

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Original Article
Volume 9, Number 5, October 2018, pages 273-278
Major Predictors of Incidence of Congestive Heart Failure and the Responsive Character of Enteral Nutrition: Meta-Analysis
Ana Valeria Garcia Ramireza, Eline de Almeida Sorianoa, Durval Ribas Filhoa, Idiberto Jose Zotarelli Filhob, c
aAssociacao Brasileira de Nutrologia (ABRAN)/Brazilian Association of Nutrology, Catanduva/SP, Rua Belo Horizonte, 909 - Centro, Catanduva SP 15801-150, Brazil
bPost Graduate and Continuing Education (Unipos), Department of Scientific Production, Street Ipiranga, 3460, Sao Jose do Rio Preto SP, Brazil
cCorresponding Author: Idiberto Jose Zotarelli Filho, Unipos - Post Graduate and Continuing Education, Street Ipiranga, 3460, Sao Jose do Rio Preto SP 15020-040, Brazil
Manuscript submitted June 18, 2018, accepted August 8, 2018
Short title: Heart Failure and Enteral Nutrition
doi: https://doi.org/10.14740/cr746w
| Abstract | ▴Top |
Background: Statistical data from the USA estimate that 5.7 million Americans over 20 years of age have congestive heart failure (CHF) and this number is expected to increase approximately 46.0% between 2012 and 2030. In Brazil, there are no epidemiological studies involving the incidence of heart failure; however, according to other countries, it can be estimated that up to 6.4 million Brazilians suffer from this syndrome. Randomized and controlled clinical studies on the efficacy of enteral nutrition (EN) in patients with CHF are lacking. The aim of the present study was to perform a systematic review of the main predictors of CHF that promote EN, as well as to find if the literary findings were conclusive in the efficacy of EN for treatment and prophylaxis of CHF.
Methods: A total of 105 papers were submitted to the eligibility analysis, after which 28 studies were selected, following the rules of the systematic review - PRISMA. The search strategy was followed in MEDLINE/Pubmed, Web of Science, ScienceDirect Journals (Elsevier), Scopus (Elsevier) and ONEFile (Gale), with the following steps: search for mesh terms and use of bouleanos “and” between terms and “or” between historical findings.
Results: The present study listed the major predictors of CHF with indication for EN. After testing the normality of each group of variables of causes of decompensation in CHF, it was analyzed that all the variables did not present normal distribution, with P < 0.10. Thus, a non-parametric Kruskal-Wallis analysis was performed, obtaining P > 0.05 in all analyses, that is, in all groups of causes of decompensation in CHF, there was no statistical difference in each group studied.
Conclusion: There is still no known influence of the efficacy of EN on increasing survival and reducing the morbidity of patients with CHF because there are few clinical trials that have evaluated this question; however, EN is very indicated in the attempt to mitigate the weight loss in these patients.
Keywords: Enteral therapy; Enteral nutrition; Cardiac insufficiency; Congestive heart failure; Clinical trials
| Introduction | ▴Top |
Congestive heart failure (CHF) is a serious and growing public health problem worldwide, being the final common pathway of most heart diseases [1, 2]. Although the scientific and technological advances and the better socioeconomic conditions have allowed the increase of the longevity of the general population and of the cardiac patients, there has been an increase in the incidence of CHF in the world [2-4]. Approximately 23 million people are carriers of this disease and two million new cases are diagnosed each year. CHF is an important public health issue due to its high prevalence, severity of clinical manifestations and reserved prognosis [3, 4].
Statistical data from the USA estimate that 5.7 million Americans over 20 years of age have CHF; an increase of approximately 46.0% is expected between 2012 and 2030, resulting in more than eight million adults [4]. In Brazil, there are no epidemiological studies involving the incidence of heart failure. However, according to other countries, up to 6.4 million Brazilians can be estimated to suffer from this syndrome [5].
CHF is caused by structural and functional abnormalities of the heart, leading to ventricular ejection defects and/or ventricular filling capacity [5-7]. In Brazil, the main causes of CHF are myocardial ischemia, systemic arterial hypertension, dilated cardiomyopathy and Chagas disease, as well as valvular disease [5]. After cardiac injury, the consequent molecular, structural and functional ventricular changes are known as cardiac remodeling. This process is accompanied by cardiac and systemic inflammatory and neuro-hormonal activation, which adversely affects the heart in a vicious cycle and compromises different organs and systems [5].
In recent decades, it has become clear that pathological changes involve not only the cardiovascular system, but also the renal, neuro-endocrinological, immunological, hematological, gastrointestinal and musculoskeletal systems, as well as nutritional status [1-3, 6, 7]. Currently, experimental and clinical studies have focused on the pathophysiology of systemic complications related to CHF in order to establish treatments to improve quality of life and increase survival [7, 8].
The clinical evolution of patients with CHF, as a rule, goes to varying degrees of malnutrition [5-8], necessitating the adhesion of enteral nutrition (EN). This may occur due to inadequate intake, altered metabolism, proinflammatory status, increased oxidative stress and increased nutrient loss, even through drug interactions. Anorexia is a consequence of reduced nutrient intake or the association of metabolic and absorptive changes (hypermetabolism, hypoxia, increased energy expenditure, inflammation) [8, 9].
Bowel edema in heart failure may be responsible for the presence of nausea, lipid malabsorption, gastric fullness sensation and protein losses [10].
The presence of malnutrition is an important predictor of survival reduction in patients with CHF regardless of important variables such as age, functional class and ejection fraction [2, 10, 11]. Thus, it becomes imperative to EN in an attempt to treat or mitigate the comorbidities of CHF.
The aim of the present study was to perform a systematic review of the main predictors of CHF that lead to EN, as well as to find if the literary findings were conclusive in the efficacy of enteral nutrition for treatment and prophylaxis of CHF.
| Patients and Methods | ▴Top |
Study design
A total of 105 papers that were submitted to the eligibility analysis were collected and, after that, 27 studies were selected, following the rules of the systematic review - PRISMA (Transparent Report of Systematic Reviews and Meta-Analyses - http://www.prisma -statement.org/), according to Fig. 1.
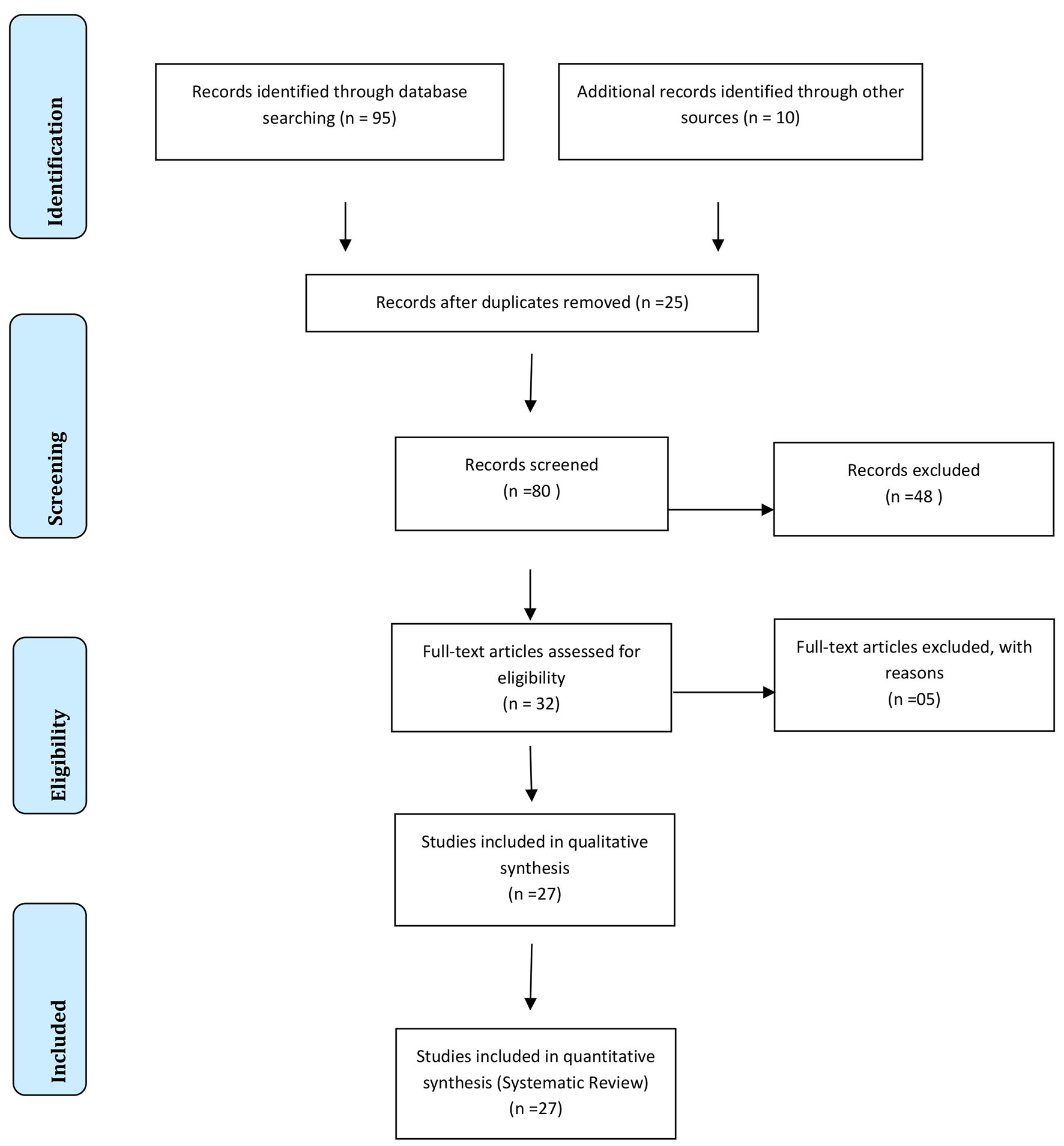 Click for large image | Figure 1. Flow chart. |
Information source
The review protocol was based on the literary search criteria with the use of Mesh Terms in the main databases such as Pubmed, Medline, Bireme, EBSCO, Scielo, etc. All references are registered in EndNote by the site:
http://www.myendnoteweb.com/EndNoteWeb.html?cat=myrefs&.
Search strategy
The search strategy was followed in MEDLINE/Pubmed, Web of Science, ScienceDirect Journals (Elsevier), Scopus (Elsevier) and ONEFile (Gale), with the following steps: search mesh terms (enteral therapy; enteral nutrition; heart failure; congestive heart failure; clinical trials), and use of bouleanos “and” between terms and “or” between historical findings.
Statistical treatment of literary findings
A descriptive analysis was performed with standard parameters of mean, standard deviation and amplitude. Anderson-Darling normality test (α-level > 0.10 considered as “normal”) was also performed for continuous and categorical data, with consequent application of Kruskal-Wallis analysis of variance to the internal data of each study alone, accepting P < 0.05 for statistical significance.
| Results | ▴Top |
The present study listed the major predictors of CHF with indication for enteral nutrition, according to Table 1. After testing the normality of each group of variables of causes of decompensation in CHF, it was analyzed that all the variables did not present normal distribution, with P < 0.10. Thus, a non-parametric Kruskal-Wallis analysis was performed, obtaining P > 0.05 in all analyses (α-level < 0.05 as a statistical difference reference), that is, in all groups of causes of decompensation in CHF, there was no statistical difference in each group studied. Therefore, the literary works evaluated in the present study presented the same response regarding the causes of decompensation in CHF.
 Click to view | Table 1. Major Predictors of CHF with Indication for Enteral Nutrition, with α-Level < 0.05 as a Statistical Difference Reference |
| Discussion | ▴Top |
Thus, CHF is a pathology in which circulatory, neuro-hormonal and metabolic factors interact causing cardiac muscle dysfunction, ventricular hypertrophy and hemodynamic changes [1-3]. The symptoms cause the individual great cardiac repercussions, with repeated hospitalizations and even death [3]. Mortality in CHF is related to age, with an increase of 27.0% per decade of life for men and 61.0% for women [4].
In CHF, there are multiple causal factors of malnutrition, called cardiac cachexia [1-5], as shown in Table 1. It is necessary to distinguish in CHF the eutrophic individual from those who present with insufficient nutrition or with severe malnutrition or cachexia, according to the classification of the New York Heart Association class III and IV [5].
Thus, the innumerable hospitalizations make the patients depressive and not receptive to feeding at restricted salt feeding and unattractive [5, 6]. Dyspnoea, muscular fatigue and edema, even in the gastrointestinal tract, makes a set for the reduction of oral intake, and EN is necessary [7-11].
Patients with CHF need to be evaluated by a multidisciplinary team to determine the patient’s state of depletion and thus, measures need to be taken to reduce the high catabolism caused by CHF, preserving the tissues and reducing the use of endogenous nutrients in order to recover organic functions to mitigate morbidity and mortality [12-15].
Severe malnutrition of the myocardiopathy is multifactorial [1-3, 16-18]. Metabolic imbalance occurs due to high basal energy expenditure, around 20.0%, and not always adequate caloric replacement [19]. Recent articles report the action of cytokines in the pathogenesis of cardiac cachexia [1-4].
Furthermore, tumor necrosis factor (TNF) has also been correlated with its elevation in class IV functional patients, especially those with cardiac cachexia, many believed to be caused by the accelerated effect of skeletal muscle catabolism [20]. Only patients with EN, associated or not with oral diet therapy can recover the catabolism generated by CHF [20, 21]. Other studies corroborate the early onset in stable myocardiopathic patients, around 24 - 48 h after cardiac decompensation [2, 3, 22].
EN is indicated for patients who do not meet the protein-calorie needs of oral diet [3, 23]. The use of the enteral route is well tolerated in patients, from 80.0% to 90.0% [1-3, 5, 24]. In patients malnourished by cardiac decompensation, by means of enteral infusion, one can achieve adequate nutritional intake, allied or not with oral diet [5, 25].
The elemental diet is indicated for patients with malabsorption, have pre-digested proteins and free amino acids [26]. The polymeric diet contains 30.0-40.0% of lipids, proteins and polysaccharides. If there is decreased gastric motility, the best choice is the elemental diet [26, 27].
Enteral diet may be infused continuously or intermittently. Studies have shown that patients who are more debilitated and less active accept diet better via a continuous probe, slowly and for a longer period, even in patients with heart disease [2, 6, 7]. According to the authors, continuous infusion should be decreased if the probability of gastric distension, diarrhea, pulmonary aspiration and metabolic abnormalities exits.
In case of diarrhea or intolerance, the fibers and ammonia in the diet formulation should be altered to protect the gastrointestinal tract [27]. In this sense, a higher rate of diarrhea was observed in the elderly when administered to the enteral diet intermittently [27]. Normally, diarrhea does not present a higher frequency in CHF patients, but constipation due to the lower amount of endogenous water and less physical movement [6, 7].
In addition, the pre-pyloric positioning is performed by nasogastric tube or gastrostomy, and the post-pyloric by nasojejunal or jejunostomy probe [8, 9]. In the literature, a higher probability of aspiration of the diet was not confirmed by intragastric or pyloric probe. However, the clinical body has a preference for post-pyloric placement [9].
The enteral infusion access is the percutaneous endoscopic gastrostomy, with low morbidity rates [3]. Due to the characteristics of the duodenal mucosa in the myocardiopathic patient, the diet should be chosen by evaluating its osmolarity, caloric density and infusion rate [3, 4].
Complications of EN
Despite the support provided by EN, there may be gastrointestinal, metabolic and mechanical complications [8]. In addition, infectious, respiratory and psychological complications may also occur [9-12]. Gastrointestinal complications are the most common, including nausea and vomiting of 2.5-10% [12]. Gastric stasis greatly impairs diabetic patients. Diarrhea is the most frequent, reaching up to 10.0-68.0% of cases [5].
In this context, according to the reports of complications observed by the Enteral and Parenteral Nutritional Support Group (GAENP) in Brazil, which analyzed 80 patients who used vasoactive drugs, 45.0% of them presented some digestive complications, in 21.0%, the complication was associated with probe discharge and, in 10.0%, diarrhea [5]. In another multicenter study conducted in the USA, it was verified in 360 patients that aspiration as a pulmonary complication was present in 88.0% of the cases [6].
Is there scientific evidence of EN in the treatment and prophylaxis of CHF?
Although few studies or case reports show the efficacy of EN to treat the comorbidities of patients with CHF, there is an urgent need for randomized and controlled trials of nutritional treatment in this condition, with the aim of improving cardiac function through a higher supply nutrients and energy.
The other goal of such treatment is also the complementation with other therapies to provide extra protein during treatment. In addition, other forms of nutritional support were tested in a small number of patients with cachexia, particularly those undergoing cardiac surgery, in whom preoperative feeding reduced the number of complications, mortality and duration of the postoperative hospital [5].
However, a major disadvantage of these favorable nutritional studies in CHF is the fact that they were all performed in the era before modern standard treatment with angiotensin-converting enzyme inhibitors and beta-blockers [2]. There is evidence that angiotensin-converting enzyme inhibitors prevent weight loss [5].
Conclusions
There is still no known influence of the efficacy of EN on increasing survival and reducing the morbidity of CHF patients because there are few clinical trials that have evaluated this question; however, EN is very indicated in the attempt to mitigate weight loss in these patients.
Conflict of Interest
None.
| References | ▴Top |
- Marcadenti A, Mendes LL, Rabito EI, Fink JDS, Silva FM. Nutritional risk in emergency-2017: a new simplified proposal for a nutrition screening tool. JPEN J Parenter Enteral Nutr. 2018.
doi pubmed - Lash K, Oppel R, Hasse J. Successful placement of nasointestinal feeding tubes using an electromagnetic sensor-guided enteral access system in patients with left ventricular assist devices. Nutr Clin Pract. 2018;33(2):281-285.
doi pubmed - Lewis KD, Conway J, Cunningham C, Larsen BMK. Optimizing nutrition in pediatric heart failure: the crisis is over and now it's time to feed. Nutr Clin Pract. 2018;33(3):397-403.
pubmed - Sahu MK, Singal A, Menon R, Singh SP, Mohan A, Manral M, Singh D, et al. Early enteral nutrition therapy in congenital cardiac repair postoperatively: A randomized, controlled pilot study. Ann Card Anaesth. 2016;19(4):653-661.
doi pubmed - Okoshi MP, Capalbo RV, Romeiro FG, Okoshi K. Cardiac Cachexia: Perspectives for Prevention and Treatment. Arq Bras Cardiol. 2017;108(1):74-80.
pubmed - Pinho RA, Araujo MC, Ghisi GL, Benetti M. [Coronary heart disease, physical exercise and oxidative stress]. Arq Bras Cardiol. 2010;94(4):549-555.
doi pubmed - Anker SD, John M, Pedersen PU, Raguso C, Cicoira M, Dardai E, Laviano A, et al. ESPEN Guidelines on enteral nutrition: cardiology and pulmonology. Clin Nutr. 2006;25(2):311-318.
doi pubmed - Singer P, Berger MM, Van den Berghe G, Biolo G, Calder P, Forbes A, Griffiths R, et al. ESPEN Guidelines on parenteral nutrition: intensive care. Clin Nutr. 2009;28(4):387-400.
doi pubmed - Kreymann KG, Berger MM, Deutz NE, Hiesmayr M, Jolliet P, Kazandjiev G, Nitenberg G, et al. ESPEN guidelines on enteral nutrition: intensive care. Clin Nutr. 2006;25(2):210-223.
doi pubmed - McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, McCarthy MS, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. 2016;40(2):159-211.
doi pubmed - Singer P, Hiesmayr M, Biolo G, Felbinger TW, Berger MM, Goeters C, Kondrup J, et al. Pragmatic approach to nutrition in the ICU: expert opinion regarding which calorie protein target. Clin Nutr. 2014;33(2):246-251.
doi pubmed - Dvir D, Cohen J, Singer P. Computerized energy balance and complications in critically ill patients: an observational study. Clin Nutr. 2006;25(1):37-44.
doi pubmed - Alberda C, Gramlich L, Jones N, Jeejeebhoy K, Day AG, Dhaliwal R, Heyland DK. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med. 2009;35(10):1728-1737.
doi pubmed - Faisy C, Candela Llerena M, Savalle M, Mainardi JL, Fagon JY. Early ICU energy deficit is a risk factor for Staphylococcus aureus ventilator-associated pneumonia. Chest. 2011;140(5):1254-1260.
doi pubmed - Petros S, Horbach M, Seidel F, Weidhase L. Hypocaloric vs normocaloric nutrition in critically ill patients: a prospective randomized pilot trial. JPEN J Parenter Enteral Nutr. 2016;40(2):242-249.
doi pubmed - Villet S, Chiolero RL, Bollmann MD, Revelly JP, Cayeux RNM, Delarue J, Berger MM. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin Nutr. 2005;24(4):502-509.
doi pubmed - Heyland DK, Dhaliwal R, Wang M, Day AG. The prevalence of iatrogenic underfeeding in the nutritionally 'at-risk' critically ill patient: Results of an international, multicenter, prospective study. Clin Nutr. 2015;34(4):659-666.
doi pubmed - Petros S, Engelmann L. Enteral nutrition delivery and energy expenditure in medical intensive care patients. Clin Nutr. 2006;25(1):51-59.
doi pubmed - Genton L, Dupertuis YM, Romand JA, Simonet ML, Jolliet P, Huber O, Kudsk KA, et al. Higher calorie prescription improves nutrient delivery during the first 5 days of enteral nutrition. Clin Nutr. 2004;23(3):307-315.
doi pubmed - Oshima T, Heidegger CP, Pichard C. Supplemental parenteral nutrition is the key to prevent energy deficits in critically ill patients. Nutr Clin Pract. 2016;31(4):432-437.
doi pubmed - Oshima T, Deutz NE, Doig G, Wischmeyer PE, Pichard C. Protein-energy nutrition in the ICU is the power couple: A hypothesis forming analysis. Clin Nutr. 2016;35(4):968-974.
doi pubmed - Pichard C, Oshima T, Berger MM. Energy deficit is clinically relevant for critically ill patients: yes. Intensive Care Med. 2015;41(2):335-338.
doi pubmed - Heidegger CP, Berger MM, Graf S, Zingg W, Darmon P, Costanza MC, Thibault R, et al. Optimisation of energy provision with supplemental parenteral nutrition in critically ill patients: a randomised controlled clinical trial. Lancet. 2013;381(9864):385-393.
doi - Gramlich L, Kichian K, Pinilla J, Rodych NJ, Dhaliwal R, Heyland DK. Does enteral nutrition compared to parenteral nutrition result in better outcomes in critically ill adult patients? A systematic review of the literature. Nutrition. 2004;20(10):843-848.
doi pubmed - Evans RA, Strauss BJ. Cost and benefit of hospital, hospital- in- the- home and ambulatory care nutrition support services. Asia Pac J Clin Nutr. 1998;7(3/4):241-244.
pubmed - Wei X, Day AG, Ouellette-Kuntz H, Heyland DK. The association between nutritional adequacy and long-term outcomes in critically ill patients requiring prolonged mechanical ventilation: a multicenter cohort study. Crit Care Med. 2015;43(8):1569-1579.
doi pubmed - Reignier J, Darmon M, Sonneville R, Borel AL, Garrouste-Orgeas M, Ruckly S, Souweine B, et al. Impact of early nutrition and feeding route on outcomes of mechanically ventilated patients with shock: a post hoc marginal structural model study. Intensive Care Med. 2015;41(5):875-886.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.