

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Case Report
Volume 10, Number 3, June 2019, pages 193-198
Transcatheter Double Valve-in-Valve Replacement of Aortic and Mitral Bioprosthetic Valves
Javad Savoja, Syed Iftikhara, d, Steven Bursteinb, Patrick Hua, c, d
aDepartment of Internal Medicine, UC Riverside School of Medicine/Riverside Community Hospital, Riverside, CA 92501, USA
bDepartment of Cardiology, Good Samaritan Hospital/Harbor-UCLA, Los Angeles, CA 90017, USA
cDepartment of Cardiology, Riverside Medical Clinic, Riverside, CA 92501, USA
dCorresponding Author: Patrick Hu, Department of Internal Medicine, UC Riverside School of Medicine/Riverside Community Hospital, Riverside, CA 92501, USA
Manuscript submitted April 8, 2019, accepted April 23, 2019
Short title: TDVIVR of Valve Stenosis
doi: https://doi.org/10.14740/cr863
| Abstract | ▴Top |
Transcatheter aortic valve replacement (TAVR) is an evolving method which has become the treatment of choice in high-risk patients with severe aortic stenosis. Unlike TAVR, the experience with transcatheter mitral valve replacement (TMVR) remains at an early stage because of challenges of valve development and possible complications such as valve displacement and subsequent left ventricular outlet tract (LVOT) obstruction. Here we report a case of transcatheter double valve-in-valve replacement (TDVIVR) in a patient with severe mitral and aortic bioprosthetic valve stenosis, followed by an extensive literature review of the latest techniques and challenges in this field.
Keywords: Transcatheter aortic valve replacement; Transcatheter mitral valve replacement; Transcatheter double valve-in-valve replacement; Left ventricular outlet tract
| Introduction | ▴Top |
The prevalence of severe aortic stenosis (AS) increases with age to 3.4% in patients aged 75 years or older. Previously, surgical aortic valve replacement (SAVR) was the only recommended treatment of choice, but transcatheter aortic valve replacement (TAVR) has emerged as an alternative treatment option over the last 15 years [1] and FDA approved in the United States since 2011. Meanwhile, surgical mitral valve repair or replacement remains the gold standard for treating severe symptomatic mitral valve disease. Unlike TAVR, the experience with transcatheter mitral valve implantation (TMVI) remains at an early stage due to challenges of valve development and possible complications such as valve displacement and subsequent left ventricular outlet tract (LVOT) obstruction. However, up to 35% of patients require a repeat operation during the first 10 years, and the in-hospital mortality rate may be as high as 12%. Recently, percutaneous mitral valve interventions have emerged as alternatives to conventional surgical valve replacement in patients requiring repeat surgery. Hu et al reported the first transcatheter mitral valve-in-valve (TMVIV) implantation in humans in 2009 [2]. Transcatheter valve-in-valve implantation (VIV) has shown good results in high-risk patients suffering from structural valve deterioration (SVD) of a previously implanted heart valve bioprosthesis. The advantages of VIV over conventional redo surgery are mainly related to a less invasive approach, which includes shorter duration of the procedure and no need for mediastinal reentry, cardiopulmonary bypass, aortic cross clamping and removal of the failed valve. VIV has been described in aortic, mitral, tricuspid and pulmonary position, but it is usually performed on a single valve [3]. Here we report a case of transcatheter double VIV replacement (TDVIVR) in a patient with severe mitral and aortic bioprosthetic valve stenosis, discuss the outcome and review different techniques used.
| Case Report | ▴Top |
Patient was a 76-year-old woman with history of rheumatic mitral and AS status post surgical mitral and aortic valve replacement 11 years before presentation to the hospital, atrial fibrillation and status post atrial appendage ligation who had been developing severe heart failure symptoms before presentation to the hospital. Patient had history of recent cholecystitis which had been managed by cholecystostomy due to high risk of surgical intervention. Having functional NYHA class 4 heart failure, patient was candidate for both aortic and mitral valve replacement. However, being in cardiogenic shock and having high risk of sepsis from recently placed cholecystostomy catheter following cholecystitis, it was decided that the patient was not a good candidate for surgical valve replacement and was sent for TDVIVR.
Procedure details
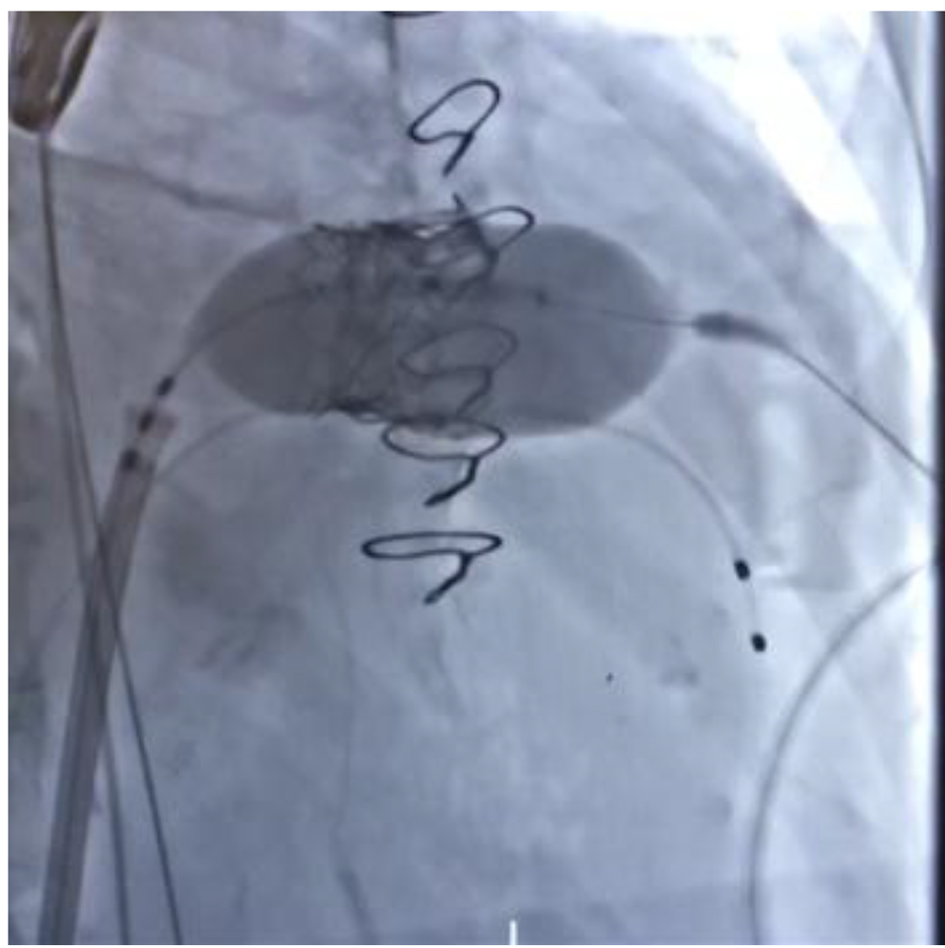
Access was obtained in the left femoral artery and vein, and right femoral artery. Temporary pacemaker was placed in the RV apex via the left femoral vein. TAVR 23-mm Edwards Sapien S3 was to be placed via right femoral artery. TMVR was to be done using the 29-mm Edwards Sapien S3 (TAVR valve) in the mitral position. Right common femoral venous access and LV puncture was completed. Initial fluoroscopic image with old bioprosthetic mitral and aortic valves was obtained (Fig. 1). Following left ventricle puncture, an exchange-length Glidewire was passed through the sheath into the LV and into the left atrium. In the next step, an 8.5 SL1 sheath was passed over the J-tip core wire into the right atrium. The BRK XS trans-septal needle was passed to the SL1 sheath. Trans-septal puncture was performed with subsequent placement of the SL1 sheath in the left atrium.
 Click for large image | Figure 1. Cardiac fluroscopy before procedures showing previous bioprosthetic mitral and aortic valves. |
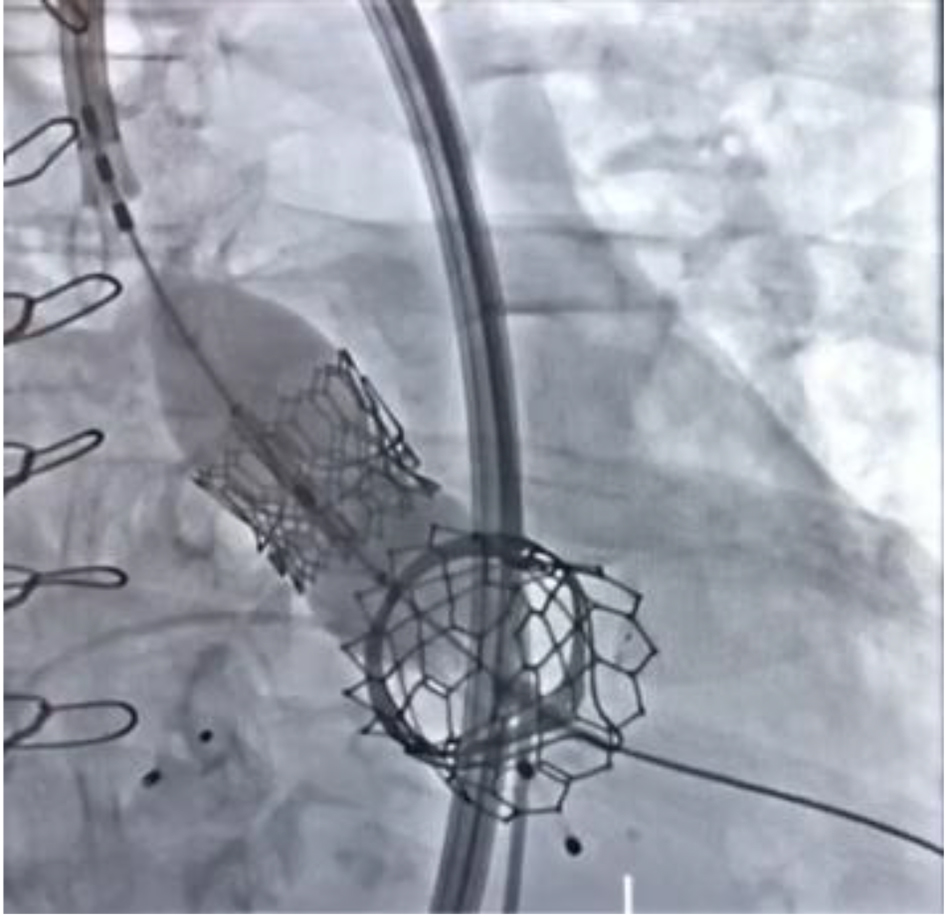
In the next step, a 6-French MP-1 guide catheter was passed over J-wire into the left atrium. Once the guide catheter was in the left atrium, a GooseNeck 20-mm snare was passed and manipulated to snare the Glidewire. Then, a 16-French Edwards TAVR sheath was passed over the Glidewire into the inferior vena cava (IVC). The sheath was advanced over the interatrial septum after an atrial septostomy was performed using a 7-mm Mustang balloon. The 29-mm Edwards Sapien S3 valve was passed through the sheath across the mitral valve bioprosthesis. After multiple coplanar views obtained of the mitral valve, ventilation was held and rapid pacing was initiated and the valve was deployed (Fig. 2). Echocardiographic finding did not demonstrate any perivalvular leak.
 Click for large image | Figure 2. Balloon inflation and transcatheter bioprosthetic mitral valve deployment. |
The delivery sheath was then removed from the right groin. Interatrial septum was closed by an 8-mm Amplatzer septal occluder.
TAVR
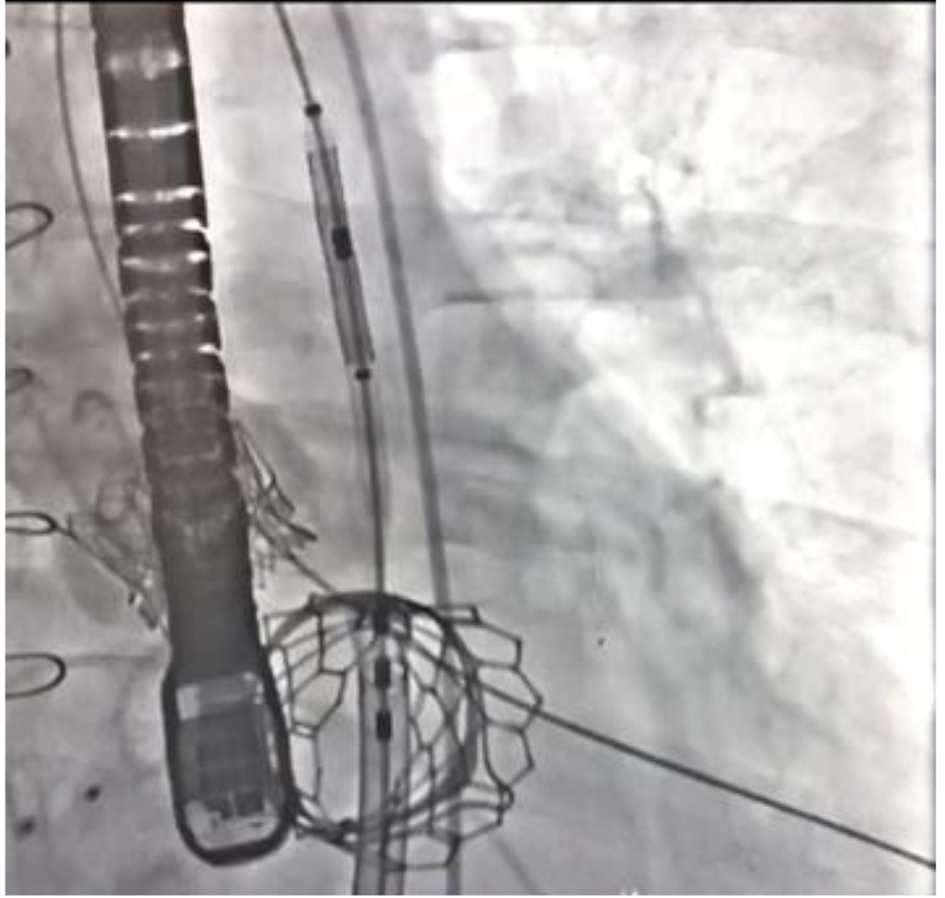
Multiple attempts to cross the aortic valve with the straight-tip wire were unsuccessful via the femoral artery approach. Therefore, a 0.035-inch exchange-length J-tip wire was passed through the 4-French apical sheath into the LV and ascending aorta through the bioprosthetic aortic valve. The 9-French sheath from the right common femoral artery was exchanged over for a 14-French Edwards delivery system. A 6-French FR4 guide catheter was passed through this 14-French sheath into the ascending aorta. Subsequently, the Amplatzer GooseNeck snare was reintroduced through the FR4 guide catheter into the aortic arch, near the brachiocephalic artery. Once the snare was loosened up with aortic arch, the J wire was passed through this snare and was snared from the right common femoral artery. The 23-mm Edwards Sapien 3 valve was passed, advanced and positioned across the aortic valve prosthesis when coplanar view was obtained, ventilation held, and rapid pacing was instituted. The pigtail was pulled back and the 23-mm Edwards Sapien S3 valve was deployed (Fig. 3). Post-operative fluoroscopic image with both TAVR and TMVR valves in place was taken (Fig. 4).
 Click for large image | Figure 3. Balloon inflation and transcatheter aortic valve deployment with bioprosthetic mitral valve in place. |
 Click for large image | Figure 4. Post-operative image with TAVR and TMVR valves in place. TAVR: transcatheter aortic valve replacement; TMVR: transcatheter mitral valve replacement. |
Patient follow-up
Two months after the procedure, patient’s NYHA class improved to class 2. Patient was feeling better and her cholecystostomy catheter was removed. Echocardiogram showed aortic valve mean gradient of 18 mm Hg and maximum gradient of 31 mm Hg.
After 7 months of follow-up, patient’s functional class remained the same. However, new echocardiogram showed two left atrial clots and patient was started on apixaban.
After 14 months of follow-up, patient remained clinically stable. Transesophageal echocardiogram showed remaining left atrial clot in residual appendage as well as the same aortic valve gradient (Fig. 5). Patient’s anticoagulant medication was switched from apixaban to rivaroxaban to provide a higher dose of anticoagulation.
 Click for large image | Figure 5. Follow-up transesophageal echocardiogram with left atrial thrombus. |
| Discussion | ▴Top |
The majority of surgical heart valves (SHVs) implanted are bioprosthetic valves. These valves are prone to over the time structural deterioration, which may manifest as valvular stenosis, regurgitation or a combination of both. It is well established that bioprosthetic valves have a shortened lifespan in younger patients, arguably due to a more robust immune response, and heightened hemodynamic stress. Both the shortened durability of valves and longer life expectancy in younger patients may contribute to a higher incidence of subsequent repeat valve replacement in the future. Although re-operation is the current standard of care, this carries a significant risk of mortality and morbidity [4]. Therefore, new procedures such as TAVR, TMVR and TDVR could potentially be considered as viable alternatives in high-risk patients.
Surgical valve replacements such as mitral valves have a higher rate of degeneration than aortic valves. This is likely because the mitral valve is exposed to a systolic pressure gradient while the aortic valve is exposed to a diastolic pressure gradient. Additionally, valve-in-valve procedures create a tube graft by the second valve continuously holding open the first valve. In the aortic position, coronary circulation is at risk, and the likelihood of an occlusion can be predicted reliably from computed tomography (CT) scans based on the size of the sinuses of Valsalva. In the mitral position, the “tube graft” will interfere with the left ventricular outflow track (LVOT) and the extent of this obstruction is much more difficult to predict. Additionally, the consequences of complications, for example, the need for a permanent pacemaker and suboptimal hemodynamic results, such as residual gradients or paravalvular leaks, are more impactful, especially due to the longer life expectancy of younger patients [5].
Potential LVOT obstruction is a known periprocedural complication of TMVR. LVOT obstruction can cause diminished LV ejection fraction, and can contribute to cerebral hypoperfusion, syncope and arrhythmias. Due to the anatomy of the mitral valve, and its proximity to both atrial and ventricular structures, LVOT obstruction provides a significant challenge. LVOT obstruction can be defined as a sudden decline in hemodynamics following TMVR, visible LVOT obstruction on echocardiography and an increase in LVOT gradient by 10 mm Hg [6]. One study discovered LVOT obstruction in 13.4% of TMVR [7]. Furthermore, LVOT obstruction may potentially pose an even more significant challenge in TDVIVR due to the manipulation of both aortic and mitral valves. Various parameters of the mitral annulus including annular area, native LVOT diameter and area, mitral annulus to interventricular septum distance and angle, have been studied; however, optimal values of each of these are not yet established. Due to this common challenge, pre-operative cardiac CT should be obtained as well as pre-operative and intra-operative echocardiography to evaluate some of these hemodynamic measures. Estimating the effect that simultaneous dual transcatheter valve replacement will have upon hemodynamic parameters becomes even more challenging because exact changes can be hard to predict. Furthermore, downstream effects of implantation prior to implanting the second valve are difficult to estimate. This phenomenon is one that the operator should be cognizant of, and evaluate closely given the high morbidity and mortality involved.
When considering optimal success of TDVIVR, there are certain factors that will contribute to procedural success. Here we review the different factors contributing in choosing the best candidates and procedure techniques.
Valve selection
Selection of the best transcatheter heart valve (THV) for a patient depends on the type and the size of SHV in place.
SHVs can be broadly classified as stented or stentless, based on the presence or absence of a rigid pericardium or fabric covered stent frame. Stented valves consist of a rigid frame and three struts or posts within which three bovine pericardial or porcine leaflets are suspended. It is essential to confirm the nature of the original surgical implantation as different implantation techniques may be subject to different challenges when considering a VIV procedure. Furthermore, the “true” inner diameter (T-ID) of the surgical bioprosthesis is one of the most important pieces of information needed for selecting the size of the THV for the aortic or mitral VIV procedure. CT scan of the surgical valves as well as echocardiogram play significant roles in the determination of THV size [8].
The two most commonly used THVs for the VIV procedure are the Edwards Sapien valve (ESV), (Edwards Lifesciences, Irvine, CA, USA), which has been used in all four valve positions, and the Medtronic CoreValve (MCV) (Medtronic Inc., Minneapolis, MN, USA) used in the aortic position alone. Other more recent additions to the market but used in the aortic position alone are the St. Jude portico valve (SPV) (St. Jude Medical, St. Paul, MN, USA), the JenaValve (JV) (JenaValve, Munich, Germany) and the Symetis valve (SV) (Symetis, Vaud, Switzerland). The Melody valve (Medtronic Inc., Minneapolis, MN, USA) has been used in both the pulmonary and mitral positions [4].
Valve positioning
The neo-annulus of the SHV is used as reference line during positioning. It is identified by correlating the structure of the SHV to its fluoroscopic appearance. This neo-annulus is at the level of the sewing ring of the surgical valve. In some SHVs, there is a marker within the sewing ring which facilitates identification of this level. Some valves have their stent frame visible and for these it is important to assess the relationship between the inflow and the level of the sewing ring. In SHVs, with no fluoroscopic marker in the frame or sewing ring, this level can be determined during the procedure by the use of pig-tail catheter with multiple contrast injections, balloon valvuloplasty or transesophageal echocardiography (TEE) [9]. It is essential to ensure that the implant position of a THV within a given SHV is in its ideal position as too low a position can lead to suboptimal function or paravalvular regurgitation and too high a position may lead to coronary obstruction (aortic valve) or embolization [10].
Access options
Antegrade trans-septal access
The first reported human transcatheter aortic valve implantation has been performed by Alain Cribier in 2002 via an antegrade trans-septal access. Because of the complexity of this approach, it was abandoned after the introduction of the transfemoral and transapical routes. Today, the trans-septal route has a significant value to access the mitral valve.
Retrograde transfemoral access
This access is considered first choice in many TAVR centers because of its obvious minimal invasiveness. With several 10 thousands transfemoral TAVRs having been performed worldwide, a broad experience has been gained during the last years. Still, vascular complications at the femoral access site are reported in 10-20% in large patient series being described to be associated with increased mortality.
Antegrade transapical access
The transapical technique is well standardized today and used at most centers as the second option for TAVR patients if a transfemoral implantation is not feasible. The first human transapical aortic valve implantation has been performed by the group of John Webb with the antecessor valve of the Sapien prosthesis in 2005. Advantages of the transapical procedure are a short distance from the sheath to the annulus and the antegrade implantation route facilitating exact positioning, the possibility to accommodate larger sheaths up to 36 F, and virtually no access limitation as the apex can be exposed in almost every patient. Thoracic deformations precluding a lateral incision, which are very rare, and a very poor left ventricular ejection fraction may be seen as contraindications for transapical TAVR.
Retrograde subclavian access
The first case reports on this new approach were published in 2008. The right subclavian artery is rarely used, due to an unfavorable implantation angle. The vast majority of subclavian TAVI cases are performed using the CoreValve prosthesis, because of a small introducer sheath. Only few cases of Sapien implantations through the subclavian artery have been described. Usually, a surgical cut-down is performed to access the subclavian artery and to introduce the sheath after placement of purse-string sutures. More recently, a percutaneous access technique has been described. This access should be considered when the femoral approach is impossible or difficult, albeit feasible.
Retrograde transaortic access
The direct transaortic route for TAVI was first reported in 2009 as a bail-out strategy in a patient with unfeasible transfemoral, subclavian or transapical access. To access the ascending aorta, a full or partial upper sternotomy, or a right anterolateral thoracotomy can be performed through skin incisions of 6 - 7 cm. As a porcelain aorta is considered a contraindication for the transaortic approach, careful CT assessment of the calcium distribution in the ascending aorta is required. This access is usually used when previous options are unfavorable.
Transatrial, transjugular and femoral vein access
These accesses have been recently used in valve-in-valve or valve-in-ring implantation in degenerated biological surgical prostheses or failed repair procedures of the mitral and tricuspid valve. Therefore, some other access sites than for the aortic valve are required. Access to a mitral ring or bioprosthesis can, however, be achieved with the well-established transapical technique. There are a couple of case reports describing alternative procedures, such as venous femoral trans-septal mitral valve-in-valve implantation, or venous transjugular trans-septal mitral valve-in-valve implantation. The transjugular access has also been used to access the tricuspid valve. Another alternative is the access through a right lateral thoracotomy and direct atrial access, where both atria can be approached.
Transcarotid access is another approach which is recently introduced for TAVR. There is little experience with this type of access [11].
Sequence of deployment in TDVIVR
D’Onofrio et al in a case report of TDVIVR in 2014 suggested that aortic valve deployment should be done first in this procedure [3]. This reasoning was based on three factors: 1) Immediate afterload reduction and consequently better hemodynamic conditions for the mitral procedure; 2) Less chance of acute hemodynamic deterioration in case of mitral prosthesis failure causing severe regurgitation; 3) Less chance of deployed mitral valve displacement and/or aortic valve malposition.
In our case, we showed that if the patient is in cardiogenic shock due to double valve stenosis, placement of mitral valve in the first place provides a better cardiac output and more hemodynamic stability for aortic valve placement.
Although high aortic valve gradient is one of the common complications of TMVR, it is not related to sequence of valve placement, especially if all the measurements and precautions are properly done.
Conclusion
In conclusion, we believe that TDVIVR may have a better long-term outcome in patients with history of primary prosthetic valve placement and can be considered in high-risk patients who are not candidates for surgical valve replacement. Furthermore, successful placement of mitral valve before aortic valve in our patient is promising for patients who receive TMVR in early ages and need subsequent TAVR at a later time.
Acknowledgments
None.
Financial Disclosure
None to report.
Conflict of Interest
None to declare.
Informed Consent
Informed consent was obtained.
Author Contributions
JS: drafting article, writing manuscript; SI: writing manuscript, obtaining consent; SB: obtaining appropriate images and interpretation of images; PH: correspondence, general supervision, manuscript editing and manuscript review.
| References | ▴Top |
- Wagner G, Steiner S, Gartlehner G, Arfsten H, Wildner B, Mayr H, Moertl D. Comparison of transcatheter aortic valve implantation with other approaches to treat aortic valve stenosis: a systematic review and meta-analysis. Syst Rev. 2019;8(1):44.
doi pubmed - Hu J, Chen Y, Cheng S, Zhang S, Wu K, Wang W, Zhou Y. Transcatheter mitral valve implantation for degenerated mitral bioprostheses or failed surgical annuloplasty rings: A systematic review and meta-analysis. J Card Surg. 2018;33(9):508-519.
doi pubmed - D'Onofrio A, Zucchetta F, Gerosa G. Simultaneous transapical aortic and mitral valve-in-valve implantation for double prostheses dysfunction: case report and technical insights. Catheter Cardiovasc Interv. 2014;84(3):509-512.
doi pubmed - Noorani A, Radia R, Bapat V. Challenges in valve-in-valve therapy. J Thorac Dis. 2015;7(9):1501-1508.
- Wyler von Ballmoos MC, Kalra A, Reardon MJ. Complexities of transcatheter mitral valve replacement (TMVR) and why it is not transcatheter aortic valve replacement (TAVR). Ann Cardiothorac Surg. 2018;7(6):724-730.
doi pubmed - Yoon SH, Bleiziffer S, Latib A, Eschenbach L, Ancona M, Vincent F, Kim WK, et al. Predictors of left ventricular outflow tract obstruction after transcatheter mitral valve replacement. JACC Cardiovasc Interv. 2019;12(2):182-193.
doi pubmed - Stone GW, Adams DH, Abraham WT, Kappetein AP, Genereux P, Vranckx P, Mehran R, et al. Clinical trial design principles and endpoint definitions for transcatheter mitral valve repair and replacement: part 2: endpoint definitions: a consensus document from the mitral valve academic research consortium. J Am Coll Cardiol. 2015;66(3):308-321.
doi pubmed - Shivaraju A, Michel J, Frangieh AH, Ott I, Thilo C, Schunkert H, Kastrati A, et al. Transcatheter aortic and mitral valve-in-valve implantation using the edwards sapien 3 heart valve. J Am Heart Assoc. 2018;7(14).
doi - Bapat V. Technical pitfalls and tips for the valve-in-valve procedure. Ann Cardiothorac Surg. 2017;6(5):541-552.
doi pubmed - Bapat VN, Attia RQ, Condemi F, Visagan R, Guthrie M, Sunni S, Thomas M. Fluoroscopic guide to an ideal implant position for Sapien XT and CoreValve during a valve-in-valve procedure. JACC Cardiovasc Interv. 2013;6(11):1186-1194.
doi pubmed - Bleiziffer S, Krane M, Deutsch MA, Elhmidi Y, Piazza N, Voss B, Lange R. Which way in? The necessity of multiple approaches to transcatheter valve therapy. Curr Cardiol Rev. 2013;9(4):268-273.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.