

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 13, Number 2, April 2022, pages 118-121

Snaring Technique for Removal of Entrapped Coronary Guidewire in the Left Anterior Descending Artery
Ravi A. Thakkera, c, Rafic F. Berbarieb, Paul Kumfaa, Syed Gilania
aDivision of Cardiology, University of Texas Medical Branch, Galveston, TX, USA
bDivision of Cardiology, UT Southwestern Medical Center, Dallas, TX, USA
cCorresponding Author: Ravi A. Thakker, Division of Cardiology, University of Texas Medical Branch, Galveston, TX 77550, USA
Manuscript submitted March 8, 2022, accepted March 17, 2022, published online April 5, 2022
Short title: Snaring Technique for Guidewire Removal
doi: https://doi.org/10.14740/cr1369
| Abstract | ▴Top |
A 68-year-old female underwent coronary angiogram which was complicated by guidewire entrapment in a deployed left anterior descending (LAD) artery stent that extended into the aorta. Snare loop technique was utilized to retrieve the entrapped guidewire and LAD stent with successful deployment of a new stent. Snaring technique is a unique method for percutaneous extraction and can be utilized with whole stent removal along with the guidewire. This technique, as outlined in our case, can be a safe and effective approach.
Keywords: Coronary guidewire complications; Percutaneous coronary intervention complications; Entrapped coronary guidewire
| Introduction | ▴Top |
Coronary guidewires play a pivotal role in the management of invasive coronary artery therapy. Gruntzig in the 1970s and several other interventionalists would pave the way for the development of the flexible guidewires used today [1]. Guidewire retention is rare at a reported incidence of 0.2% or less. Although rare, serious complications such as coronary thrombus formation, air embolus, systemic embolization, coronary artery dissection, and cardiac tamponade can occur [2]. We present a case of a guidewire entrapment in the left anterior descending (LAD) artery with extension to the aorta with removal using the snare loop technique.
| Case Report | ▴Top |
A 68-year-old African American female presented to the cardiology clinic to establish care with progressively worsening dyspnea at rest over 2 months. She had associated paroxysmal nocturnal dyspnea, bilateral lower extremity swelling, and weight gain. She denied chest pain, palpitations, syncope. The patient’s past medical history was notable for coronary artery disease with recent triple vessel coronary artery bypass grafting, mild aortic stenosis, hypertension, hyperlipidemia, obesity, New York Heart Association (NYHA) class II heart failure with preserved ejection fraction (HFpEF), uncontrolled type two diabetes mellitus, prior ischemic stroke, peripheral artery disease with stenting of the right femoral artery, stage 3 chronic kidney disease, chronic obstructive pulmonary disease, and tobacco use of greater than 30 pack years.
Initial workup included an electrocardiogram with no ST segment changes. Troponin was negative. Her N-terminal-pro hormone BNP (NT-proBNP) was elevated at 1,780 pg/mL (normal range: < 125 pg/mL). Transthoracic echocardiography was notable for diastolic dysfunction, dilated left atrium, and elevated right systolic pressure. She further underwent myocardial perfusion imaging which demonstrated reversible defects in the anterior and infero-apical left ventricular myocardium. A left heart catheterization using right radial access was performed to evaluate the left ventricular defects. Diagnostic angiography demonstrated mid LAD disease. Extra-backup catheter (EBU) 3.0 was used to engage the LAD. Fractional flow reserve (FFR) of the mid LAD was positive. The guidewire was then placed in the LAD and another placed in the first diagonal branch (D1). Intravascular ultrasound (IVUS) was indicative of diffuse disease from ostial LAD to mid LAD. Another wire was placed in the left circumflex (LCX) artery. A 2.5-mm balloon was deployed, and a 2.75 × 38 mm drug-eluting stent (DES) was placed in the mid LAD and a 3.5 × 24 mm DES was placed in the proximal LAD. The mid LAD stent was then post-dilated. IVUS indicated well expanded and well apposed stents. LAD and LCX wires were then pulled successfully. The D1 wire had significant resistance while pulling back behind proximal LAD and then got stuck behind the proximal LAD stent struts. Apex Over-The-Wire (Boston Scientific) balloon was used to retrieve the wire but with no success. Fine-cross was then utilized with some success but the distal radiopaque portion of the wire got stuck and broke and remained behind the proximal LAD stent struts with a portion of the wire extending into the ascending aorta. At this time, the options were to do percutaneous attempt to remove the broken portion of the wire from the ascending aorta or surgical removal. It was decided to pursue the percutaneous approach to retrieve the guidewire extending from the ascending aorta to the LAD artery. Detailed review of angiogram demonstrated the broken portion of the guidewire extending from the left main (LM) artery and ascending aorta to the aortic arch and was mobile and coiled. EBU 3.0 guidewire was advanced to the aortic arch and Ensnare (Merit Medical) 4 - 8 mm was deployed to attempt capture but was unsuccessful due to significant mobility in the wire. Therefore, a larger Ensnare (Merit Medical) 12 - 20 mm and 8 French Amplatzer left (AL1) guide to the aortic arch was deployed and the wire was captured from the ascending aorta. The AL1 guide was then advanced over the wire towards the LM while pulling on the captured wire but the thin portion of the wire broke loose again and a portion of the mobile wire retrieved, with residual portion behind the LAD stent and extending out of the LM into the aortic root. This was followed by EBU 3.0 guide which was advanced to LM followed by Ensnare (Merit Medical) 4 - 8 mm which was deployed to capture the wire outside the LM and was removed with moderate amount of resistance. Once we reviewed the retrieved material it was noted that the broken wire was entrapped within the proximal LAD stent that was elongated and partly extending into the LM and aortic root. Therefore, the broken wire and proximal LAD stent were captured by the snare and retrieved in one piece (Fig. 1). The final angiogram showed patent residual focal nonflow limiting dissection in the proximal LAD. A 3 × 24 mm DES was placed to the proximal LAD and was well expanded when confirmed on IVUS. LM remained patent with no dissection or injury. Gross examination of the retrieved stent and guidewire showed separation and unwinding of the distal tip of the BMW wire (Fig. 2).
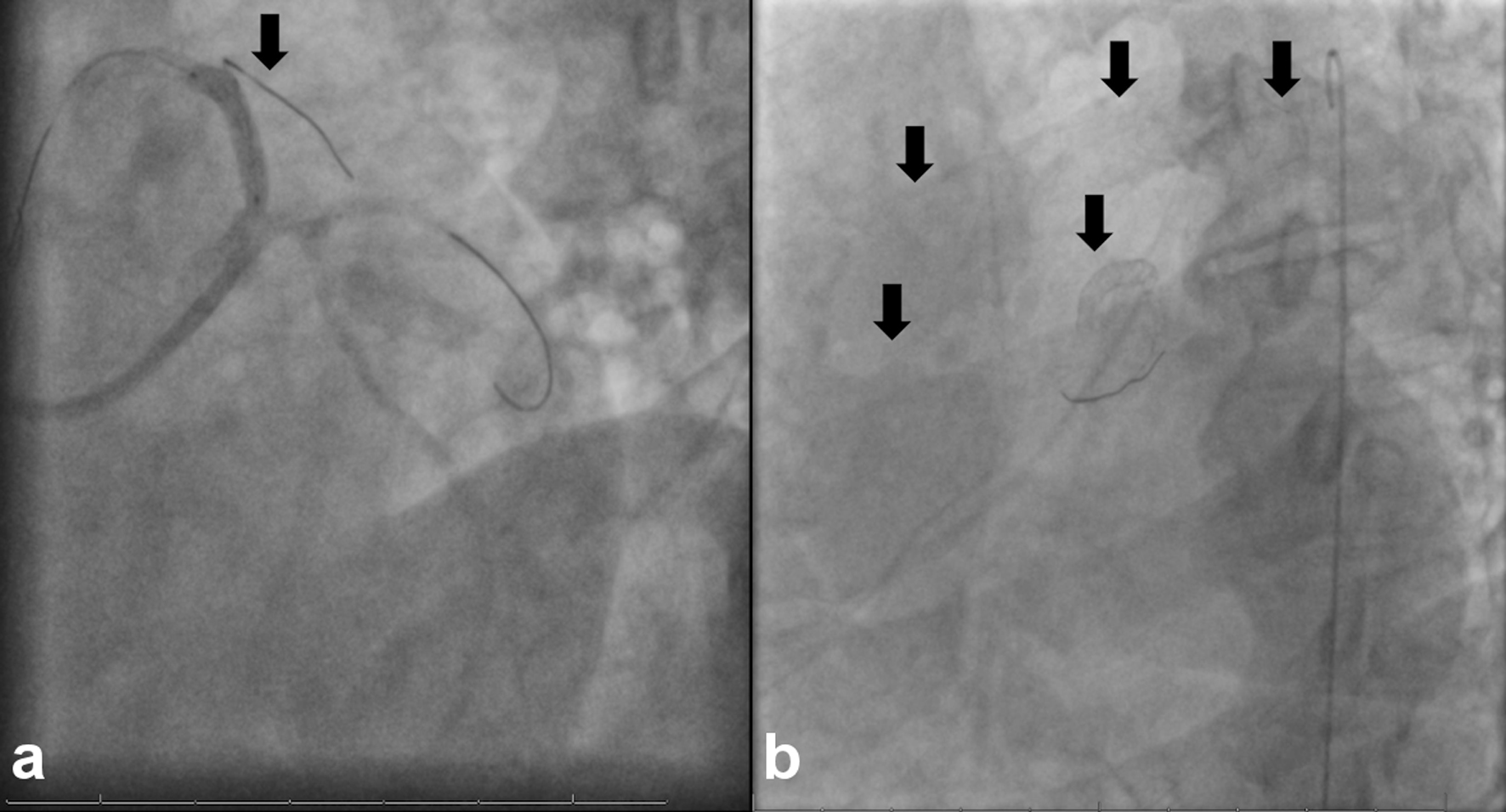 Click for large image | Figure 1. (a) Left anterior (LA) caudal view on the left with view of guidewire in LCX, LAD, and D1 (arrow). (b) Mobile guidewire with detached distal portion entrapped in drug-eluting stent (arrows). LCX: left circumflex artery; LAD: left anterior descending; D1: first diagonal branch. |
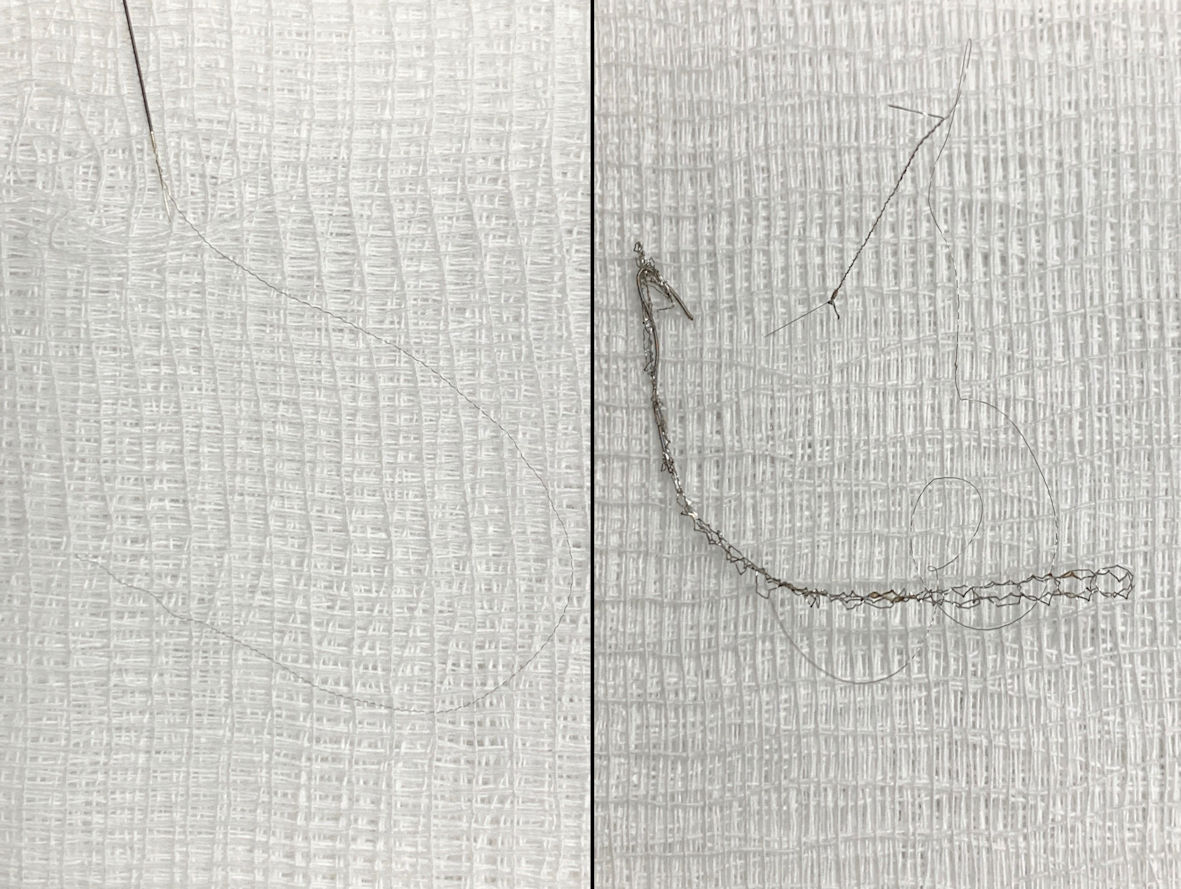 Click for large image | Figure 2. Gross specimen of retrieved stent and guidewire showing separation and unwinding of the distal tip of the BMW wire. |
| Discussion | ▴Top |
The structure of the guidewire is composed of the inner aspect known as the core which has a proximal portion made of alloy and the distal portion is made of either nitinol or steel and is usually flexible. The body of the guidewire is composed of either coils or plastic polymers. Coils play an important role in the dexterity of the wire. The outer coating of the guidewire is composed of a either a hydrophilic coat thereby decreasing surface tension or a hydrophobic coat which reduces the agility of the wire but allows for more tactility [3]. The BMW guidewire, which was found to be entrapped in the struts of our patient’s stent, is known for its torquability. It consists of both a distal core and a stainless proximal shaft [4]. The concern for guidewire unraveling and entrapment is appreciated to occur at a higher instance when rotation beyond 180 degrees occurs. Management is focused through either percutaneous retrieval which was our approach, surgical removal, and no intervention at all. An alternative if pursuing the percutaneous route, as noted by Danek et al, is to limit excessive force when removing entrapped guidewires and to assist removal with use of a balloon catheter or microcatheter over the entrapped wire to center the application of force. They also suggest the use of a snare loop when fracturing is involved, which is the method we utilized [5]. Recently Megaly et al also demonstrated a case of entrapment of the Runthrough wire in the diagonal branch after LAD stenting. Attempts by the team were made to extract the wire but a segment ended up being left behind in the ascending aorta. They utilized wire entrapment and removal en bloc, as well as Gooseneck microsnares (Medtronic) but these failed. Ultimately, Ensnare (Merit Medical) 27 × 48 mm was deployed with successful extraction of the wire in the aorta [6].
Post-procedure our patient did well and had preservation of her hemodynamic status. She was discharged 3 days later on dual antiplatelet therapy and a high-dose statin. She was followed up in clinic 1 month later with absence of chest pain and had improvement in dyspnea.
Although guidewires play a common role in everyday invasive cardiovascular therapy, operators should always be cautious during deployment and retraction even in the most straightforward of procedures. Our case highlights one technique of broken guidewire removal using snare retrieval with positive outcomes.
Learning points
Entrapped coronary guidewires are a rare complication. Outcomes can be devastating from dissection, thrombus formation, to tamponade. The three main management approaches are percutaneous removal, surgery, and conservative observation. Snaring technique is a unique method for percutaneous extraction and can be utilized with whole stent removal along with the guidewire. This technique, as outlined in our case, can be a safe and effective approach.
Acknowledgments
The information in this case was presented at a prior TCT conference.
Financial Disclosure
The authors report no pertinent financial disclosure or funding relevant to this manuscript.
Conflict of Interest
The authors declare that there is no conflict of interest.
Informed Consent
Informed consent was obtained from patient’s next of kin.
Author Contributions
RAT, RFB, PK, and SG contributed to study design, drafting of the manuscript, editing of the manuscript, and final approval of the manuscript.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
NYHA: New York Heart Association; HFpEF: heart failure with preserved ejection fraction; NT-proBNP: N-terminal-pro hormone; LAD: left anterior descending; EBU: extra-backup catheter; FFR: fractional flow reserve; D1: first diagonal branch; IVUS: intravascular ultrasound; LCX: left circumflex artery; DES: drug-eluting stent; LM: left main artery; AL1: Amplatzer left
| References | ▴Top |
- Kaltenbach M. 40 years of percutaneous coronary intervention: a historical remark on the development and evolution of guidewire technology. JACC Cardiovasc Interv. 2017;10(24):2582-2583.
doi pubmed - Al-Moghairi AM, Al-Amri HS. Management of retained intervention guide-wire: a literature review. Curr Cardiol Rev. 2013;9(3):260-266.
doi pubmed - Toth GG, Yamane M, Heyndrickx GR. How to select a guidewire: technical features and key characteristics. Heart. 2015;101(8):645-652.
doi pubmed - Hong YM, Lee SR. A case of guide wire fracture with remnant filaments in the left anterior descending coronary artery and aorta. Korean Circ J. 2010;40(9):475-477.
doi pubmed - Danek BA, Karatasakis A, Brilakis ES. Consequences and treatment of guidewire entrapment and fracture during percutaneous coronary intervention. Cardiovasc Revasc Med. 2016;17(2):129-133.
doi pubmed - Megaly M, Basir MB, Brilakis E, Alaswad K. Wire entrapment and unraveling in the aorta: snaring technique for the nonvisible filament. JACC Cardiovasc Interv. 2022;15(2):e21-e22.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.