

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Review
Volume 13, Number 1, February 2022, pages 2-10

Quadricuspid Aortic Valve: An Introduction for Clinicians
Shivan Saitha ![]() , Sunil Saithb
, Sunil Saithb ![]() , Avinash Murthyc, d
, Avinash Murthyc, d
aRutgers Graduate School of Biomedical Sciences, Portage, MI 49024, USA
bDepartment of Cardiology, SUNY Downstate Health Sciences University, Brooklyn, NY 11203, USA
cPrairie Cardiovascular, Springfield, IL 62769, USA
dCorresponding Author: Avinash Murthy, Prairie Cardiovascular, Springfield, IL 62769, USA
Manuscript submitted July 11, 2021, accepted July 24, 2021, published online January 29, 2022
Short title: Quadricuspid Aortic Valve
doi: https://doi.org/10.14740/cr1308
- Abstract
- Incidences
- Classifications
- Causes
- Mode of Presentation
- Diagnosis
- Management
- Follow-Up
- Conclusions
- References
| Abstract | ▴Top |
Quadricuspid aortic valve (QAV) is a congenital heart anomaly in which the aortic valve has four cusps of various size possibilities, as opposed to the three symmetrical cusps generally observed. This cardiac valvular abnormality is rarely identified, with an estimated incidence rate of 0.013% to 0.043%, although recent technological advancements in diagnostics have contributed to an increase in detection. Historically, it had been typically encountered during open heart surgery or postmortem; however, it is presently diagnosed primarily via ultrasound echocardiography, and could go undetected unless specifically considered. It was first reported by Babington in 1847, and since then approximately 300 cases have been published. This condition is sporadically associated with additional congenital cardiovascular defects, with coronary artery irregularities being the most common. In more than half of published QAV incidences it has led to the progressive development of aortic regurgitation (AR) usually sans aortic stenosis, particularly amongst elderly patients, often requiring surgical intervention after 50 years of age. A fifth of total instances, but two-thirds of instances with AR, warrant surgery seldom amidst complications, with reconstructive tricuspidization preferred over valve replacement.
Keywords: Quadricuspid aortic valve; Aortic valve insufficiency; Congenital valve disorders; Heart valve diseases; Cardiac surgical procedures; Aortic valve reconstruction surgery
| Incidences | ▴Top |
Perhaps the first retained human awareness of the valvulopathy preceded even medical journals, as Leonardo da Vinci’s detailed anatomical illustrations and notes on the typical tricuspid aortic valve dated to 1512 - 13 also includes quadricuspid and bicuspid examples [1]. Dr. Benjamin Guy Babington reported the first known case of quadricuspid aortic valve (QAV) in an 1847 London Medical Gazette article after observing it incidentally while conducting an autopsy on a 34-year-old woman with stunted development [2]. It has repeatedly been vaguely misattributed to a Dr. Balington in 1862, which may have been due to a self-perpetuating error by Robicsek et al or publisher from 1969 upon the first documented in vivo encounter and surgical treatment of a QAV [3]. Coincidentally, in the very same issue of The American Journal of Cardiology as the aforementioned Robicsek article, Peretz et al reported the first QAV diagnosis by way of aortography [4].
The estimated incidences of QAVs ranges from as low as 0.003% to as high as 1.46% [5], with its most commonly accepted incidence rate to be between 0.013% and 0.043% [6]. It has been found to have a significantly lower rate of incidences amongst the general patient population (0.008% to 0.033%) as compared to aortic valve replacement candidates (1.46%) [7]. Due to their rarity, QAVs may go undiagnosed without specific consideration, and thus the wide range of published incidences [8], although the numbers diagnosed have been on rise with echocardiographic imaging allowing the systematic study of a greater noncomplicated population [9]. The average age of diagnosis is 43.5 ± 21.8 years, with a range of 2 days to 84 years of age [10]. Subsequent surgical patients were approximately a decade younger when diagnosed than those who did not undergo surgical correction, although there was no significant difference between survival rates of the two groups. Similarly, there was no meaningful distinction between survival rates of QAV and non-QAV patient populations when matched for sex and age. A small male predominance is generally acknowledged, although it has been proposed to be as high as 62%. However, one publication has documented a slightly-higher female prevalence of 52%, and claims the aforementioned male predominance was perhaps due to their higher likelihood of males undergoing aortic valve surgery, for which they accounted for 75% of cases [10]. A previous review on QAVs in 2011 documented 271 reported cases amongst medical publications [11]. Bicuspid (approximately 2% of the population) aortic valves are the most prevalent aortic anomaly [12], followed by unicuspid (0.02% [13]) then QAVs [14], although the borderline scarcity between unicuspid and QAVs generate conflicting data to said rates of occurrences [15]. There have only been eight reported cases of quinticuspid, also referred to as pentacuspid aortic valves as of 2016 [16]. Quadricuspid pulmonary valves are nine times more prevalent than QAVs, with a comparable minor male predominance [17].
About 18% [18] to 32% [10] of QAV patients present with an additional congenital heart defect, such as coronary artery and ostium abnormalities, atrial [19] and ventricular [20] septal defect (ASD and VSD, respectively), patent ductus arteriosus [21], tetralogy of Fallot [22], sinus of Valsalva fistula [23], subaortic fibromuscular stenosis [24], regurgitation [25] and prolapse [26] of the mitral valve, hypertrophic nonobstructive cardiomyopathy [27], and transposed great arteries [28]. The most common cardiovascular irregularities observed with QAV are deformities in coronary arteries and ostia [27], with atypical coronary arteries, usually singular, associated with 10% of cases; this is of particular significance due to a reported sudden cardiac death of a previously unremarkable 16-year-old while walking owed to a left coronary ostium dome-like occlusion, with ventricular fibrillation noted as the immediate cause of death [29]. Furthermore, a single case has been reported in a patient with Ehlers-Danlos syndrome [18], as well as another case amongst identical twins [30]. QAVs’ correlation with aortic irregularities is ambivalent; one publication reported it was not associated with aortic dilation (unlike bicuspid aortic valves) [9], while another found common concurrence with ascending aortic dilation and aneurysms [31].
| Classifications | ▴Top |
There are two utilized QAV anatomical classification systems. The first one is Hurwitz and Roberts’s classification system, seven subtypes were included, lettered A to G, based on the four cusps’ relative sizes [6], with an additional type H supplemented by Vali et al [32] (Table 1 [8], Fig. 1). Based on their findings, approximately 85% of QAVs are of type A, B, or C. Based on a review of the literature by Timperley et al, type B has been reported as the most prevalent [8], although a later meta-analysis supported type A as being the most common [33].
 Click to view | Table 1. Hurwitz and Roberts’s Seven Subtypes With an Additional Type H |
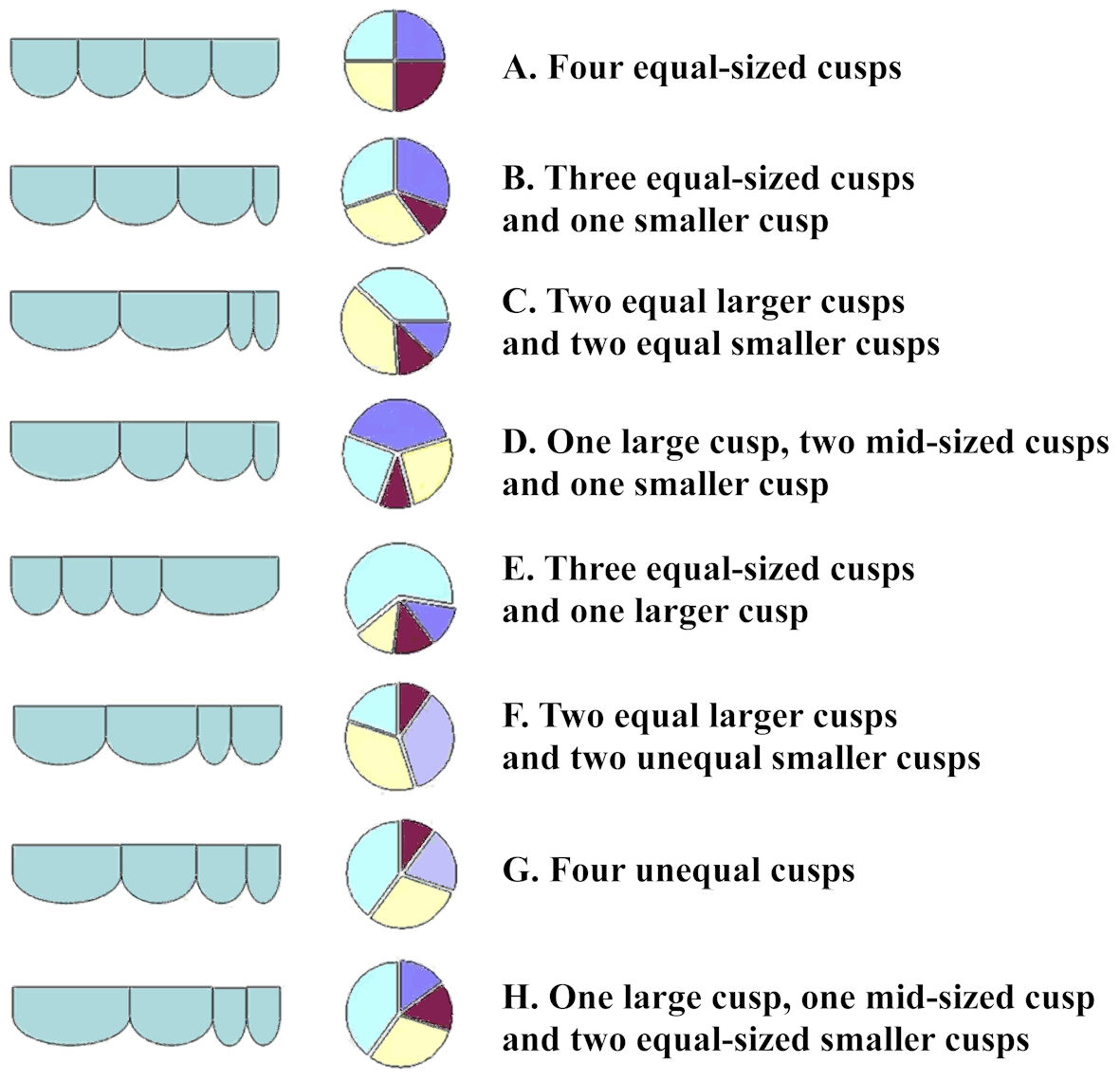 Click for large image | Figure 1. Hurwitz and Roberts’ classification subtypes of quadricuspid aortic valves, including Vali et al’s type H supplement. The figure was reprinted with permission from Yuan [38]. |
The second one is Nakamura’s classification system, four subtypes, numbered I to IV, based on the supernumerary cusps’ relative position to the left, right, and noncoronary cusps (Table 2 [34], Fig. 2) were included. According to this classification’s initial publication, the most frequent type encountered is type II, with types I and II respectively corresponding to Hurwitz and Roberts types A and B.
Click to view | Table 2. Nakamura’s Four Subtypes |
 Click for large image | Figure 2. Nakamura’s simplified classification subtypes of quadricuspid aortic valves. S: supernumerary cusp; R: right coronary cusp; L: left coronary cusp; N: noncoronary cusp. The figure was reprinted with permission from Yuan [38]. |
However, it should be noted that the most commonly used Hurwitz and Roberts’s classification system, as well as Nakamura’s by its namesake’s own admission, often lacks correspondence with patient treatment and management, as well as with surgical and echocardiographic findings. Thus, additional subtyping categories have been proposed, such as a condensed revision of Hurwitz and Robert’s seven subtypes into four concerning their clinical implications on management by Jagannath et al [11].
| Causes | ▴Top |
QAVs have been reported in both human and non-human mammals, such as dogs, shrews, and hamsters [35]. Furthermore, it has been established that arterial valvulogenesis does not differ considerably between human and non-human mammals [36]. Both the aortic and pulmonic semilunar valves emerge from mesenchymal ridges in the post-division truncus arteriosus, with the usual three nodules materializing within the vascular lumen after arterial trunk septation during the fifth and ninth weeks of gestation at the junction between the conus and truncus in the aortic and pulmonary ridges [37]. Irregular aortic valves can occur from disordered semilunar cusps primordia development within the aortic trunk wall [33]. The specific etiology of QAVs is yet undetermined [8]. Multiple pathophysiological mechanisms at various points of development have been proposed that might alter the valve cusp number, such as irregular septation of the conotruncus causing unequal distribution of the distention in each of the great arteries, anomalous proliferation of mesenchymal ridges, or valve cusp division during its formation [37]. The current leading hypothesis involves the partition of one of the three valve cushions due to an invagination of the endothelial layer on the luminal side during an early stage of valve development [35].
| Mode of Presentation | ▴Top |
QAV patients may be asymptomatic until their sixth decade, with subsequent symptoms experienced correlating with the valve’s functional status and any associated abnormalities [38]. Congestive heart failure is the most common prevailing presenting diagnosis. As previously mentioned, QAVs can be nonpathological, with symptomatic degeneration cases often associated with prolapsing, conjoint larger cusps, and poor coaptation due to smaller cusps [39].
The most common clinical manifestation observed is aortic regurgitation (AR) without aortic stenosis due to chronic aortic insufficiency (AI) [38]. Tutarel et al reported the following in QAV cases: pure AR in 74.7%, AR with stenosis in 8.4%, pure stenosis in 0.7%, and normal function in 16.2% [40]. It has been proposed that Hurwitz and Roberts’ type B have a higher likelihood of developing AR due to the single undersized cusp progressively leading to uneven stress distribution, trauma, and malcoaptation [41], although it has also been suggested that AR is just as likely with type A [8]. The most commonly accepted explanation proposed for said AR is unequal shear stress leading to progressive leaflet fibrosis and partial coaptation eventually failing. Notably, the accessory cusps location has not been found to correspond with the likelihood of developing AR [42].
Ninety-six percent of QAV patients had an adequate assessment of their ascending aorta at the time of initial diagnosis [10]. Aortic dimensions changes were noted by serial echocardiography in 40% of patients, although there was no significant correlation between said changes over time and QAV subtypes (P = 0.64), nor history of hypertension (P = 0.64). There has been one published case in which AI resulting from a QAV progressed to aortic disease, ultimately concluding in patient mortality due to cardiac tamponade after an ascending aortic aneurysm [43].
Structural valve degeneration can increase susceptibility to certain cardiac pathologies, such as rheumatic valves and bacterial endocarditis, which may mask or complicate QAV diagnosis [44]. The associated risk of infective endocarditis was recorded in 1.4% of QAV cases [9], with a small supernumerary cusp as an anticipating risk factor [44]. This risk is believed to be lessened in patients with Hurwitz and Roberts’ type A/Nakamura type I, as the equally-sized cusps lack asymmetry or flow disturbance. Diagnosis of a QAV with AR has been recognized as an important risk factor for endocarditis [45], although the American College of Cardiology/American Heart Association’s (ACC/AHA) 2008 guidelines for infective endocarditis do not advise prophylactic antibiotic treatment for patients unless an active infection is detected [46]. Nevertheless, some physicians still propose unconditional prophylactic antibiotic use [47], while others advise prophylactics solely for patients with unequal-sized cusps and AR [44].
| Diagnosis | ▴Top |
As most patients present associated symptoms before diagnostic procedures are undertaken, the majority of QAV-presenting cases are only found to be such in their later years. As compared to other aortic valve anatomies, QAV patients may present with AR and be symptomatic at relatively earlier age [48]. When combined with additional congenital heart defects [49] or presented as a diastolic heart murmur [50], QAV is sometimes incidentally discovered in pediatric patients. Differential diagnosis signs can include valve neoplastic involvement, valvular degeneration with or without calcifications, and adherent thrombus or vegetations, such as aortic valve tumors (e.g., papillary fibroelastoma, myxoma) [51]. Pseudo-QAVs can be produced by rheumatic fever and bacterial endocarditis amongst other severe bacterial infections, by way of inflammation precipitating septation of a normal valve cushion [52]. True congenital QAVs can be distinguishable by the presence of corpus nodules of Arantius at the center of the free border on each of the four valve’s cusps [52].
Modern technological advancements in common clinical practice diagnostics have contributed to a recent increase in QAV detection, as more than 80% of reports have been published after 1980, with echocardiography responsible for 60% of such [33]. Presently, most QAV diagnoses (51.1%) [33] are made via two-dimensional transthoracic [53] or real-time three-dimensional transesophageal echocardiography (TTE and TEE, respectively). TTE was initially employed in the 1970s, and was first utilized for QAV detection in 1984 [54, 55]. TTE and TEE can both visualize aortic valve morphology (i.e., cusp number and thickening degree, plus possible vegetations), as well as the size of the aortic root and left ventricle [56], with TEE being the more sensitive method as it can additionally visualize the coronary ostia. However, echocardiography in practice is operator-dependent, and its quality and usefulness can be compromised by either suboptimal acoustic windows or inapt subject body habitus [57]. A short-axis view of the aortic valve produces the most effective visualization for QAV identification and examination (i.e., number, thickening, mobility) as it produces a distinct “X” diastolic shape as opposed to the usual “Y” from tricuspid aortic valves [11], and a rectangular systolic character [54] (Fig. 3). If the valvular anatomy is uncertain, differential diagnosis can involve a multitude of possible explanations, such as valve neoplastic involvement, valvular degeneration (with possible calcification), adherent thrombus, or vegetations [51]. Likewise, while echocardiography can infer leaflet size, surgical findings do not always compare [8].
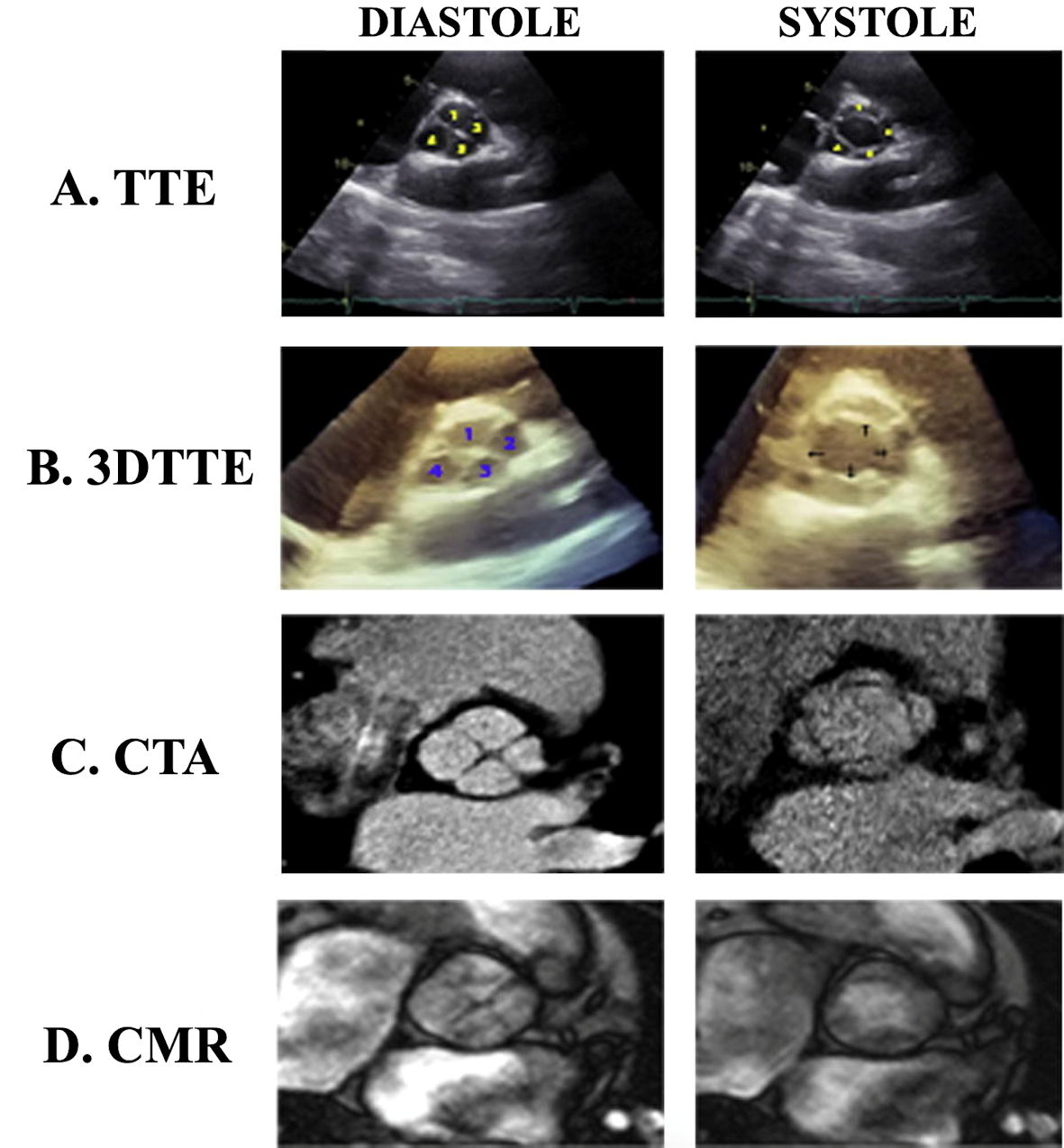 Click for large image | Figure 3. A Hurwitz and Roberts’ type A/Nakamura type I quadricuspid aortic valve visualized by various imaging methods in both diastolic and systolic phases. TTE: transthoracic echocardiography; 3DTTE: three-dimensional TTE; CTA: computed tomography angiogram; CMR: cardiac magnetic resonance imaging. The figure was reprinted with permission from Malviya et al [56]. |
Fewer recent cases of QAV have been initially detected by the relatively historical methods of surgical examination (22.6% of documented incidences) and pathological inspection (15.6%), and rarely is it diagnosed by aortography (6.5%) or the few cases by cardiac magnetic resonance imaging (CMR) [52]. It has been proposed that future cardiac imaging, and thus QAV diagnoses will be conducted by ways of emerging methods such as CMR and multi-detector cardiac computerized tomography (CCT) via cross-sectional imaging [58]; however, TEE is still the most popular current diagnostic modality by a significant margin. In addition to diagnoses, CMR can detect QAV morphology, AR presence and volume, valve stenosis due to calcification, cardiac function and chamber sizes, as well as possible associated disorders (e.g., stenotic pulmonary valve, hypertrophic cardiomyopathy, a patent ductus arteriosus, sinus of Valsalva aneurysm, and coronary artery conditions [52]) [59, 60]. CCT can likewise detect all the preceding as well as coronary ostia location and aorta dimensions [61]. Color Doppler is customarily used to confirm and evaluate the severity of AR diagnosis with central jet stemming from incomplete cusp coaptation [9, 56].
| Management | ▴Top |
QAV surgical indications include severe aortic stenosis [62], but principally severe AR and dysfunctional QAV linked with other lesions (e.g., left coronary ostium occlusion) [10]. The various methods by which these can be surgically corrected include biological or mechanical valve implantation, Ross procedure, Bentall procedure, and bi-/tricuspidization (with or without root replacement) [63]. Approximately one-fifth of QAV cases require surgical intervention, with valve repair, via the aforementioned methods collectively referred to as aortic valve reconstruction surgery (AVRS), favored versus replacement [48]. Upon a separate review of 186 QAV cases, 45.2% of instances required surgery usually during their fifth to sixth decades [33], while in another publication 66.7% (26/39) of QAV patients with AR necessitated surgical replacement of their aortic valve [27]. The average age for QAV valve replacement amongst 46 documented cases is 54 years [56], with the youngest patient having been 5 years old [64]. If feasible, particularly among younger candidates, repair is preferred as to avoid valve replacement-associated risks such as bleeding, endocarditis, thromboembolism, and prosthetic valve deterioration [48]. Among 31 QAV patients undergoing surgery, 23 (73%) were replaced while seven (23%) were repaired [39].
The objective of AVRS is to reestablish proper coaptation while minimizing transvalvular gradient and turbulent flow to achieve lasting durability [65]. This intention is predominantly undertaken by varied tricuspidization techniques, although QAV bicuspidization has been documented twice [38]. Bicuspidization was first reported in 2010 by Luciani et al as the four unequaled cusps of a Hurwitz and Roberts’ type G QAV posed geometrical challenges hindering tricuspidization [66]. Shimamoto et al published the second instance of QAV bicuspidization in 2014 after an unsuccessful tricuspidization produced an incompetent valve, although they still recommend routinely attempting tricuspidization first as it is surgically simpler and physiologically corresponds better [67]. The decision between reconstructive procedures is commonly determined based on the severity of the disorder, QAV condition, and surgeon’s predilection [39]. Surgical decision making can be influenced by a multitude of factors, including patient symptoms, AR severity, left ventricular dilation or dysfunction, and corresponding aortopathy with aneurysm [68]. Tricuspidization appears to be most appropriate in cases of two normal and two smaller leaflets (Hurwitz and Roberts’ types F and G), or in the case of three larger and one smaller leaflets (type B) [11]. Bicuspidization seems more applicable in cases of two larger leaflets each being combined with two smaller leaflets (types C, F, and G). Fewer coaptation lines have yielded superior valve competence in both bicuspid and tricuspid aortic valves, and thus tricuspidization of a QAV is often favored [48]. Regardless of the methodology employed, the surgery can be performed by way of a standard median sternotomy with cardiopulmonary bypass alongside retrograde or antegrade cold blood cardioplegia to arrest the heart [65]. Supplemental leaflet length can be added when necessary by tissue patch material, either as native or bovine pericardium [11].
Additionally, a few Ross procedures (subcoronary inclusion technique), also known as pulmonary autograft procedures, have successfully treated QAV while reducing aortic root dilation risk [69]. Compared with traditional mechanical or bioprosthetic replacements, autografting a patient’s own pulmonary valve (identical in size, shape, and strength to their aortic valve) minimizes future valve re-replacement probability and does not require lifetime blood thinner medication use [70]. Manouguian technique (posterior aortic annulus enlargement) was once reported on a Hurwitz and Roberts’ type A QAV patient with narrow annulus alongside aortic steno-insufficiency and mitral insufficiency [25]. In one study on 31 QAV patients requiring surgery, 40% had corresponding aortic dilation, and 23% underwent correlated aortic resectioning [40].
A less invasive and significantly less popular alternative to AVRS specifically for stenosed QAVs is transcatheter aortic valve replacement (TAVR), also referred to as transcatheter aortic valve implantation (TAVI), with its first documented case and TAVR/TAVI as its treatment published in 2011 by Blanke et al [71]. This percutaneous intervention is especially favored for patient candidates considered intermediate to high risk for AVRS complications, but can still require patients to spend the night of procedure in the intensive care unit for monitoring, and generally 2 to 5 days in the hospital for recovery.
Postoperative complications are rare [38]. Noted postoperative complications include: progressive AR [10], cardiac arrest, transient ischemic attack (TIA), third-degree atrioventricular (AV) block [72], thromboembolism, prosthetic valve endocarditis, and bleeding [73]. The overall survival rates of QAV patients are 89.9% at 5-year and 84.9% at 10-year follow-ups [10]. Nonetheless, an accurate prognosis of repair durability is undetermined due to insufficient cases and scant reporting regarding long-term patient outcomes [48]. Valve replacement with standard suturing technique does increase the risk of complete AV heart block due to the accessory cusp being predominantly located above the membranous septum in between the right coronary and the noncoronary cusps [72]. It has been proposed that said endangerment can be avoided by utilizing pledgeted sutures on the accessory leaflet, from exterior of the sinus of Valsalva to superior of the aortic annulus [74]. TAVR/TAVI carries with it its own risks [75]: most notably stroke which generally occurs in the immediate postprocedural period [76]; other less severe complications include paravalvular AR, conduction disturbances (particularly new-onset left bundle branch blockage), and least of all vascular complications [75].
| Follow-Up | ▴Top |
Due to the aforementioned small number of QAVs documented in medical literature, its natural history of disease is not of defined conclusions [9]. Nonpathological QAV cases still justify attentive recurring monitoring and clinical follow-ups, as frequently the valve can develop progressive hemodynamic concessions [77]. This is especially true for younger QAV-presenting patients, considering their recurrent need for AVRS later in life [8]. The median follow-up time post-AVRS was 38 months [39].
Echocardiograms are customarily performed both pre- and postoperative alongside surgical correction, as well as at hospital discharge and annually if no complications present [65]. Long-term follow-ups to gauge the lastingness of an operation are warranted as this is still a relatively rare occurrence with only a few recent review publications [65]. Withal, surgical tricuspidization is expected to be the future clinical standard treatment option for patients presenting QAV with AR, as it has previously shown to achieve durability and proper coaptation including low valve gradient sans turbulent flow [65].
The proportionate lack of observed aortic aneurysms is to be noted for scientific and treatment consequences, and thus histological and clinical studies of said in QAV cases show potential considerations for future research [11].
| Conclusions | ▴Top |
QAV is a rare congenital defect meriting specific attention. The majority of patients develop progressive aortic regurgitation sans stenosis. It is occasionally concurrent with ancillary cardiovascular congenital defects, most commonly with the coronary artery. Most cases are diagnosed via echocardiography while 20% of cases necessitate surgical correction rarely with complications. Also, as mentioned throughout this paper, there are many conflicting data points regarding QAV statistics, which we believe merits meta-analysis clarification, especially considering the recent breakthroughs in diagnostics leading to a relative surge of documented cases.
Acknowledgments
Figures 1 and 2 were reproduced, with permission, from Yuan [38]. Figure 3 were reproduced, with permission, from Malviya et al [56].
Financial Disclosure
No financial disclosure or funding was sought for this study.
Conflict of Interest
The authors have no conflict of interest to declare.
Author Contributions
Dr. Shivan Saith (primary author): responsible for collecting the review material and putting together the manuscript. Dr. Sunil Saith (co-author): responsible for review/oversight. Dr. Avinash Murthy: concept/design, drafting article and approval of article.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Perloff JK. The Howard Gilman Foundation Lecture. Where have we come from and where are we going? Valve management past, present and future. Adv Cardiol. 2004;41:1-8.
- Bietry RE, Freedberg RS, Saric M. Benjamin Babington and the quadricuspid aortic valve. Ann Intern Med. 2013;159(3):228-229.
doi pubmed - Robicsek F, Sanger PW, Daugherty HK, Montgomery CC. Congenital quadricuspid aortic valve with displacement of the left coronary orifice. Coll Works Cardiopulm Dis. 1968;14:87-90.
- Peretz DI, Changfoot GH, Gourlay RH. Four-cusped aortic valve with significant hemodynamic abnormality. Am J Cardiol. 1969;23(2):291-293.
doi - Yotsumoto G, Iguro Y, Kinjo T, Matsumoto H, Masuda H, Sakata R. Congenital quadricuspid aortic valve: report of nine surgical cases. Ann Thorac Cardiovasc Surg. 2003;9(2):134-137.
- Hurwitz LE, Roberts WC. Quadricuspid semilunar valve. Am J Cardiol. 1973;31(5):623-626.
doi - Tsukioka K, Nobara H, Takano T, Wada Y, Amano J. Quadricuspid aortic valve with ascending aortic aneurysm: a case report and histopathological investigation. Ann Thorac Cardiovasc Surg. 2011;17(4):418-421.
doi pubmed - Timperley J, Milner R, Marshall AJ, Gilbert TJ. Quadricuspid aortic valves. Clin Cardiol. 2002;25(12):548-552.
doi pubmed - Savino K, Quintavalle E, Ambrosio G. Quadricuspid Aortic Valve: A Case Report and Review of the Literature. J Cardiovasc Echogr. 2015;25(3):72-76.
doi pubmed - Tsang MY, Abudiab MM, Ammash NM, Naqvi TZ, Edwards WD, Nkomo VT, Pellikka PA. Quadricuspid aortic valve: characteristics, associated structural cardiovascular abnormalities, and clinical outcomes. Circulation. 2016;133(3):312-319.
doi pubmed - Jagannath AD, Johri AM, Liberthson R, Larobina M, Passeri J, Tighe D, Agnihotri AK. Quadricuspid aortic valve: a report of 12 cases and a review of the literature. Echocardiography. 2011;28(9):1035-1040.
doi pubmed - Roberts WC. The congenitally bicuspid aortic valve. A study of 85 autopsy cases. Am J Cardiol. 1970;26(1):72-83.
doi - Novaro GM, Mishra M, Griffin BP. Incidence and echocardiographic features of congenital unicuspid aortic valve in an adult population. J Heart Valve Dis. 2003;12(6):674-678.
- Falcone MW, Roberts WC, Morrow AG, Perloff JK. Congenital aortic stenosis resulting from a unicommisssural valve. Clinical and anatomic features in twenty-one adult patients. Circulation. 1971;44(2):272-280.
doi pubmed - Zhu J, Zhang J, Wu S, Zhang Y, Ding F, Mei J. Congenital quadricuspid aortic valve associated with aortic insufficiency and mitral regurgitation. J Cardiothorac Surg. 2013;8:87.
doi pubmed - Al Mehisen R, El Essely R, Al-Mallah M, Al-Mohaissen MA, Kashour T. Quadricuspid aortic valve, single coronary artery, solitary kidney and oblique facial cleft. A unique constellation of congenital abnormalities: case report and review of the literature. J Genet Syndr Gene Ther. 2016;7(2).
doi - Davia JE, Fenoglio JJ, DeCastro CM, McAllister HA, Jr., Cheitlin MD. Quadricuspid semilunar valves. Chest. 1977;72(2):186-189.
doi pubmed - Dotti MT, De Stefano N, Mondillo S, Agricola E, Federico A. Neurological involvement and quadricuspid aortic valve in a patient with Ehlers-Danlos syndrome. J Neurol. 1999;246(7):612-613.
doi pubmed - Sousa L, Pinto F, Nogueira G, Kaku S, Antunes AM. Quadricuspid aortic valve and atrial septal defect. Rev Port Cardiol. 2001;20(3):329-330.
- Demirkol S, Balta S, Arslan Z, Unlu M, Kucuk U, Iyisoy A. Association of quadricuspid aortic valve and ventricular septal defect in a patient who had undergone atrial septal defect surgery. Kardiol Pol. 2013;71(5):546.
doi pubmed - Seol SH, Kim U, Cho HJ, Kim DK, Kim DI, Kim DS. Quadricuspid aortic valve with patent ductus arteriosus. Tex Heart Inst J. 2010;37(6):726-727.
- Suzuki Y, Daitoku K, Minakawa M, Fukui K, Fukuda I. Congenital quadricuspid aortic valve with tetralogy of Fallot and pulmonary atresia. Jpn J Thorac Cardiovasc Surg. 2006;54(1):44-46.
doi pubmed - Egred M, Patel JC, Metcalfe MJ. Sinus of Valsalva fistula with quadricuspid aortic valve, a first reported association. Int J Cardiol. 2005;101(1):151-152.
doi pubmed - Iglesias A, Oliver J, Munoz JE, Nunez L. Quadricuspid aortic valve associated with fibromuscular subaortic stenosis and aortic regurgitation treated by conservative surgery. Chest. 1981;80(3):327-328.
doi pubmed - Sakamoto Y, Saitoh F, Ohnishi K, Kurosawa H, Takakura H. [A case of quadricuspid aortic valve associated with mitral insufficiency]. Nihon Kyobu Geka Gakkai Zasshi. 1994;42(8):1235-1237.
- Konrad R, Natividade M, Costa S, Salame CK. Valva Aortica Quadricuspide: uma Revisao Completa Quadricuspid Aortic Valve: a complete review. Rev bras ecocardiogr imagem Cardiovasc. 2009;22(3):39-52.
- Janssens U, Klues HG, Hanrath P. Congenital quadricuspid aortic valve anomaly associated with hypertrophic non-obstructive cardiomyopathy: a case report and review of the literature. Heart. 1997;78(1):83-87.
doi pubmed - Erdmenger J, Vazquez-Antona C, Becerra R, Romero A, Roldan J, Buendia A, Vargas-Barron J. [Quadricuspid aortic valve in a patient with d-transposition of the great arteries]. Arch Cardiol Mex. 2005;75(4):460-462.
- Kurosawa H, Wagenaar SS, Becker AE. Sudden death in a youth. A case of quadricuspid aortic valve with isolation of origin of left coronary artery. Br Heart J. 1981;46(2):211-215.
doi pubmed - Fratellone P, Berger M, Khan M, Bassiri-Tehrani M. Quadricuspid aortic valve diagnosed by echocardiography in two cases identical twins. Am J Cardiol. 2007;100(9):1490-1491.
doi pubmed - Song I, Park JA, Choi BH, Ko SM, Shin JK, Chee HK, Kim JS. Morphological and functional evaluation of quadricuspid aortic valves using cardiac computed tomography. Korean J Radiol. 2016;17(4):463-471.
doi pubmed - Vali Y, Rajendra R, Nishtar S. A previously undescribed type of quadricuspid aortic valve: type H. J Heart Valve Dis. 2010;19(6):792-793.
- Tutarel O. The quadricuspid aortic valve: a comprehensive review. J Heart Valve Dis. 2004;13(4):534-537.
- Nakamura Y, Taniguchi I, Saiki M, Morimoto K, Yamaga T. Quadricuspid aortic valve associated with aortic stenosis and regurgitation. Jpn J Thorac Cardiovasc Surg. 2001;49(12):714-716.
doi pubmed - Lopez-Garcia A, Carmen Fernandez M, Duran AC, Sans-Coma V, Fernandez B. Quadricuspid aortic valves in Syrian hamsters and their formation according to current knowledge on valvulogenesis. Jpn J Vet Res. 2015;63(1):37-43.
- Fernandez B, Duran AC, Fernandez-Gallego T, Fernandez MC, Such M, Arque JM, Sans-Coma V. Bicuspid aortic valves with different spatial orientations of the leaflets are distinct etiological entities. J Am Coll Cardiol. 2009;54(24):2312-2318.
doi pubmed - Gulyasy B, Lopez-Candales A, Reis SE, Levitsky S. Quadricuspid aortic valve: an unusual echocardiographic finding and a review of the literature. Int J Cardiol. 2009;132(2):e68-71.
doi pubmed - Yuan SM. Quadricuspid aortic valve: a comprehensive review. Braz J Cardiovasc Surg. 2016;31(6):454-460.
doi pubmed - Idrees JJ, Roselli EE, Arafat A, Johnston DR, Svensson LG, Sabik JF, 3rd, Pettersson GB. Outcomes after repair or replacement of dysfunctional quadricuspid aortic valve. J Thorac Cardiovasc Surg. 2015;150(1):79-82.
doi pubmed - Tutarel O, Westhoff-Bleck M. Functional status of the quadricuspid aortic valve/an uncommon coincidence of congenital quadricuspid aortic valve accompanied by hypertrophic obstructive cardiomyopathy. Anadolu Kardiyol Derg. 2008;8(1):86; author reply 86-87.
- Feldman BJ, Khandheria BK, Warnes CA, Seward JB, Taylor CL, Tajik AJ. Incidence, description and functional assessment of isolated quadricuspid aortic valves. Am J Cardiol. 1990;65(13):937-938.
doi - Naito K, Ohteki H, Yunoki J, Hisajima K, Sato H, Narita Y. Aortic valve repair for quadricuspid aortic valve associated with aortic regurgitation and ascending aortic aneurysm. J Thorac Cardiovasc Surg. 2004;128(5):759-760.
doi pubmed - Massoni F, Ricci S. Death from ascending aortic aneurysm secondary to quadricuspid aortic valve. Am J Forensic Med Pathol. 2014;35(4):232-233.
doi pubmed - Takeda N, Ohtaki E, Kasegawa H, Tobaru T, Sumiyoshi T. Infective endocarditis associated with quadricuspid aortic valve. Jpn Heart J. 2003;44(3):441-445.
doi pubmed - Bilge AK, Bugra Z, Tayyareci Y, Ruzgar O, Umman S, Meric M. An uncommon coincidence of congenital quadricuspid aortic valve accompanied by hypertrophic obstructive cardiomyopathy. Anadolu Kardiyol Derg. 2007;7(4):E7-8.
- Nishimura RA, Carabello BA, Faxon DP, Freed MD, Lytle BW, O'Gara PT, O'Rourke RA, et al. ACC/AHA 2008 Guideline update on valvular heart disease: focused update on infective endocarditis: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52(8):676-685.
doi pubmed - Kawanishi Y, Tanaka H, Nakagiri K, Yamashita T, Okada K, Okita Y. Congenital quadricuspid aortic valve associated with severe regurgitation. Asian Cardiovasc Thorac Ann. 2008;16(5):e40-41.
doi pubmed - Schmidt KI, Jeserich M, Aicher D, Schafers HJ. Tricuspidization of the quadricuspid aortic valve. Ann Thorac Surg. 2008;85(3):1087-1089.
doi pubmed - Tayama E, Chihara S, Kosuga T, Akasu K, Kawano H, Ohashi M, Fukunaga S, et al. A case report of surgical treatment of quadricuspid aortic valve associated with regurgitation. Ann Thorac Cardiovasc Surg. 2000;6(2):130-133.
- Brock M, Tugertimur A, Schwartz MC. A rare pediatric cardiac anomaly: Quadricuspid aortic valve with aortic regurgitation. Ann Pediatr Cardiol. 2013;6(2):202-203.
doi pubmed - Franco A, Gabriel S, Ruehm SG. The quadricuspid aortic valve. J Radiol Case Rep. 2014;8(11):25-29.
doi pubmed - Khan SK, Tamin SS, Araoz PA. Quadricuspid aortic valve by cardiac magnetic resonance imaging: a case report and review of the literature. J Comput Assist Tomogr. 2011;35(5):637-641.
doi pubmed - Kanda H, Kunisawa T, Iida T, Kanao M, Toyama Y, Iwasaki H. Quadricuspid aortic valve detected by three-dimensional transesophageal echocardiography. J Cardiothorac Vasc Anesth. 2015;29(3):e33-35.
doi pubmed - Herman RL, Cohen IS, Glaser K, Newcomb EW, 3rd. Diagnosis of incompetent quadricuspid aortic valve by two-dimensional echocardiography. Am J Cardiol. 1984;53(7):972.
doi - Chandrasekaran K, Tajik AJ, Edwards WD, Seward JB. Two-dimensional echocardiographic diagnosis of quadricuspid aortic valve. Am J Cardiol. 1984;53(11):1732-1733.
doi - Malviya A, Kumar P, Mishra J, Srivastava P. Egyptian Society of Cardiology Quadricuspid aortic valve - A case report and literature review. Egypt Hear J. 2016;68(4):271-275.
doi - Tanaka R, Yoshioka K, Niinuma H, Ohsawa S, Okabayashi H, Ehara S. Diagnostic value of cardiac CT in the evaluation of bicuspid aortic stenosis: comparison with echocardiography and operative findings. AJR Am J Roentgenol. 2010;195(4):895-899.
doi pubmed - Pulcino A, Sordelli C, Ismeno G, Tritto FP, Golino P, Piazza L. A case of quadricuspid aortic valve characterized by echocardiography and magnetic resonance imaging. Monaldi Arch Chest Dis. 2011;76(3):146-148.
doi pubmed - Pouleur AC, le Polain de Waroux JB, Pasquet A, Watremez C, Vanoverschelde JL, El Khoury G, Gerber BL. Successful repair of a quadricuspid aortic valve illustrated by transoesophageal echocardiography, 64-slice multidetector computed tomography, and cardiac magnetic resonance. Eur Heart J. 2007;28(22):2769.
doi pubmed - Kajinami K, Takekoshi N, Mabuchi H. Images in cardiology. Non-invasive detection of quadricuspid aortic valve. Heart. 1997;78(1):87.
doi pubmed - Chapman CB, Kohmoto T, Kelly AF, Thornton F, Keevil JG. Cardiac computed tomography and quadricuspid aortic valve: a case report. WMJ. 2010;109(4):219-221.
- Mecozzi G, Pratali S, Milano A, Nardi C, Bortolotti U. Severe quadricuspid aortic valve stenosis after mediastinal irradiation. J Thorac Cardiovasc Surg. 2003;126(4):1198-1199.
doi - Yamanaka K, Okada K, Okita Y. Aortic root replacement with a valve-sparing technique for quadricuspid aortic valve. Eur J Cardiothorac Surg. 2015;47(4):741-743.
doi pubmed - Rosenkranz ER, Murphy DJ, Jr., Cosgrove DM, 3rd. Surgical management of left coronary artery ostial atresia and supravalvar aortic stenosis. Ann Thorac Surg. 1992;54(4):779-781.
doi - Song MG, Yang HS, Lee DH, Shin JK, Chee HK, Kim JS. Mid-term results in patients having tricuspidization of the quadricuspid aortic valve. J Cardiothorac Surg. 2014;9:29.
doi pubmed - Luciani GB, Morjan M, Faggian G, Mazzucco A. Repair of quadricuspid aortic valve by bicuspidization: a novel technique. Interact Cardiovasc Thorac Surg. 2010;11(3):348-350.
doi pubmed - Shimamoto T, Komiya T, Maruo T, Sakaguchi G. Tailor-made approach for quadricuspid aortic valve repair. Asian Cardiovasc Thorac Ann. 2014;22(4):472-474.
doi pubmed - Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Guyton RA, O'Gara PT, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Thorac Cardiovasc Surg. 2014;148(1):e1-e132.
doi - Misfeld M, Christiansen F, Sievers HH. Ross procedure in a quadricuspid aortic valve. Ann Thorac Surg. 2005;80(3):1110-1111.
doi pubmed - Bowdish ME, Kumar SR, Starnes VA. The Ross procedure: an excellent option in the right hands. Ann Transl Med. 2016;4(23):471.
doi pubmed - Blanke P, Wengenmayer T, Sorg S, Pache G. Stenosed quadricuspid aortic valve treated by transcatheter aortic valve implantation. J Am Coll Cardiol. 2011;57(14):1567.
doi pubmed - Pirundini PA, Balaguer JM, Lilly KJ, Gorsuch WB, Taft MB, Cohn LH, Rizzo RJ. Replacement of the quadricuspid aortic valve: strategy to avoid complete heart block. Ann Thorac Surg. 2006;81(6):2306-2308.
doi pubmed - Daprati A, Generali T, Arlati F, Roberto M. Quadricuspid aortic valve plasty: is it worth it to repair as an alternative to substitution? Ann Thorac Surg. 2013;95(1):e7-8.
doi pubmed - Kono T, Oda T, Akaiwa K, Nakamura K, Tanaka H. A case of a quadricuspid aortic valve identified preoperatively using transthoracic echocardiography. J Med Ultrason (2001). 2017;44(3):263-266.
doi pubmed - Agarwal S, Tuzcu EM, Krishnaswamy A, Schoenhagen P, Stewart WJ, Svensson LG, Kapadia SR. Transcatheter aortic valve replacement: current perspectives and future implications. Heart. 2015;101(3):169-177.
doi pubmed - Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-2198.
doi pubmed - Williams L, Peters P, Shah P. Tricuspidization of quadricuspid aortic valve. Ann Thorac Surg. 2013;95(4):1453-1455.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.