

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Case Report
Volume 8, Number 5, October 2017, pages 254-257
A Novel Technique for the Administration of Sub-Ambient Oxygen in the Operating Room
Asad A. Khawajaa, Marco Corridoreb, c, Joseph D. Tobiasb, c, d
aMarshall University, Joan C. Edwards School of Medicine, Huntington, WV, USA
bDepartment of Anesthesiology and Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA
cDepartment of Anesthesiology and Pain Medicine, The Ohio State University, Columbus, OH, USA
dCorresponding Author: Joseph D. Tobias, Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, 700 Children’s Drive, Columbus, OH 43205, USA
Manuscript submitted September 6, 2017, accepted September 18, 2017
Short title: Anesthesia and Sub-Ambient Oxygen
doi: https://doi.org/10.14740/cr608w
| Abstract | ▴Top |
Hypoplastic left heart syndrome (HLHS) is a common form of congenital heart disease with abnormal development of left-sided structures of the heart. As excessive pulmonary blood flow is common prior to palliative surgical procedures, therapeutic maneuvers may be required to decrease pulmonary blood flow and augment systemic cardiac output. Respiratory manipulations to optimize the ratio of pulmonary to systemic blood flow may include techniques to induce hypercarbia or the delivery of sub-ambient concentrations of oxygen (FiO2 less than 0.21). We present a neonate with HLHS who required intraoperative care during a stage I hybrid procedure. Options for the intraoperative administration of a sub-ambient concentration of oxygen are presented.
Keywords: HLHS; Sub-ambient oxygen; Anesthesia
| Introduction | ▴Top |
Hypoplastic left heart syndrome (HLHS) is a complex form of congenital heart disease (CHD) with abnormal or under-development of left-sided cardiac structures. There is frequently accompanying stenosis and/or atresia of the mitral and aortic valves. These structural defects result in impaired systemic circulation once the patent ductus arteriosus (PDA) closes [1]. When the PDA is present, the distribution of cardiac output to either the pulmonary or systemic circulation remains dependent on the regional differences in the vascular resistance of the two circulations [2-4]. Output to the systemic and pulmonary circulations is delivered from a single right ventricle connected in parallel and thus the distribution of blood flow depends on the ratio of the resistance between the two. Given the mixing of the systemic and pulmonary venous return, systemic oxygen saturations are generally 75% when the distribution to the pulmonary and systemic beds is equivalent (Qp/Qs = 1). As the pulmonary resistance decreases during the post-natal course, excessive pulmonary blood flow with a high systemic oxygen saturation and inadequate systemic oxygen delivery manifested by an increasing lactic acid concentration may occur [5-7]. Various therapeutic options may be implemented to augment hypoxic pulmonary vasoconstriction (HPV) to sustain a higher pulmonary vascular tone and augment cardiac output to the systemic circulation. In general, two respiratory principles may be implemented to limit pulmonary blood flow including the administration of a sub-ambient inspired oxygen concentration (FiO2) or increasing the partial pressure of carbon dioxide (PaCO2) in the blood via hypoventilation or the administration of inspired carbon dioxide (2-5% FiCO2) [2, 8-10]. We present a neonate with HLHS who required intraoperative care during a stage I hybrid procedure [11]. Options for the intraoperative administration of a sub-atmospheric concentration of oxygen are presented.
| Case Report | ▴Top |
Institutional Review Board approval is not required at Nationwide Children’s Hospital (Columbus, OH) for the presentation of single case reports. The patient was a 2.2-kg, 7-day-old infant who was born with complex single ventricle anatomy including a double inlet left ventricle, hypoplastic right heart with d-transposition of the great arteries, a small ventricular septal defect, and extreme aortic arch hypoplasia. The maternal history was positive for substance abuse and urine toxicology at birth was positive for cannabinoids, opioids, methamphetamines, tricyclic antidepressants, and cocaine. Given the patient’s small birth weight and significant hemodynamic instability, he was judged to be a poor candidate for the Norwood procedure. Therefore, it was decided to proceed with hybrid palliation with a stage I procedure to include placement of bilateral pulmonary artery bands and stenting of the PDA. Prior to surgery, the patient was breathing spontaneously in an oxygen hood with nitrogen blended to maintain the FiO2 at 0.17 - 0.18. Inotropic support included milrinone 0.25 µg/kg/min along with prostaglandin E1 at 0.025 µg/kg/min to maintain ductal PDA. Under these conditions, the patient’s serum lactic acid concentration was stable in the 2 - 3 mmol/L range (normal ≤ 2 mmol/L) with a sub-ambient FiO2 at 0.17 - 0.18. When the FiO2 was ≥ 0.21, there was a concomitant increase in the serum lactic acid concentration into the range of 4.5 - 7.6 mmol/L. The patient’s preoperative American Society of Anesthesiologists’ physical classification was 4. Given his critical hemodynamic status, the patient was nil per os. Vascular access included an umbilical artery catheter, an umbilical vein catheter, a left femoral percutaneously inserted central catheter (PICC), and a peripheral intravenous cannula. The patient was transported to the operating room and standard American Society of Anesthesiologists’ monitors were placed. Given his inability to tolerate an oxygen concentration ≥ 0.21, the decision was made to induce and maintain anesthesia at a sub-ambient FiO2 ≤ 0.21. The options for such care are discussed in more details in the discussion section. Normally, the anesthetic oxygen and nitrous flow meters on the anesthesia machine are coupled (proportioning system) to ensure that FiO2 cannot decrease below 0.25 - 0.30 (Fig. 1). Therefore, prior to anesthetic care, the anesthetic machine was adjusted to deliver a hypoxic gas mixture by uncoupling the oxygen and nitrous flow meters. This was done by physically removing the chain that links the oxygen and nitrous flow meters (Fig. 1). Anesthesia was induced and maintained by a combined inhaled-intravenous technique with the inhalation of sevoflurane in a sub-ambient concentration of oxygen (FiO2 0.15 - 0.19) and the intravenous administration of fentanyl (5 µg/kg). The sub-ambient oxygen concentration was achieved by using the air and nitrous oxygen flow meters to deliver the desired FiO2. Bag-valve-mask ventilation was provided without difficulty and rocuronium (1 mg/kg) was administered to provide neuromuscular blockade and facilitate endotracheal intubation. The FiO2 and the systemic oxygen saturation by pulse oximetry during the preoperative and intraoperative times are listed in Table 1. Following the induction of anesthesia and endotracheal intubation, the patient was placed in a supine position with his arms tucked to the side. Anesthesia was maintained with isoflurane (expired concentration 0.2-0.4%) in air and nitrous oxide to maintain the FiO2 at 0.13 - 0.17. No hemodynamic response was noted to surgical incision. The operative procedure lasted 131 min. Along the ductus arteriosus, a large hematoma was noted, which precluded placement of the PDA stent. Therefore, only bilateral pulmonary artery bands (3 mm) were placed after which the FiO2 was brought back to 0.21 by discontinuing the nitrous oxide. Given the aortic arch anatomy and preoperative concerns, it was decided to continue prostaglandin therapy. At the completion of the surgical procedure, the patient’s trachea was extubated and he was transported to the cardiothoracic intensive care unit (CTICU), breathing spontaneously with a native airway. His postoperative course was unremarkable. Postoperative medications and fluids were infused as they were pre-operatively. Approximately 1.5 months later, the patient was taken back to the operating room for a Norwood procedure following weight gain and a substantial improvement in his general status. Postoperative extracorporeal membrane oxygenation (ECMO) was required for cardiorespiratory support. ECMO support was eventually weaned and the patient transitioned to conventional mechanical ventilation. His trachea was eventually extubated. He continues to be followed by the Cardiology Service at Nationwide Children’s Hospital.
 Click for large image | Figure 1. The Datex-Ohmeda Aestiva 5 anesthesia machine that was used to deliver the sub-ambient oxygen gas mixture. The chain or proportioning mechanism (white arrow) which connects the oxygen and nitrous oxide flow meters was removed so that nitrous oxide could be administered with air to deliver an FiO2 less than 0.21. These modifications are not recommended by the manufacturer of the anesthesia machine. |
 Click to view | Table 1. Oxygen Saturation and FiO2 During the Procedure |
| Discussion | ▴Top |
Regardless of the surgical option undertaken to treat HLHS, the therapeutic goals are to provide unobstructed systemic cardiac output, a controlled source of pulmonary blood flow, reliable coronary blood flow, adequate arterial and venous mixing at the atrial level, and unrestricted pulmonary venous drainage. Current options for HLHS include the Norwood procedure, the hybrid procedure or cardiac transplantation. Prior to surgical intervention and following the Norwood procedure, the control of pulmonary blood flow remains a key component in the care of these patients. By limiting pulmonary blood flow, there is a redistribution of cardiac output with an increase in systemic blood flow. Simple respiratory maneuvers can facilitate this process including a reduction of the FiO2 to reduce arterial oxygen or the induction of hypercarbia [12, 13]. Hypercarbia can be achieved by altering ventilation strategies (deliberate hypoventilation) or by adding carbon dioxide to the inspired gas mixture [8, 14, 15]. Although hypercarbia augments HPV thereby decreasing pulmonary blood flow, disadvantages of this therapy include the need for airway control with endotracheal intubation, stimulation of respiratory drive with a secondary increase in minute ventilation unless pharmacologic paralysis or sedation is used, systemic acidosis until compensatory mechanisms compensate for the respiratory acidosis, and stimulation of the sympathetic nervous system with hemodynamic effects.
The addition of nitrogen to the inhaled gas mixture to lower the FiO2 can be accomplished without the need for endotracheal intubation and without some of the other deleterious physiologic effects of hypercarbia. When the decision is made to deliver sub-atmospheric FiO2 to the patient, there are various options that have been described in clinical practice. As was demonstrated with our patient during the preoperative period, in the spontaneously breathing patient with a native airway, a standard oxygen hood can be used. To deliver the sub-ambient oxygen, a standard oxygen blender which is usually used to blend air and oxygen can be modified to blend air and nitrogen or oxygen and nitrogen (Fig. 2). Alternatively, nitrogen is added to the inspiratory limb of the delivery system to dilute the inspired gas and achieve the desired FiO2. To ensure patient safety, systemic oxygen saturation is monitored using pulse oximetry. Pulse oximeters may have decreased accuracy at lower oxygen saturations and have been shown to generally overestimate arterial oxyhemoglobin saturation at these low SaO2 levels (65-75%), resulting in a poor precision (high standard deviation) and low accuracy with a bias (SpO2 - SaO2) of about 5% [16]. This discrepancy may vary based on the manufacturer and type of pulse oximeter [16]. In addition to pulse oximetry, tissue and cerebral oxygenation can be measured using near infrared spectroscopy and may be helpful in continuously monitoring oxygen delivery, cardiac output, and tissue oxygenation [17, 18].
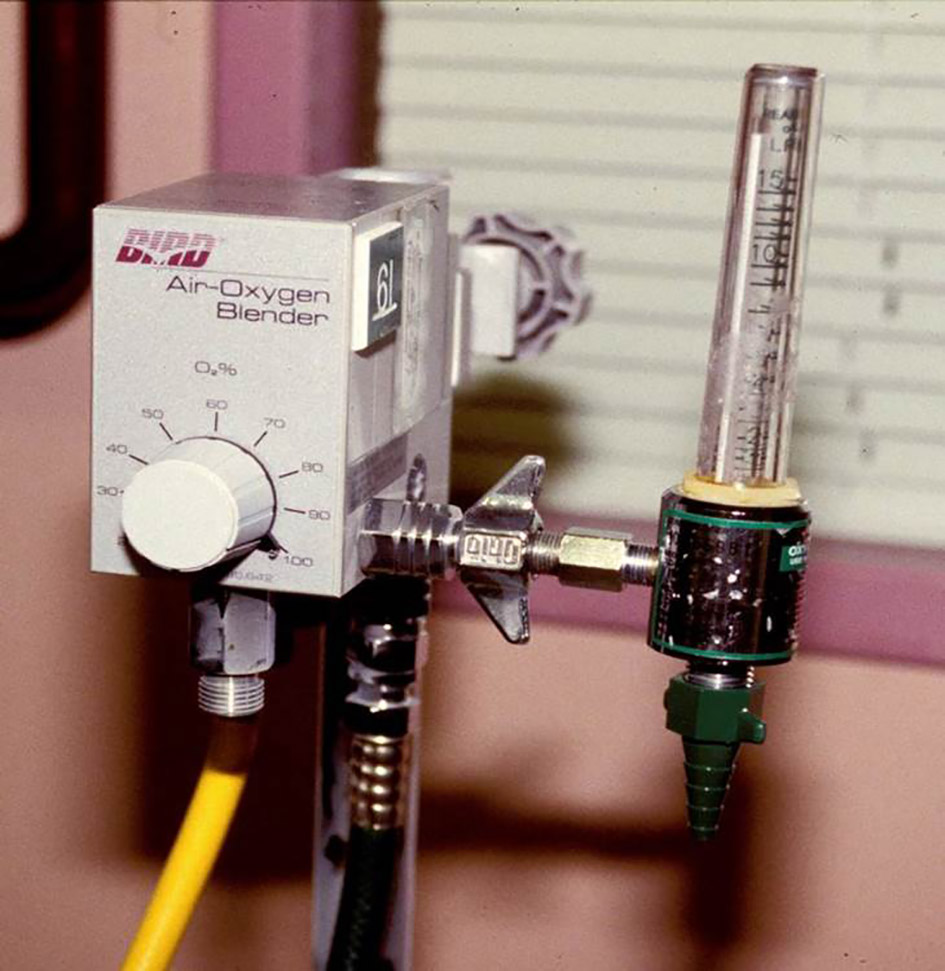 Click for large image | Figure 2. Standard oxygen blender for the administration of various concentrations of oxygen. The blender mixes oxygen (green hose) and air (yellow hose). In specific clinical scenarios, this blender can be modified to deliver a sub-ambient oxygen concentration to a hood by modification of the air hose so that it can be attached to a nitrogen tank. When this is done, it is mandatory to monitor the systemic oxygen saturation of the patient (pulse oximetry) and the inspired gas concentration to avoid morbidity and mortality from the administration of a hypoxic gas mixture. |
During mechanical ventilation, a sub-ambient FiO2 is generally achieved by adding a low flow of nitrogen from a large G cylinder (100% nitrogen) into the inspiratory limb of the ventilator circuit. The FiO2 is then measured distal to the point where the nitrogen is added prior to the patient’s ETT. However, as the gas (nitrogen) is added distal to the ventilator, alterations in minute ventilation will affect the FiO2 unless there is also a concomitant change in the flow of the added gas [19]. Nitrogen (100% concentration from a tank) is not routinely administered in inspiratory gas mixtures, but rather is used to power surgical equipment. It is supplied in high-pressure cylinders with an extremely high PSI and therefore down-regulators are required to ensure that nitrogen is delivered at an appropriate pressure.
Given these concerns, we decided to proceed with a different technique for intraoperative care. The anesthesia machine has a proportioning system in which the O2 and nitrous oxide (N2O) flow meters are coupled together in such a way that the administration of an FiO2 less than 0.30 is not feasible [20]. The two flow meters are coupled by a simple chain (Fig. 1). Therefore, an unmodified anesthesia machine could not be used to reduce the FiO2 to the concentration required by our patient. By uncoupling the oxygen and nitrous flow meters in the anesthetic machine, a gas mixture with an FiO2 ≤ 0.21 could be provided to the patient while allowing use of all of the other functions of the anesthesia machine including the inspired oxygen concentration monitor. Furthermore, changes in the minute ventilation did not affect the FiO2 with careful monitoring of FiO2. As the actual inspired concentration of N2O was less than 25%, no systemic effects were seen even in this compromised patient [21]. Modification of the anesthesia machine is not routinely recommended and should only be done in consultation with departmental leadership and operating room equipment support teams. Such modifications are not endorsed or recommended by the manufacturers of the anesthesia machine. Following such use, the machine should be removed from clinical care and rechecked by the biomedical engineering staff to ensure that the modification has been successfully reversed and that the machine has been returned to standards for intraoperative care.
In summary, we present a unique method for the administration of a sub-ambient FiO2 to facilitate the intraoperative care of a 7-day-old infant with HLHS. To limit pulmonary blood flow, a sub-ambient oxygen concentration may be needed to augment HPV and augment systemic cardiac output. We present a unique modification of the anesthesia machine with removal of the proportioning system to allow for the administration of a low concentration of nitrous oxide to dilute the fresh gas flow of air (FiO2 0.21) to achieve the desired sub-ambient FiO2. This system avoids some of the technical issues involved with the addition of nitrogen to the inspiratory limb of the ventilator circuit.
| References | ▴Top |
- Grossfeld PD. Hypoplastic left heart syndrome: it is all in the genes. J Am Coll Cardiol. 2007;50(16):1596-1597.
doi pubmed - Shime N, Hashimoto S, Hiramatsu N, Oka T, Kageyama K, Tanaka Y. Hypoxic gas therapy using nitrogen in the preoperative management of neonates with hypoplastic left heart syndrome. Pediatr Crit Care Med. 2000;1(1):38-41.
doi pubmed - Yabek SM, Mann JS. Prostaglandin E1 infusion in the hypoplastic left heart syndrome. Chest. 1979;76(3):330-331.
doi - Hansen DD, Hickey PR. Anesthesia for hypoplastic left heart syndrome: use of high-dose fentanyl in 30 neonates. Anesth Analg. 1986;65(2):127-132.
pubmed - Bailey LL, Gundry SR. Hypoplastic left heart syndrome. Pediatr Clin North Am. 1990;37(1):137-150.
doi - Barnea O, Austin EH, Richman B, Santamore WP. Balancing the circulation: theoretic optimization of pulmonary/systemic flow ratio in hypoplastic left heart syndrome. J Am Coll Cardiol. 1994;24(5):1376-1381.
doi - Feinstein JA, Benson DW, Dubin AM, Cohen MS, Maxey DM, Mahle WT, Pahl E, et al. Hypoplastic left heart syndrome: current considerations and expectations. J Am Coll Cardiol. 2012;59(1 Suppl):S1-42.
doi pubmed - Day RW, Barton AJ, Pysher TJ, Shaddy RE. Pulmonary vascular resistance of children treated with nitrogen during early infancy. Ann Thorac Surg. 1998;65(5):1400-1404.
doi - Jobes DR, Nicolson SC, Steven JM, Miller M, Jacobs ML, Norwood WI, Jr. Carbon dioxide prevents pulmonary overcirculation in hypoplastic left heart syndrome. Ann Thorac Surg. 1992;54(1):150-151.
doi - Chang AC, Zucker HA, Hickey PR, Wessel DL. Pulmonary vascular resistance in infants after cardiac surgery: role of carbon dioxide and hydrogen ion. Crit Care Med. 1995;23(3):568-574.
doi pubmed - Galantowicz M, Cheatham JP, Phillips A, Cua CL, Hoffman TM, Hill SL, Rodeman R. Hybrid approach for hypoplastic left heart syndrome: intermediate results after the learning curve. Ann Thorac Surg. 2008;85(6):2063-2070; discussion 2070-2061.
- Tabbutt S, Ramamoorthy C, Montenegro LM, Durning SM, Kurth CD, Steven JM, Godinez RI, et al. Impact of inspired gas mixtures on preoperative infants with hypoplastic left heart syndrome during controlled ventilation. Circulation. 2001;104(12 Suppl 1):I159-164.
doi pubmed - Ramamoorthy C, Tabbutt S, Kurth CD, Steven JM, Montenegro LM, Durning S, Wernovsky G, et al. Effects of inspired hypoxic and hypercapnic gas mixtures on cerebral oxygen saturation in neonates with univentricular heart defects. Anesthesiology. 2002;96(2):283-288.
doi pubmed - Mora GA, Pizarro C, Jacobs ML, Norwood WI. Experimental model of single ventricle. Influence of carbon dioxide on pulmonary vascular dynamics. Circulation. 1994;90(5 Pt 2):II43-46.
pubmed - Riordan CJ, Randsbeck F, Storey JH, Montgomery WD, Santamore WP, Austin EH, 3rd. Effects of oxygen, positive end-expiratory pressure, and carbon dioxide on oxygen delivery in an animal model of the univentricular heart. J Thorac Cardiovasc Surg. 1996;112(3):644-654.
doi - Ross PA, Newth CJ, Khemani RG. Accuracy of pulse oximetry in children. Pediatrics. 2014;133(1):22-29.
doi pubmed - Tobias JD. Cerebral oximetry monitoring with near infrared spectroscopy detects alterations in oxygenation before pulse oximetry. J Intensive Care Med. 2008;23(6):384-388.
doi pubmed - Tobias JD. Cerebral oxygenation monitoring: near-infrared spectroscopy. Expert Rev Med Devices. 2006;3(2):235-243.
doi pubmed - Asakura A, Miyashita T, Fujimoto J, Morimura N, Kurahashi K, Yamada Y. A simple method to reduce the inspiratory oxygen fraction for high pulmonary blood flow patients in an operating room. Paediatr Anaesth. 2007;17(12):1194-1197.
doi pubmed - Berge JA, Gramstad L, Grimnes S. A simplified concept for controlling oxygen mixtures in the anaesthetic machine - better, cheaper and more user-friendly? Acta Anaesthesiol Scand. 1995;39(4):563-567.
doi pubmed - Hickey PR, Hansen DD, Strafford M, Thompson JE, Jonas RE, Mayer JE. Pulmonary and systemic hemodynamic effects of nitrous oxide in infants with normal and elevated pulmonary vascular resistance. Anesthesiology. 1986;65(4):374-378.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.