

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Case Report
Volume 9, Number 1, February 2018, pages 72-74
Conversion of Atrial Fibrillation to Sinus Rhythm During Coronary Intervention: Complex Interplay of Arrhythmic and Ischemic Substrate
Munish Sharmaa, e, Daniel A.N. Mascarenhasb, c, Bharat Kanthariad
aDepartment of Internal Medicine, Easton Hospital, Easton, PA, USA
bDrexel University College of Medicine, Philadelphia, PA, USA
cEaston Hospital, Easton, PA, USA
dCardiovascular and Heart Rhythm Consultants, NY, USA
eCorresponding Author: Munish Sharma, Department of Internal Medicine, Easton Hospital, PA 18042, USA
Manuscript submitted December 15, 2017, accepted December 27, 2017
Short title: Conversion of AF to Sinus Rhythm During PCI
doi: https://doi.org/10.14740/cr658w
| Abstract | ▴Top |
Atrial fibrillation (AF) can be a manifestation of acute coronary syndrome (ACS). Presence of AF during ACS further adds to complexities in the management issues and prognosis of ACS. We report a case of a 77-year-old male in whom we observed spontaneous conversion of AF to sinus rhythm during percutaneous coronary interventional procedure for critical ostial stenosis of the right coronary artery; and discuss potential electrophysiological mechanisms related to such phenomenon.
Keywords: Atrial fibrillation; Acute coronary syndrome; Right coronary artery
| Introduction | ▴Top |
Presence of atrial fibrillation (AF) during acute coronary syndrome (ACS) may have cause and effect relationship. Although the exact underlying mechanisms of AF in the setting of ACS, and vice versa, are not completely understood, their prognostic values as predictors of acute and long-term morbidities and mortalities, have been well-established [1]. Management of patients presenting with AF and ACS remains a complex issue such that as much as prompt coronary revascularization, prompt restoration of sinus rhythm is necessary. While the former is usually achieved by catheter-based percutaneous coronary intervention (PCI) procedure typically involving coronary stenting, for the latter most patients undergo pharmacological or direct current cardioversion. We report a case of a 77-year-old male who presented with AF and ACS, and while undergoing PCI for critical ostial stenosis of the right coronary artery (RCA) developed spontaneous conversion of AF to sinus rhythm.
| Case Report | ▴Top |
A 77-year-old male with a history of coronary artery disease, prior coronary artery bypass graftsurgery, bioprosthetic aortic valve replacement and paroxysmal AF presented with worsening shortness of breath on exertion for 1day. Patient did not have any chest pain, palpitation, dizziness, diaphoresis or nausea. Physical examination was significant for normal temperature, blood pressure of 110/70 mm Hg, irregular heart rate of 88 - 100 bpm, respiratory rate of 14/min with oxygen saturation of 95% at room air. Heart sounds were irregular with grade 1/6 ejection systolic murmur at right second intercostal space. Lungs were clear to auscultation. There was no evidence of edema of the extremities, and the rest of the physical examination was normal. His troponin I, serum potassium and magnesium were normal. He had an insertable loop recorder (ILR), (Reveal LINQ LNQ11Medtronic) which showed a new AF event for 36 h. The patient was brought to cardiac catheterization laboratory for coronary angiography with a view to PCI if necessary, and direct current cardioversion. Along with patent grafts and known disease in the respective coronary arteries, new critical and severe stenotic lesions involving the ostium and distal segment prior to the posterior descending branch of large dominant RCAwere detected (Fig. 1). These lesions were addressed in a stepwise manner with standard interventional balloon dilatation techniques. Interestingly, the patient’s rhythm converted to atrial flutter which converted to sinus rhythm upon PCI of the proximal ostial lesion restoring Thrombolysis in Myocardial Infarction (TIMI) grade 3 flows through the previously occluded segment as well as throughout the remainder of the vessel (Fig. 2, 3). He has remained free from any symptoms in sinus rhythm for more than 9 months as confirmed by regular follow-up of ILR.
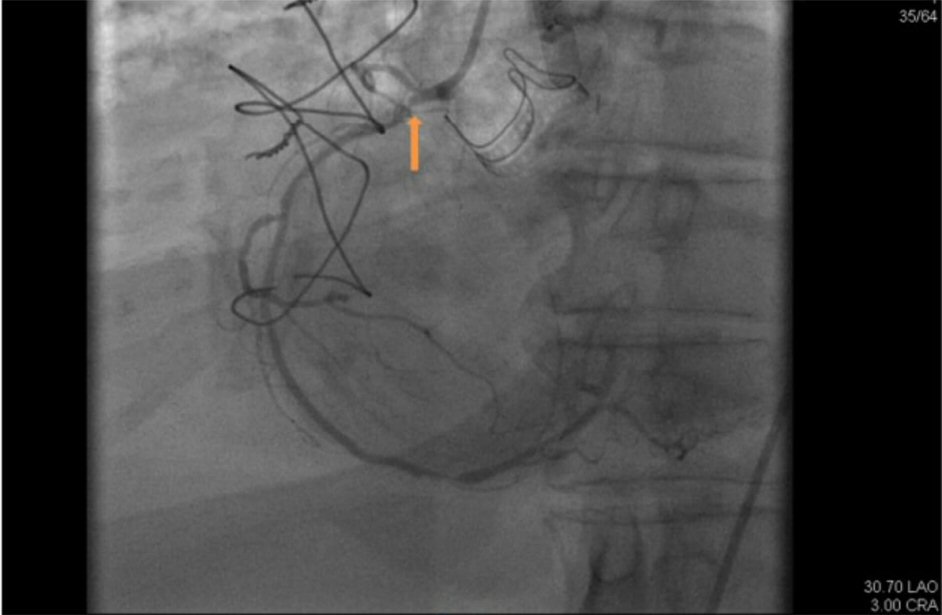 Click for large image | Figure 1. About 99% of proximal right coronary artery occlusion before balloon inflation. |
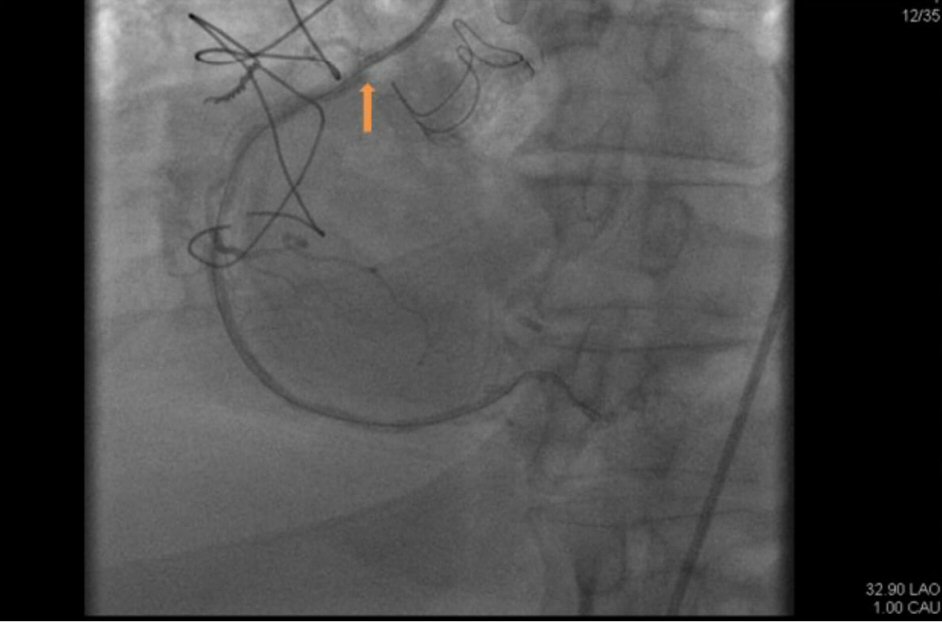 Click for large image | Figure 2. Proximal right coronary artery after balloon inflation. |
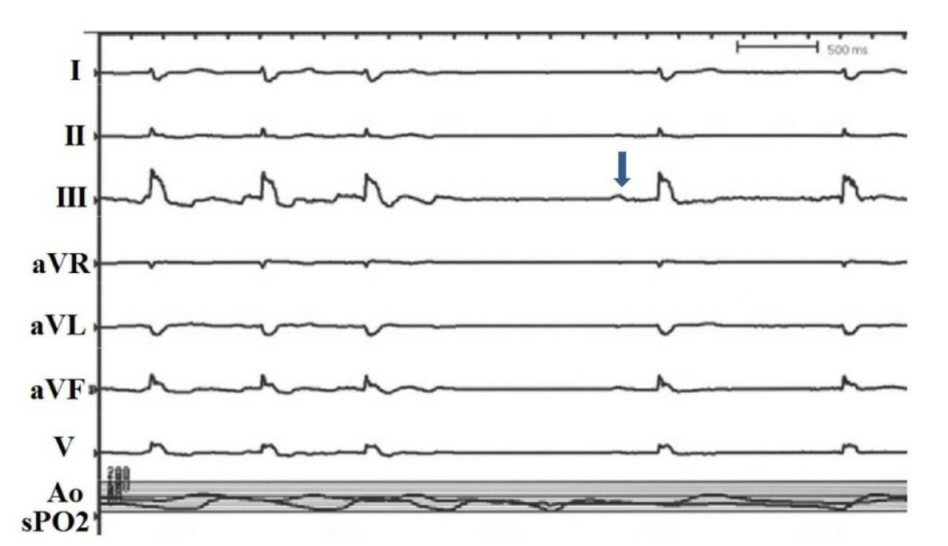 Click for large image | Figure 3. Conversion of atrial fibrillation to normal sinus rhythm during balloon inflation of the proximal right coronary artery (arrow). |
| Discussion | ▴Top |
An episode of ACS may trigger new onset AF or worsen existing AF, and conversely, AF itself may cause ACS by likely promoting a prothrombotic state but the exact mechanisms to explain the relationship are still speculative. In a study, patients more than 70 years of age were found to have 16% risk of developing AF post ACS while for those ≤ 59 years; the risk was 4.2% [2]. In REGARDS (Reasons for Geographic and Racial Differences in Stroke) cohort trial conducted in 24,000 United States citizens without underlying coronary artery disease, AF at baseline was found to be associated with increased risk of ACS (hazard ratio (HR) 1.70, 95% CI 1.26 - 2.30) [3]. The combination of these two entities poses complexity in the management of patients too, especially with regards to concomitant use of anticoagulants and antiplatelet drugs as it can increase the risk of severe bleeding. The risk for subsequent hospitalization for bleeding was found to be 1.8 times higher in patients on vitamin K antagonists (VKAs) and aspirin, 3.5 times higher in patients on clopidogrel and VKAs and 4 times higher in patients on triple therapy [4, 5]. Atrial ischemia induced by acute ST segment elevation myocardial infarction (MI) besides increased left atrial pressure due to left ventricular dysfunction, increased vagal stimulation and complication such as pericarditis have been postulated to be possible mechanism of infarct associated AF [6, 7]. There has been correlation found between stenosis of the RCA and the occurrence of AF, particularly in acute phase of infarction. In a study conducted on 1,039 patients to evaluate AF in MI, occlusion of the right proximal coronary artery was found to be associated with early onset MI (less than 24 h of onset of MI). Atrial and sinus node ischemia due to impairment of blood flow in the sinus node artery or atrioventricular node artery causing ischemia of atrium and sinus node, atrial ischemia and right atrial overload due to right ventricular MI were postulated to be pathophysiologic mechanisms for AF in occlusion of RCA [8].
In our case, we were able to directly demonstrate the restoration of normal sinus rhythm with relief of occlusion of a major dominant RCA. Although we did not have intra-cardiac recordings of electrical activation of different parts of the atria, nor was that intended to during our PCI procedure, we postulate that with restoration of coronary flow, the arrhythmia substrate changed such that the rhythm became more regular and stable as single wavelet atrial flutter (AFL) from multiwavelet AF. As is known, from the electrophysiological interrelationships between AF and AFL, during the period of AF, the functional component of AFL reentrant circuits is formed [9]. Restoration of coronary flow also influences autonomic balance between the sympathetic and parasympathetic inputs with further changes that occur in the automaticity and refractoriness of atrial tissue. Beat-to-beat cycle length oscillations also occur due to changes in areas of slow conduction in the reentrant circuit. When an earlier timed beat encounters area of full refractoriness from the preceding beat, and not be able to conduct through the critical isthmus, the arrhythmia terminates spontaneously.
The mortality due to acute MI and AF was found to be as high as 90 % when the reperfusion strategy was not available [10]. Two large studies found a higher incidence of in-hospital as well as long-term mortality in patients with AF and acute MI [2, 11]. In this context early angiography and revascularization may help achieve better prognosis and has been recommended in the conclusion of GUSTO-I Experience trial as well but further studies are warranted [12]. In our case, patient benefited from timely coronary angiography and reperfusion therapy as the patient spontaneously converted to sinus rhythm from AF and has remained so as evident by ILR monitoring. Hence patient did not require electrical or chemical cardioversion and achieved immediate symptomatic relief too.
Conflict of Interest
The authors declare no conflict of interest.
| References | ▴Top |
- Pizzetti F, Turazza FM, Franzosi MG, Barlera S, Ledda A, Maggioni AP, Santoro L, et al. Incidence and prognostic significance of atrial fibrillation in acute myocardial infarction: the GISSI-3 data. Heart. 2001;86(5):527-532.
doi pubmed - Behar S, Zahavi Z, Goldbourt U, Reicher-Reiss H. Long-term prognosis of patients with paroxysmal atrial fibrillation complicating acute myocardial infarction. SPRINT Study Group. Eur Heart J. 1992;13(1):45-50.
doi pubmed - Soliman EZ, Safford MM, Muntner P, Khodneva Y, Dawood FZ, Zakai NA, Thacker EL, et al. Atrial fibrillation and the risk of myocardial infarction. JAMA Intern Med. 2014;174(1):107-114.
doi pubmed - Capodanno D, Angiolillo DJ. Management of antiplatelet and anticoagulant therapy in patients with atrial fibrillation in the setting of acute coronary syndromes or percutaneous coronary interventions. Circ Cardiovasc Interv. 2014;7(1):113-124.
doi pubmed - Sorensen R, Hansen ML, Abildstrom SZ, Hvelplund A, Andersson C, Jorgensen C, Madsen JK, et al. Risk of bleeding in patients with acute myocardial infarction treated with different combinations of aspirin, clopidogrel, and vitamin K antagonists in Denmark: a retrospective analysis of nationwide registry data. Lancet. 2009;374(9706):1967-1974.
doi - Blanton RM, Nappi A, Kimmelstiel CD. Conversion of infarction-associated atrial fibrillation by restoration of atrial perfusion. Clin Cardiol. 2010;33(12):E79-81.
doi pubmed - Goldstein JA. Pathophysiology and management of right heart ischemia. J Am Coll Cardiol. 2002;40(5):841-853.
doi - Sakata K, Kurihara H, Iwamori K, Maki A, Yoshino H, Yanagisawa A, Ishikawa K. Clinical and prognostic significance of atrial fibrillation in acute myocardial infarction. Am J Cardiol. 1997;80(12):1522-1527.
doi - Waldo AL. Inter-relationships between atrial flutter and atrial fibrillation. Pacing Clin Electrophysiol. 2003;26(7 Pt 2):1583-1596.
doi pubmed - Hod H, Lew AS, Keltai M, Cercek B, Geft IL, Shah PK, Ganz W. Early atrial fibrillation during evolving myocardial infarction: a consequence of impaired left atrial perfusion. Circulation. 1987;75(1):146-150.
doi pubmed - Goldberg RJ, Seeley D, Becker RC, Brady P, Chen ZY, Osganian V, Gore JM, et al. Impact of atrial fibrillation on the in-hospital and long-term survival of patients with acute myocardial infarction: a community-wide perspective. Am Heart J. 1990;119(5):996-1001.
doi - Crenshaw BS, Ward SR, Granger CB, Stebbins AL, Topol EJ, Califf RM. Atrial fibrillation in the setting of acute myocardial infarction: the GUSTO-I experience. Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries. J Am Coll Cardiol. 1997;30(2):406-413.
doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.