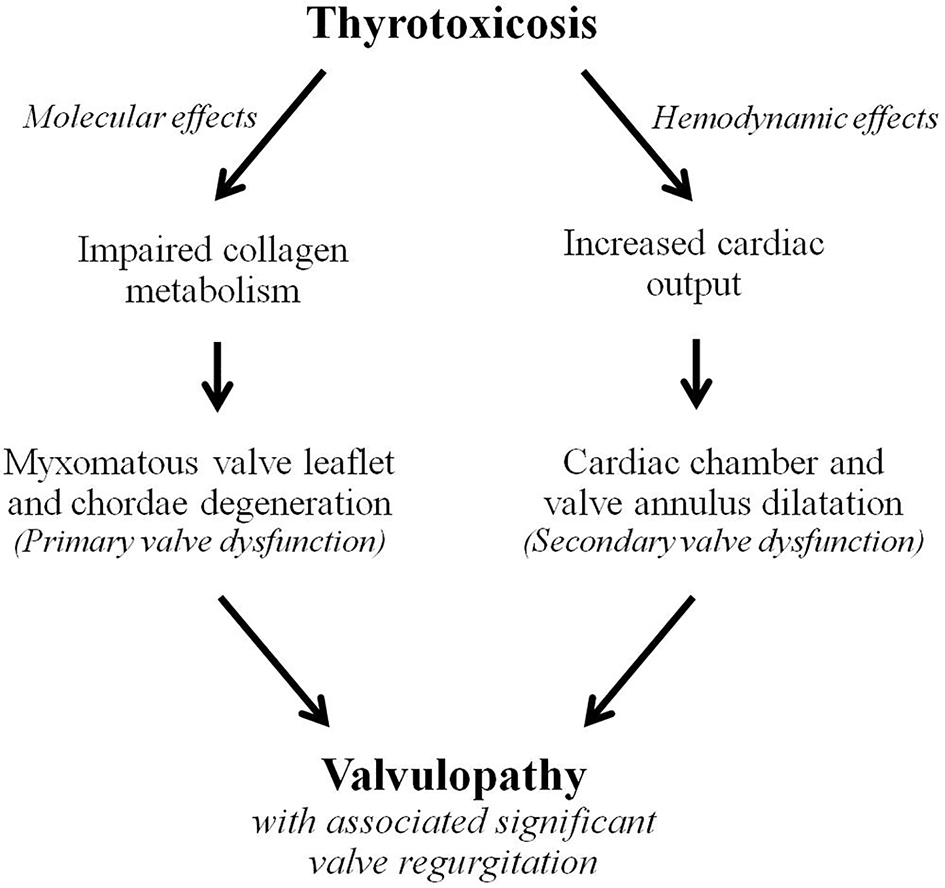
Hyperthyroidism has a myriad of systemic effects, and exerts many changes on the cardiovascular system. While some of these effects are related to the hemodynamic burden of a hyperdynamic circulation leading to cardiac chamber dilatation due to increased preload and volume overload, other important effects are direct degenerative changes on valve structures, including the leaflets and the subvalvular apparatus, leading to progressive and significant valvular insufficiency and further exacerbation of heart failure. Thyrotoxic valvulopathy should therefore be thought of as a combination of both secondary changes caused by cardiac chamber dilatation causing valve leaflet malcoaptation, and primary changes caused by a direct damaging effect on the valve structures, as we demonstrate in Figure 4. Such changes are being increasingly identified at the cellular level and may become a target for heart failure therapies in the future.
Figure 4. Schematic demonstrating the impact of thyrotoxicosis on cardiac valves through a combined effect of direct myxomatous valve degeneration causing primary valve insufficiency, and hemodynamic volume overload causing cardiac chamber dilatation and further valve incompetency.
Disclosures
All authors declare no disclosures related to this manuscript.
Klein I, Danzi S. Thyroid disease and the heart. Circulation. 2007;116(15):1725-1735. doipubmed
Wu HH, Guo XH, Gao YM. Clinical features of thyrotoxic heart disease: analysis of 75 cases. Zhonghua Yi Xue Za Zhi. 2007;87(4):262-264. pubmed
Brauman A, Algom M, Gilboa Y, Ramot Y, Golik A, Stryjer D. Mitral valve prolapse in hyperthyroidism of two different origins. Br Heart J. 1985;53(4):374-377. doipubmed
Skelton CL. The heart and hyperthyroidism. N Engl J Med. 1982;307(19):1206-1208. doipubmed
Dougherty MJ, Craige E. Apathetic hyperthyroidism presenting as tricuspid regurgitation. Chest. 1973;63(5):767-772. doi
Iranzo Vazquez D, Rius Riu F, Pizarro Lozano E, Lupon Roses J. [Severe tricuspid insufficiency as main manifestation of hyperthyroidism]. Rev Esp Cardiol. 1997;50(1):65-66. doi
Lozano HF, Sharma CN. Reversible pulmonary hypertension, tricuspid regurgitation and right-sided heart failure associated with hyperthyroidism: case report and review of the literature. Cardiol Rev. 2004;12(6):299-305. doipubmed
Whitner TE, Hudson CJ, Smith TD, Littmann L. Hyperthyroidism presenting as isolated tricuspid regurgitation and right heart failure. Tex Heart Inst J. 2005;32(2):244-245. pubmed
Park JH, Shong M, Lee JH, Choi SW, Jeong JO, Seong IW. Reversible severe tricuspid regurgitation with right heart failure associated with thyrotoxicosis. Thyroid. 2006;16(8):813-814. doipubmed
Ismail HM. Reversible pulmonary hypertension and isolated right-sided heart failure associated with hyperthyroidism. J Gen Intern Med. 2007;22(1):148-150. doipubmed
Syriou V, Plastiras SC, Paterakis T, Moyssakis I, Vlachoyiannopoulos P. Severe reversible right heart failure in a patient with hyperthyroidism. Int J Clin Pract. 2008;62(2):334-336. doipubmed
Saad AK, Pisarevsky AA, Gonzalez DR, Vazquez Blanco M, Petrucci E. [Young woman with hyperthyroidism associated with severe tricuspid regurgitation]. Medicina (B Aires). 2008;68(1):55-58.
Di Giovambattista R. Hyperthyroidism as a reversible cause of right ventricular overload and congestive heart failure. Cardiovasc Ultrasound. 2008;6:29. doipubmed
Bonou M, Lampropoulos KM, Andriopoulou M, Kotsas D, Lakoumentas J, Barbetseas J. Severe tricuspid regurgitation and isolated right heart failure due to thyrotoxicosis. Indian Heart J. 2012;64(6):600-602. doipubmed
Lim KO, Boughner DR, Perkins DG. Ultrastructure and mechanical properties of chordae tendineae from a myxomatous tricuspid valve. Jpn Heart J. 1983;24(4):539-548. doipubmed
Bahn RS. Graves' ophthalmopathy. N Engl J Med. 2010;362(8):726-738. doipubmed
Peacey SR, Flemming L, Messenger A, Weetman AP. Is Graves' dermopathy a generalized disorder? Thyroid. 1996;6(1):41-45. doipubmed
Kage K, Kira Y, Sekine I, Okabe F, Nakaoka T, Hashimoto E, Yamasaki M, et al. High incidence of mitral and tricuspid regurgitation in patients with Graves' disease detected by two-dimensional color Doppler echocardiography. Intern Med. 1993;32(5):374-376. doipubmed
Reynolds JL, Woody HB. Thyrotoxic mitral regurgitation: a probable form of intrinsic papillary muscle dysfunction. Am J Dis Child. 1971;122(6):544-548. doi
Aronson RJ, Hoffman M, Algueti-Margulis A, Yust I. Spontaneous rupture of mitral chordae tendineae in hyperthyroidism. Am J Cardiol. 1987;59(5):475-476. doi
Fujiwara T, Katsumura T, Doko S, Motohiro K, Inada H, Sato M, Kiso A, et al. [Rheumatic valvular disease associated with hyperthyroidism]. Nihon Kyobu Geka Gakkai Zasshi. 1983;31(8):1315-1319. pubmed
Cavros NG, Old WD, Castro FD, Estep HL. Case report: reversible mitral regurgitation and congestive heart failure complicating thyrotoxicosis. Am J Med Sci. 1996;311(3):142-144. doi
Yanai-Landau H, Amital H, Bar-Dayan Y, Levy Y, Gur H, Lin HC, Alosachie IJ, et al. Autoimmune aspects of primary pulmonary hypertension. Pathobiology. 1995;63(2):71-75. doipubmed
Marvisi M, Brianti M, Marani G, Del Borello R, Bortesi ML, Guariglia A. Hyperthyroidism and pulmonary hypertension. Respir Med. 2002;96(4):215-220. doipubmed
Marvisi M, Zambrelli P, Brianti M, Civardi G, Lampugnani R, Delsignore R. Pulmonary hypertension is frequent in hyperthyroidism and normalizes after therapy. Eur J Intern Med. 2006;17(4):267-271. doipubmed
Ma RC, Cheng AY, So WY, Hui DS, Tong PC, Chow CC. Thyrotoxicosis and pulmonary hypertension. Am J Med. 2005;118(8):927-928. doipubmed
Hegazi MO, El Sayed A, El Ghoussein H. Pulmonary hypertension responding to hyperthyroidism treatment. Respirology. 2008;13(6):923-925. doipubmed
Nakchbandi IA, Wirth JA, Inzucchi SE. Pulmonary hypertension caused by Graves' thyrotoxicosis: normal pulmonary hemodynamics restored by (131)I treatment. Chest. 1999;116(5):1483-1485. doipubmed
Virani SS, Mendoza CE, Ferreira AC, de Marchena E. Graves' disease and pulmonary hypertension: report of 2 cases. Tex Heart Inst J. 2003;30(4):314-315. pubmed
Xenopoulos NP, Braden GA, Applegate RJ. Severe right heart failure in a patient with Grave's disease. Clin Cardiol. 1996;19(11):903-905. doipubmed
Baptista A, Costa RP, Ferreira C, Mateus P, Trigo Faria A, Moreira I. [Pulmonary hypertension, heart failure and hyperthyroidism: a case report]. Rev Port Cardiol. 2013;32(3):253-256. doi
Biondi B. Mechanisms in endocrinology: Heart failure and thyroid dysfunction. Eur J Endocrinol. 2012;167(5):609-618. doipubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.