aDivision of Cardiology, Onassis Cardiac Surgery Center, Athens, Greece bLaboratory of Experimental Surgery and Surgical Research, University of Athens, Medical School, Athens, Greece cDepartment of Surgery, The Ohio State University Comprehensive Cancer Center, The Ohio State University, Columbus, OH, USA dCorresponding Author: Michael Spartalis, Division of Cardiology, Onassis Cardiac Surgery Center, Fokidos 42, Athens 115 27, Greece
Manuscript submitted June 6, 2017, accepted June 15, 2017 Short title: QAV, PFO and Stroke doi: https://doi.org/10.14740/cr567w
Quadricuspid aortic valve (QAV) is a rare congenital aortic valve abnormality. It is less common as compared to bicuspid or unicuspid aortic valve abnormality. QAV causes aortic regurgitation usually in the fifth to sixth decade of life. We present a rare case of a female patient with cryptogenic stroke due to a QAV and a patent foramen ovale (PFO). The patient underwent transcatheter closure of PFO, as there was no clear indication for surgery for her valve. Surgical removal remains the method of choice for the treatment of the QAV before left ventricular decompensation occurs.
A quadricuspid aortic valve (QAV) is a rare congenital abnormality of the aortic valve with an estimated prevalence of 0.008-1.46% [1]. The first case was reported in 1862 by Balington [2]. The most frequent complication of a quadricuspid valve is aortic insufficiency, while various comorbidities are coronary anomalies and aortic root dilation [3]. Other findings, including abnormalities of other heart valves, patent ductus arteriosus (PDA), septal defects and persistent left superior vena cava have also been reported in the literature [4, 5]. In our case, no anomalous origin of coronary arteries and aortic root dilation was found in the transesophageal examination, rather than a patent foramen ovale (PFO).
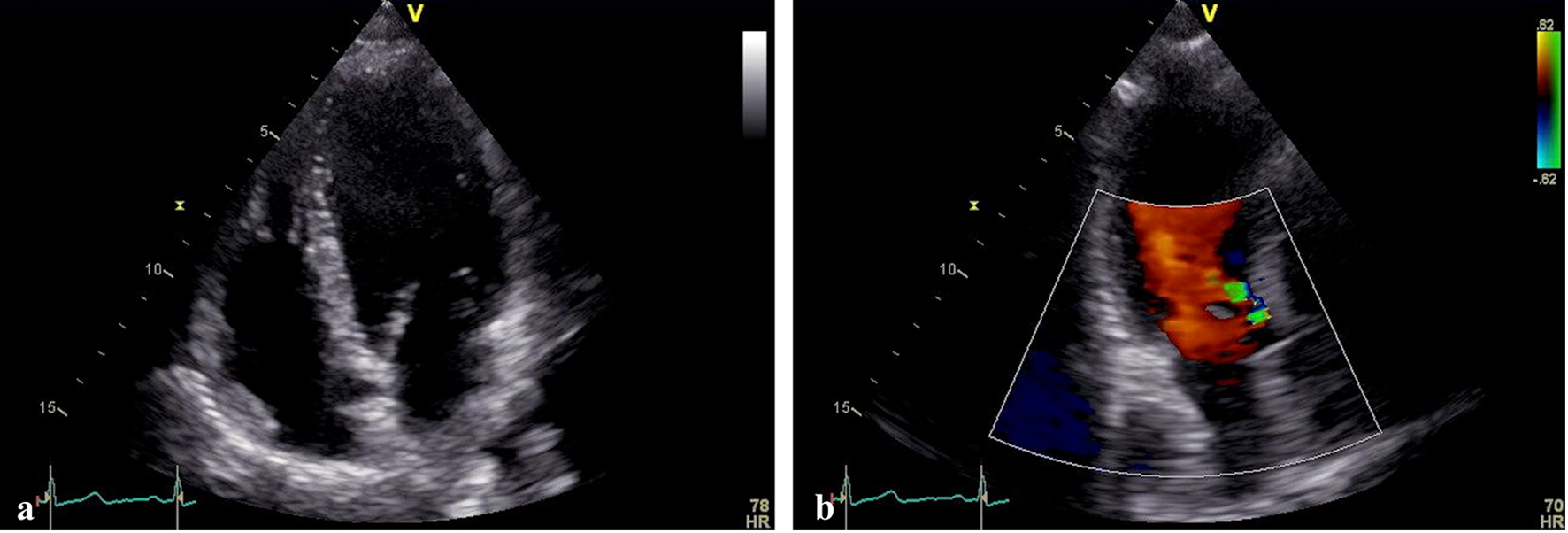
A 48-year-old Caucasian female was referred to our department with a history of stroke. The patient did not have a definitive cause of stroke. The echocardiographic evaluation showed a floppy interatrial septum, a mild aortic regurgitation (AR) and no other significant abnormalities (Fig. 1a, b). A QAV was suspected, so a transesophageal examination was scheduled to assess the severity of the AR and the structural integrity of the interatrial septum. The aortic valve was quadricuspid (type B) with mild AR, and the aortic root measurement was 28 mm (Fig. 2a, b). For further evaluation of our patient, contrast echocardiography was conducted and confirmed our suspicion of a PFO with a small left to right shunt (Fig. 3a, b). The patient did not have a surgical indication and proceeded for percutaneous occlusion of PFO.
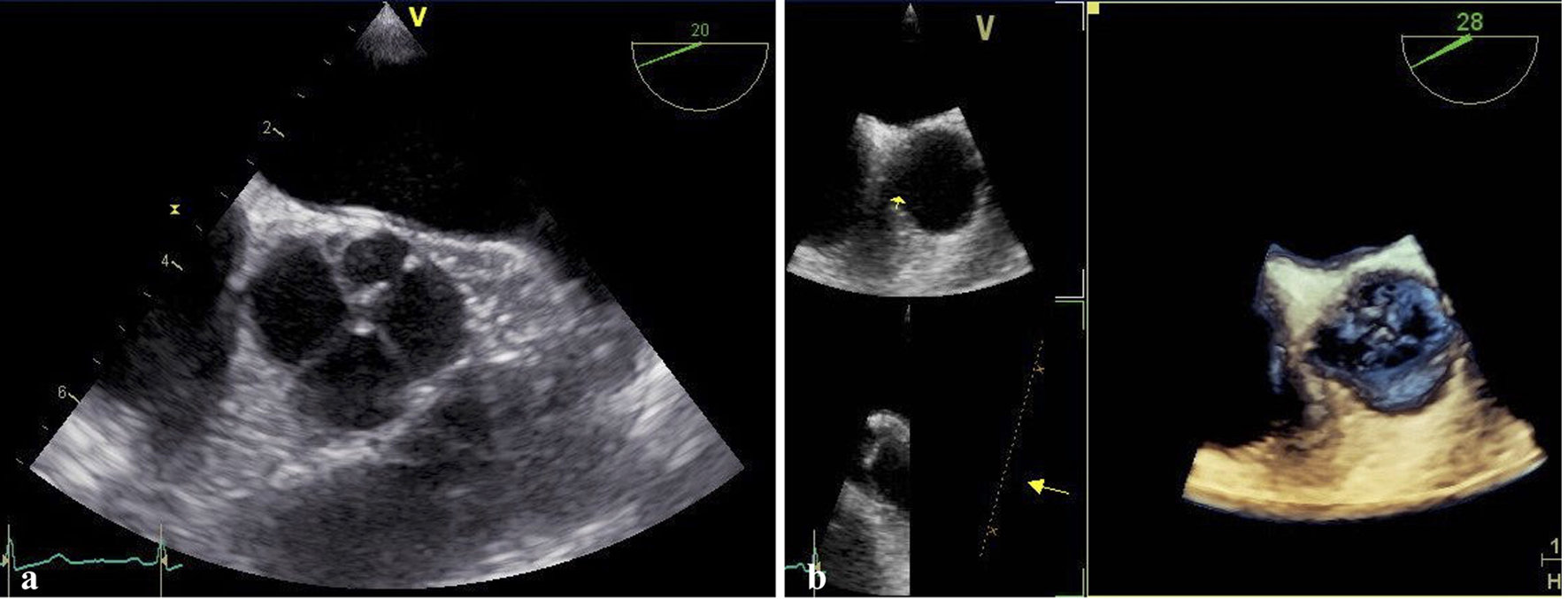
Figure 2. (a) Transesophageal echocardiography showing an aortic valve with four cusps (left coronary cusp, right coronary cusp, non-coronary cusp and accessory cusp). (b) 3D echocardiography showing an aortic valve with four cusps (left coronary cusp, right coronary cusp, non-coronary cusp and accessory cusp).
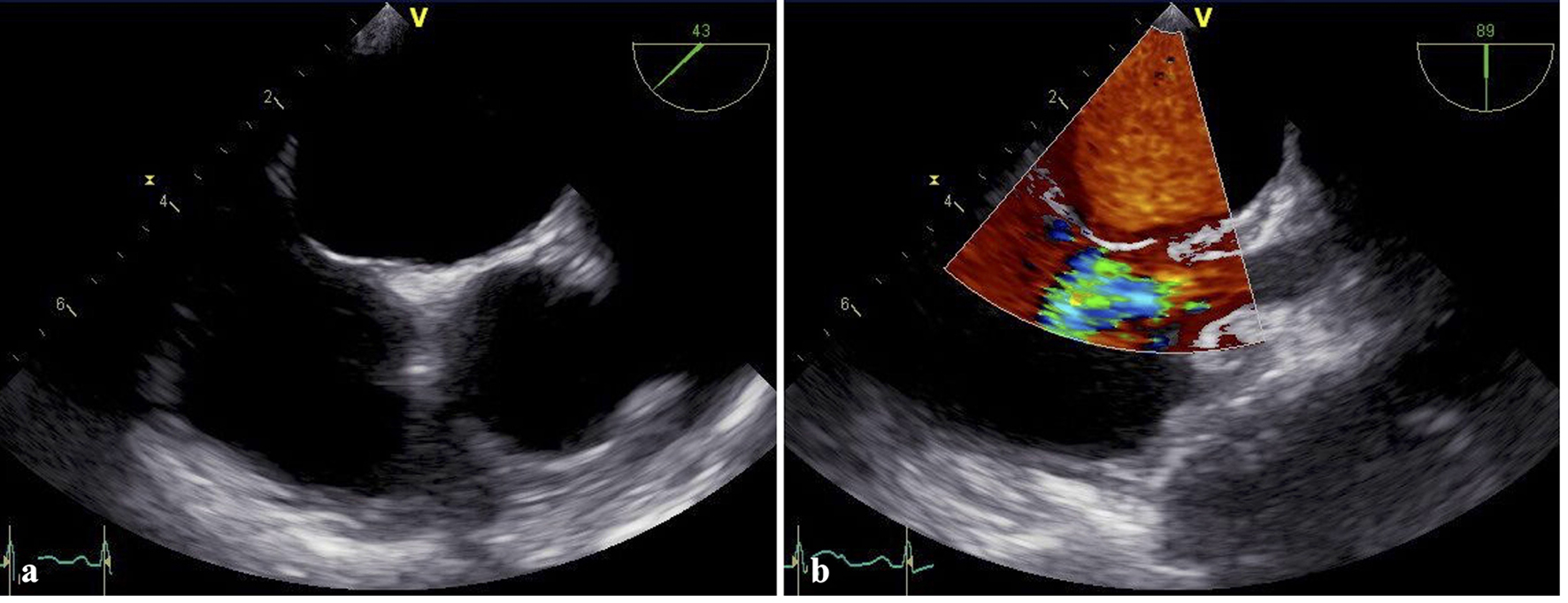
Figure 3. (a) Transesophageal echocardiography demonstrating a flap-like structure between the atrial septa primum and secundum at the position of the fossa ovalis (patent foramen ovale). (b) Transesophageal echocardiography with continuous wave Doppler signal detecting blood flow between the left atrium and right atrium.
QAV is defined by two classifications. Hurwitz and Roberts divide QAV into seven categories in accordance with the relative size of the four cusps. The most frequent form has three cusps of equal size and one smaller cusp (type B) [6]. Nakamura et al classify QAV according to the location of the supernumerary cusp. The most frequent is type B like in our case, in which the supernumerary cusp is positioned between the non-coronary cusp and the right coronary cusp [7].
A QAV mostly presents as an isolated congenital abnormality, but can also be found with different anomalies, such as ventricular septal defect (VSD), PDA, pulmonary valve stenosis, subaortic muscular stenosis and defects of the coronary arteries [5]. We present a novel case of a patient with QAV and PFO, which has never been reported in the literature [4, 5, 8].
QAV generally has a normal function when the patient is under 18 years of age and starts deteriorating over 40 years of age [5]. Clinical presentation varies from asymptomatic to various symptomatology like palpitations, chest discomfort, dyspnea, congestive heart failure, fatigue, syncope and even sudden cardiac death [5]. There is only one paper published reporting of a QAV manifested with ischemic stroke [9]. The involvement of PFO in the genesis of cryptogenic stroke is well established, and current guidelines suggest a transcatheter occlusion of PFO as a secondary prevention [10]. Is QAV or the PFO the lead cause of stroke in our case?
QAV has the tendency to develop to AR, due to gradual leaflet fibrosis and advanced failure of leaflet coaptation with aging [1]. Calcific valve disease of the left heart valves is classified as “low embolic risk” according to current guidelines. Nonetheless, it remains an important risk factor for cardiovascular events, including ischemic stroke [8].
The surgical indications for QAV are severe AR, severe aortic stenosis and dysfunctional valve with coronary ostium occlusion [5]. The replacement of the aortic valve with surgery is the procedure of choice for patients with QAV and AR, but there are also some reports of transcatheter aortic valve replacements [1]. The possibility of a third-degree atrioventricular block is probably elevated after valve replacement because the supernumerary cusp is usually positioned between the non-coronary cusp and the right coronary cusp, over the membranous septum [11].
The selection of patients and the treatment of choice are crucial because not all the patients with QAV require surgery [5]. Controversy remains over the strategic management of the patients with a QAV regarding indications for surgery, the treatment of choice and antibiotic administration as a precaution to prevent infective endocarditis [5]. Aortic valve regurgitation is the predominant hemodynamic abnormality and the main indication for aortic valve replacement in most patients who received surgery [4]. All patients with QAV require close surveillance for progression of AR.
Our patient underwent transcatheter closure of PFO, as there was no clear indication for surgery for her valve at this moment. A close echocardiographic follow-up was suggested to monitor the aortic insufficiency.
Conclusions
This case reports for the first time a female patient with a QAV and PFO, which manifested with an ischemic stroke. Clear delineation of the anatomy of the valve is difficult but of an immense clinical importance as these patients may develop progressive AR and other cardiovascular abnormalities, which will require cardiothoracic surgery. Surgical removal remains the method of choice for the treatment of QAV.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Financial Support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of Interest
No author has any conflicts of interest to disclose.
Hayakawa M, Asai T, Kinoshita T, Suzuki T. Quadricuspid aortic valve: a report on a 10-year case series and literature review. Ann Thorac Cardiovasc Surg. 2014;20(Suppl):941-944. doipubmed
Balington J. London Medical Gazette, July 1862.
Gu J, Qin C, Wu Z. Quadricuspid aortic valve with D (Rho) antigen negativity: a novel case report. Anatol J Cardiol. 2017;17(2):164. pubmed
Tutarel O. The quadricuspid aortic valve: a comprehensive review. J Heart Valve Dis. 2004;13(4):534-537. pubmed
Hurwitz LE, Roberts WC. Quadricuspid semilunar valve. Am J Cardiol. 1973;31(5):623-626. doi
Nakamura Y, Taniguchi I, Saiki M, Morimoto K, Yamaga T. Quadricuspid aortic valve associated with aortic stenosis and regurgitation. Jpn J Thorac Cardiovasc Surg. 2001;49(12):714-716. doipubmed
Aboitiz-Rivera CM, Blachman-Braun R, Lanza MF, Berebichez-Fridman R, Diaz-Huizar MJ, Ferrer-Arellano LG, Ramirez-Freyre AA, et al. Quadricuspid aortic valve: an unexpected echocardiographic finding. Med Ultrason. 2016;18(2):250-252. doipubmed
Krisper M, Kohncke C, Escher F, Morris DA, Tschope C, Pieske B. A patient with quadricuspid aortic valve and ischemic stroke. J Heart Valve Dis. 2016;25(4):456-458. pubmed
De Vecchis R, Baldi C, Cantatrione S. Transcatheter closure of PFO as secondary prevention of cryptogenic stroke. Herz. 2017;42(1):45-50. doipubmed
Pirundini PA, Balaguer JM, Lilly KJ, Gorsuch WB, Taft MB, Cohn LH, Rizzo RJ. Replacement of the quadricuspid aortic valve: strategy to avoid complete heart block. Ann Thorac Surg. 2006;81(6):2306-2308. doipubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.