

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Short Communication
Volume 13, Number 2, April 2022, pages 110-117

Isolated Tricuspid Valve Replacement for Infective Endocarditis
Philip Y.K. Panga, d, Lily W.Y. Yangb, c, Ling Zhub, Yeow Leng Chuaa
aDepartment of Cardiothoracic Surgery, National Heart Centre Singapore, Singapore 169609, Singapore
bMinistry of Health Holdings, Singapore, Singapore
cYong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore
dCorresponding Author: Philip Y.K. Pang, Department of Cardiothoracic Surgery, National Heart Centre Singapore, Singapore 169609, Singapore
Manuscript submitted January 21, 2022, accepted February 5, 2022, published online March 12, 2022
Short title: Tricuspid Valve Surgery for Endocarditis
doi: https://doi.org/10.14740/cr1359
| Abstract | ▴Top |
Background: Existing data regarding isolated tricuspid valve replacement for primary tricuspid valve disease such as infective endocarditis (IE) are limited. The aim of this study was to review our experience of isolated tricuspid valve replacement for IE.
Methods: A retrospective review was performed to evaluate the perioperative and long-term outcomes of patients undergoing isolated tricuspid valve replacement for IE at our tertiary referral center between January 2000 and December 2014. Surgical outcomes were reviewed to include survival and postoperative complications.
Results: Seven patients underwent isolated tricuspid valve replacement for IE during the study period. Mean age was 41 ± 14 years with six (86%) males. Six patients (86%) were intravenous drug users. Five patients (71%) presented with septic emboli to the lungs. Five patients (71%) had active endocarditis at the time of surgery. The indications for surgery were heart failure in three patients (43%), persistent sepsis in three patients (43%) and both in one patient (14%). Methicillin-sensitive Staphylococcus aureus was the most common infective organism, isolated in five patients (71%). There were no in-hospital mortalities or permanent pacemaker implantations. Follow-up was completed in 86% of the cases. The median follow-up period was 13 months (range 2 to 129 months). Three patients (43%) died during the follow-up period, at 7 months, 8 months and 13 months, respectively. All deaths were associated with prosthetic valve IE and recurrent intravenous drug use.
Conclusions: This study supplements the paucity of data pertaining to tricuspid valve replacement for IE in the local population. Survival outcomes can be improved with prompt surgical intervention, optimal medical optimization, and a holistic, psychosocial approach targeting intravenous drug abuse.
Keywords: Tricuspid valve replacement; Tricuspid regurgitation; Infective endocarditis
| Introduction | ▴Top |
Tricuspid valve replacement (TVR) is an uncommon and challenging procedure, which has historically been associated with high mortality and morbidity [1]. It is indicated in both primary and secondary diseases of the tricuspid valve when valve repair is not possible or unsuccessful. When clinically severe, tricuspid regurgitation (TR) is associated with a poor prognosis, independent of age, pulmonary pressure, or biventricular systolic function [2, 3]. Tricuspid valve surgery is usually performed concomitantly during another cardiac procedure, usually involving the mitral valve. Isolated tricuspid valve surgery is uncommon and is required in < 10% of patients with tricuspid valve endocarditis [4, 5]. Existing data regarding isolated TVR for primary tricuspid valve disease such as infective endocarditis (IE) are limited, available mainly from single-center retrospective studies with small sample sizes.
| Materials and Methods | ▴Top |
This retrospective study was performed to evaluate the perioperative and long-term outcomes of patients undergoing isolated TVR for IE at our tertiary referral center between January 2000 and December 2014. The local Institutional Review Board approved this study (2015/2740), with a waiver of informed consent. This study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration. Data were extracted from electronic medical records and patient case notes. Adverse events were defined according to the guidelines for reporting morbidity and mortality after cardiac valve operations [6].
Definitions
In-hospital mortality was defined as all-cause mortality during the hospital stay for the surgical treatment of tricuspid valve IE. Active IE was defined as ongoing infection in a patient who was still receiving antibiotic therapy. Renal failure was defined as serum creatinine clearance levels lower than 60 mL/min as calculated with the Cockroft-Gault formula, or the need for renal replacement therapy.
Surgical technique
All operations were performed via median sternotomy using moderately hypothermic (30 - 32 °C) cardiopulmonary bypass (CPB), which was initiated via central cannulation of the ascending aorta and both vena cavae. Either a beating or rested heart approach was adopted for TVR, according to surgeon preference. In cases where the heart was arrested, myocardial protection was achieved via hyperkalemic hypothermic cardioplegia, using the antegrade approach, either alone or in combination with the retrograde technique. Flooding of the surgical field with carbon dioxide was applied in all cases. Intraoperative transoesophageal echocardiography was routinely performed in all cases.
| Results | ▴Top |
Demographics
Seven patients underwent isolated TVR for IE during the study period. Six patients (86%) were male. The mean age was 41.0 ± 14.1 years. Two patients (29%) presented in New York Heart Association (NYHA) functional class II, one (14%) in class III, and four (57%) in class IV. Six patients (86%) had a history of intravenous drug use (IVDU). Five patients (71%) had chronic hepatitis C infection. Five patients (71%) had septic emboli to the lungs prior to TVR. Methicillin-sensitive Staphylococcus aureus (MSSA) was the most commonly isolated organism causing IE, affecting five patients (71%), followed by methicillin-resistant Staphylococcus aureus (MRSA) in one patient (14%), and Streptococcus and Neisseria in one patient (14%). Five patients (71%) underwent TVR for active IE. The indications for surgery were heart failure in three patients (43%), persistent sepsis in three patients (43%), and both in one patient (14%). No patients had undergone previous open-heart surgery. Preoperative transoesophageal echocardiographic imaging and data were shown in Figure 1 and Table 1, respectively. All seven patients had severe TR. The average size of the tricuspid valve vegetations in the five patients with active IE was 24.6 ± 16.1 mm.
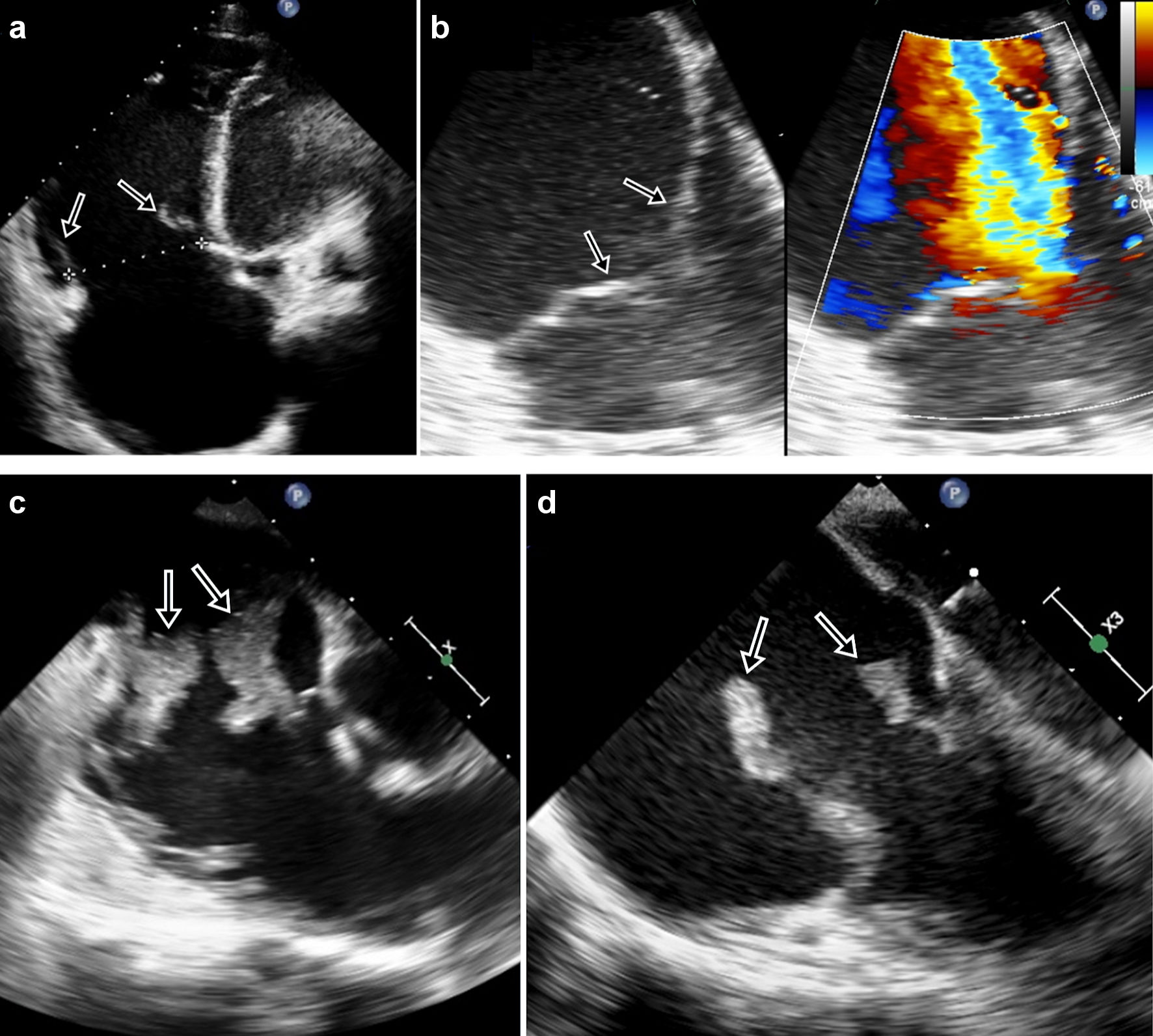 Click for large image | Figure 1. Preoperative echocardiography. (a, b) Treated endocarditis: (a) Severely dilated tricuspid valve annulus measuring 59 mm (arrows), with non-coapting tricuspid valve leaflets. (b) Dilated tricuspid valve annulus (arrows) measuring 39 mm, with central malcoaptation and severe tricuspid regurgitation. (c, d) Active endocarditis: large, mobile vegetations (arrows) on damaged tricuspid valve leaflets. |
 Click to view | Table 1. Preoperative Data |
Operative data
All surgeries were performed in the elective setting. Operative and postoperative data were shown in Table 2. The mean aortic cross clamp and CPB times were 49 min and 90 min, respectively. Mechanical valves were implanted in two patients (29%), and bioprosthetic valves in five patients (71%). Six patients (86%) were initially planned for valve replacement. One patient (14%) underwent TVR after failure of tricuspid valve repair.
Click to view | Table 2. Operative and Postoperative Data |
Early outcomes
One patient (14%) underwent re-exploration for postoperative mediastinal bleeding. No patients required a permanent pacemaker or implantable defibrillator. One patient (14%) suffered a sternal wound infection. Two patients (29%) developed postoperative pneumonia, likely precipitated by pre-existing septic emboli to the lung. The average length of stay was 34 days (range 7 to 60 days), attributed to prolonged antibiotic therapy for IE. Five patients (71%) showed improvement in their NYHA class after TVR. There were no in-hospital mortalities.
Late outcomes
Follow-up data were obtained by direct assessment during scheduled reviews at our institution. One foreign patient (14%) was lost to follow-up after returning to his native country. The median follow-up period was 13 months (range 2 to 129 months). One patient (14%) underwent reoperative TVR for prosthetic valve endocarditis 3 months after his initial surgery, but subsequently demised from recurrent prosthetic valve IE 4 months later. Three patients (43%) died during the follow-up period, including the patient who underwent reoperative TVR. All deaths were associated with recurrent IVDU and prosthetic valve IE after initial TVR, occurring at 7 months, 8 months and 13 months, respectively. One patient (14%) developed symptomatic tricuspid valve stenosis but declined reoperation.
Summary
Data of the seven patients undergoing isolated TVR for IE were summarized in Table 3.
Click to view | Table 3. Summary Table of Seven Patients Undergoing Isolated Tricuspid Valve Replacement for Infective Endocarditis |
| Discussion | ▴Top |
This study provides information on early and late clinical outcomes of patients undergoing isolated TVR for IE, in a cohort of relatively young patients. The majority of our patients had a history of IVDU. Valve replacement is preferred in cases of organic TR in which gross structural alterations preclude the success of repair, such as in endocarditis, rheumatic heart disease and myxomatous degeneration. In an earlier report from our institution, 10% of patients undergoing surgery for IE have a history of IVDU. The incidence of tricuspid valve IE was 63% in IV drug abusers compared to 4% in non-IV drug abusers (P < 0.001) [7]. The majority of patients in the present study were severely symptomatic, in NYHA class III or IV. Surgery improved symptoms in most patients. Despite their relatively young age, our patients had multiple laboratory derangements in keeping with their chronic disease and poor nutritional status.
TVR is a high-risk procedure associated with operative mortality of 17-22%, 5-year survival rates of 60-72%, and 10-year survival rates of 45-65% [8-10]. Our in-hospital mortality compares favorably to other studies. This is likely due to differences in the patient profile. Our patients had a relatively short history of IE with preserved right ventricular function, whereas previous reports describe patients with irreversible dilatation and dysfunction of the right ventricle. The consistently high late mortality rates of TVR have led authors to suggest that tricuspid valve disease requiring replacement may be a marker for end-stage valvular heart disease [8]. Pulmonary hypertension has been found to be a predictor of late mortality after TVR [11]. Postoperatively, no patient required a permanent pacemaker, compared to other TVR studies reporting pacemaker implantation rates of 9-28% [1, 12]. In a validated risk score, Koplan et al [13] identified the following (age exceeding 70 years, prior valve surgery and multivalvular procedures) as independent risk factors for pacemaker implantation after TVR. None of our patients had these risk factors.
At 13 months post-surgery, three patients (43%) from our cohort had died from prosthetic valve endocarditis. Prosthetic valve endocarditis is associated with a much higher mortality compared to native valve endocarditis [14]. Even with timely diagnosis, antibiotic therapy and reoperation, mortality ranges from 26% to 75% in medically treated patients and 23-43% in surgically treated patients [15]. Factors contributing to the risk of prosthetic valve endocarditis and reoperation include IVDU [16] and human immunodeficiency virus infection [17]. In a recent report from a multi-center Italian study involving 21 centers over a 35-year period, 157 of 4,069 patient (3.8%) underwent isolated tricuspid valve surgery for active IE. From the same study, the incidence of IVDU was 38%. Age, prosthetic valve IE, IVDU and permanent pacemaker leads were associated with increased recurrence of IE and poorer long-term survival [4]. Ongoing IVDU appears to be the greatest contributor towards mortality for IVDU-related tricuspid valve endocarditis [18]. In IVDUs, repeated exposure to particulate matter damages right-sided heart valves. Over time, this serves as a nidus for infection during skin flora-related episodes of bacteremia [19]. The recurrence of IVDU as a cause of prosthetic tricuspid valve endocarditis has poor prognostic implications in TVR. The management of IVDU patients involves both that of endocarditis, as well as the underlying drug addiction. Previous studies of IVDU-associated endocarditis have demonstrated survival benefits attributed to addiction treatment [20]. Several authors have proposed introducing addiction and psychiatric therapy in the inpatient and outpatient setting during the postoperative period, citing the impracticality of using drug abstinence as a requirement for surgery, as patients tend to present acutely [21]. In this unique patient population, it is prudent to tailor a psychosocial approach to treatment, including education, social support and drug rehabilitation.
There is currently no ideal approach for TVR. Several issues remain unresolved, in terms of the type of prosthesis, the surgical approach, and alternatives to valve replacement. The choice between mechanical and bioprosthetic valves remains controversial. In a 25-year study comparing mechanical and bioprosthetic TVR in 90 patients, the type of prosthesis was not shown to affect early and late mortality, or reoperation rate [8]. Mortality at 30-days and 5-years respectively was 15% and 27% in the mechanical group, compared to 21% and 30% in the bioprosthetic group, with no significant differences between the two (P = 0.354; P = 0.658). Freedom from reoperation at 5, 10, and 15 years were, 86%, 76%, and 70% in the mechanical group, versus 97%, 83%, and 57% in the bioprosthetic group (P = 0.762). A meta-analysis of 1,160 prostheses and 6,046 follow-up years showed no significant differences in survival and reoperation rates [22]. Current evidence does not support the use of one prosthesis over the other, and we believe that the choice should be individualized based on several factors, including age, projected lifespan, comorbidities, concomitant prosthetic valves and the patient’s informed choice. In our study, four of the six patients (67%) who were intravenous drug users underwent bioprosthetic valve replacement despite their relatively young age (range 27 - 46 years). This decision factored in their multiple comorbidities including chronic hepatitis C infection, bleeding risks associated with life-long anti-coagulation and likelihood of non-compliance to anti-coagulation.
All TVRs at our center were performed using a conventional open surgical approach. Novel transcatheter approaches in the treatment of TR are currently being developed, and some have successfully been implanted in humans [23], representing a potentially viable alternative to open TVR, and a modality for re-intervention after failed TVR. A multi-center French study has reported successful tricuspid valve-in-valve implantation of the Melody (Medtronic, Minneapolis, MN) and SAPIEN (Edwards Lifesciences, Irvine, CA) transcatheter valves in high-risk patients with failing tricuspid bioprostheses [24]. This could potentially be a treatment option for prohibitive or high-risk surgical patients, whose TR is not amenable to medical therapy alone.
Limitations
This study involved a retrospective analysis of a small cohort. Despite the long study period, the sample size was small as isolated TVR for IE is a rare procedure. Statistical power was limited.
Conclusions
This study supplements the paucity of data pertaining to TVR for IE. In recurrent intravenous drug users, survival outcomes can be improved with prompt surgical intervention, optimal medical optimization, and a holistic, psychosocial approach to address intravenous drug abuse.
Acknowledgments
The authors thank Clara Zhang and Selena Chew for their editorial assistance.
Financial Disclosure
No commercial or other sources of funding were received for this study.
Conflict of Interest
The authors have no conflict of interest to declare.
Informed Consent
The Institutional Review Board approved this study (2015/2740), with a waiver of informed consent.
Author Contributions
Conception and design: PYK Pang and YL Chua. Administrative support: PYK Pang, L Zhu, and LWY Yang. Provision of study materials or patients: PYK Pang and YL Chua. Collection and assembly of data: PYK Pang, L Zhu, and LWY Yang. Data analysis and interpretation: PYK Pang, L Zhu, LWY Yang, and YL Chua. Manuscript writing and final approval of manuscript: all authors.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
CPB: cardiopulmonary bypass; IE: infective endocarditis; IVDU: intravenous drug use; MRSA: methicillin-resistant Staphylococcus aureus; MSSA: methicillin-sensitive Staphylococcus aureus; NYHA: New York Heart Association; TR: tricuspid regurgitation; TVR: tricuspid valve replacement
| References | ▴Top |
- Moraca RJ, Moon MR, Lawton JS, Guthrie TJ, Aubuchon KA, Moazami N, Pasque MK, et al. Outcomes of tricuspid valve repair and replacement: a propensity analysis. Ann Thorac Surg. 2009;87(1):83-88; discussion 88-89.
doi pubmed - Topilsky Y, Nkomo VT, Vatury O, Michelena HI, Letourneau T, Suri RM, Pislaru S, et al. Clinical outcome of isolated tricuspid regurgitation. JACC Cardiovasc Imaging. 2014;7(12):1185-1194.
doi pubmed - Nath J, Foster E, Heidenreich PA. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004;43(3):405-409.
doi pubmed - Di Mauro M, Foschi M, Dato GMA, Centofanti P, Barili F, Corte AD, Ratta ED, et al. Surgical treatment of isolated tricuspid valve infective endocarditis: 25-year results from a multicenter registry. Int J Cardiol. 2019;292:62-67.
doi pubmed - Yong MS, Coffey S, Prendergast BD, Marasco SF, Zimmet AD, McGiffin DC, Saxena P. Surgical management of tricuspid valve endocarditis in the current era: A review. Int J Cardiol. 2016;202:44-48.
doi pubmed - Akins CW, Miller DC, Turina MI, Kouchoukos NT, Blackstone EH, Grunkemeier GL, Takkenberg JJ, et al. Guidelines for reporting mortality and morbidity after cardiac valve interventions. J Thorac Cardiovasc Surg. 2008;135(4):732-738.
doi pubmed - Pang PY, Sin YK, Lim CH, Tan TE, Lim SL, Chao VT, Chua YL. Surgical management of infective endocarditis: an analysis of early and late outcomes. Eur J Cardiothorac Surg. 2015;47(5):826-832.
doi pubmed - Filsoufi F, Anyanwu AC, Salzberg SP, Frankel T, Cohn LH, Adams DH. Long-term outcomes of tricuspid valve replacement in the current era. Ann Thorac Surg. 2005;80(3):845-850.
doi pubmed - Chang BC, Lim SH, Yi G, Hong YS, Lee S, Yoo KJ, Kang MS, et al. Long-term clinical results of tricuspid valve replacement. Ann Thorac Surg. 2006;81(4):1317-1323, discussion 1323-1314.
doi pubmed - Garatti A, Nano G, Bruschi G, Canziani A, Colombo T, Frigiola A, Martinelli L, et al. Twenty-five year outcomes of tricuspid valve replacement comparing mechanical and biologic prostheses. Ann Thorac Surg. 2012;93(4):1146-1153.
doi pubmed - Civelek A, Ak K, Akgun S, Isbir SC, Arsan S. Tricuspid valve replacement: an analysis of risk factors and outcomes. Thorac Cardiovasc Surg. 2008;56(8):456-460.
doi pubmed - Do QB, Pellerin M, Carrier M, Cartier R, Hebert Y, Page P, Perrault LP, et al. [Isolated tricuspid valve replacement. Long-term results]. Arch Mal Coeur Vaiss. 2000;93(9):1119-1124.
- Koplan BA, Stevenson WG, Epstein LM, Aranki SF, Maisel WH. Development and validation of a simple risk score to predict the need for permanent pacing after cardiac valve surgery. J Am Coll Cardiol. 2003;41(5):795-801.
doi - Habib G. [Infective endocarditis: what's new? European Society of Cardiology (ESC) Guidelines 2009 on the prevention, diagnosis and treatment of infective endocarditis]. Presse Med. 2010;39(6):704-709.
doi pubmed - Nataloni M, Pergolini M, Rescigno G, Mocchegiani R. Prosthetic valve endocarditis. J Cardiovasc Med (Hagerstown). 2010;11(12):869-883.
doi pubmed - Alagna L, Park LP, Nicholson BP, Keiger AJ, Strahilevitz J, Morris A, Wray D, et al. Repeat endocarditis: analysis of risk factors based on the International Collaboration on Endocarditis - Prospective Cohort Study. Clin Microbiol Infect. 2014;20(6):566-575.
doi pubmed - Fedoruk LM, Jamieson WR, Ling H, Macnab JS, Germann E, Karim SS, Lichtenstein SV. Predictors of recurrence and reoperation for prosthetic valve endocarditis after valve replacement surgery for native valve endocarditis. J Thorac Cardiovasc Surg. 2009;137(2):326-333.
doi pubmed - Shetty N, Nagpal D, Koivu S, Mrkobrada M. Surgical and medical management of isolated tricuspid valve infective endocarditis in intravenous drug users. J Card Surg. 2016;31(2):83-88.
doi pubmed - Frontera JA, Gradon JD. Right-side endocarditis in injection drug users: review of proposed mechanisms of pathogenesis. Clin Infect Dis. 2000;30(2):374-379.
doi pubmed - Rodger L, Glockler-Lauf SD, Shojaei E, Sherazi A, Hallam B, Koivu S, Gupta K, et al. Clinical characteristics and factors associated with mortality in first-episode infective endocarditis among persons who inject drugs. JAMA Netw Open. 2018;1(7):e185220.
doi pubmed - Elbatarny M, Bahji A, Bisleri G, Hamilton A. Management of endocarditis among persons who inject drugs: A narrative review of surgical and psychiatric approaches and controversies. Gen Hosp Psychiatry. 2019;57:44-49.
doi pubmed - Rizzoli G, Vendramin I, Nesseris G, Bottio T, Guglielmi C, Schiavon L. Biological or mechanical prostheses in tricuspid position? A meta-analysis of intra-institutional results. Ann Thorac Surg. 2004;77(5):1607-1614.
doi pubmed - Campelo-Parada F, Lairez O, Carrie D. Percutaneous treatment of the tricuspid valve disease: new hope for the "Forgotten" valve. Rev Esp Cardiol (Engl Ed). 2017;70(10):856-866.
doi - Godart F, Baruteau AE, Petit J, Riou JY, Sassolas F, Lusson JR, Fraisse A, et al. Transcatheter tricuspid valve implantation: a multicentre French study. Arch Cardiovasc Dis. 2014;107(11):583-591.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.