

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 13, Number 4, August 2022, pages 206-217

Factors Influencing Thirty-Day Readmission Rate in Patients With Heart Failure Exacerbation
Mrhaf Alsammana, b, c ![]() , Dewid Zayas Zuazagaa, b, Karthikram Komanduria, b, Rakesh Prashada, b, Cristobal Cintrona, b, Kim N. Page Vickeryb
, Dewid Zayas Zuazagaa, b, Karthikram Komanduria, b, Rakesh Prashada, b, Cristobal Cintrona, b, Kim N. Page Vickeryb
aDepartment of Internal Medicine, Graduate Medical Education, University of Central Florida College of Medicine, Orlando, FL, USA
bDepartment of Internal Medicine, Internal Medicine Residency Program, HCA Florida Ocala Hospital, Ocala, FL, USA
cCorresponding Author: Mrhaf Alsamman, Department of Internal Medicine, Graduate Medical Education, University of Central Florida College of Medicine, Orlando, FL, USA
Manuscript submitted April 27, 2022, accepted June 17, 2022, published online August 15, 2022
Short title: Factors of 30-Day Readmission in HF Patients
doi: https://doi.org/10.14740/cr1390
| Abstract | ▴Top |
Background: The purpose of this study is to further investigate the leading causes of readmission at 30 days in heart failure exacerbation patients, along with associations to mortality and intensive care unit (ICU) admissions.
Methods: A retrospective data analysis was performed on a total of 33,400 patients between January 1, 2016, and December 31, 2020. The primary endpoints were to determine whether guideline-directed medical therapy (GDMT), length of stay, and time to first diuretic affect readmission rates. Secondary endpoints include time to first chest X-ray, time to first echocardiogram, administration of intravenous fluids, diet, presence of cardiology consult, and ICU admission.
Results: Patients who received GDMT had decreased likelihood of mortality (odds ratio (OR): 0.518; 95% confidence interval (CI): 0.394 - 0.682; P < 0.001). Patients who had an echocardiogram done within 1 day of admission had less likelihood of death (OR: 0.606; 95% CI: 0.483 - 0.759; P < 0.001). In addition, patients who had a cardiac diet during their hospitalization were 0.632 times less likely to experience mortality (95% CI: 0.502 - 0.797; P < 0.001). Patients that received their first intravenous diuretic 2 h or more after admission were 1.290 times as likely to be readmitted within 30 days (95% CI: 1.018 - 1.634; P = 0.035). In addition, patients that did not receive intravenous diuretics were even more likely to be readmitted within 30 days (OR: 1.555; 95% CI: 1.237 - 1.955; P < 0.01). Patients who were treated with GDMT had a decreased chance of being readmitted within 30 days (OR: 0.781; 95% CI: 0.647 - 0.944; P = 0.01).
Conclusions: This study stresses the importance of initiating GDMT, cardiac diet, diuretics, and echocardiogram in timely manner.
Keywords: Heart failure; Angiotensin-converting enzyme inhibitor; Echocardiogram; Guideline-directed medical therapy; Beta-blocker
| Introduction | ▴Top |
With a prevalence of over 5.8 million in the United States and over 23 million worldwide, heart failure (HF) is one of the primary causes of hospitalization and readmissions. According to Medicare, 30-day readmissions of HF patients increased by 23% between 2009 and 2012 [1, 2]. HF accounts for approximately $31 billion in healthcare costs in the United States [3]. For these patients, as per the American College of Cardiology, the hallmark for treatment is guideline-directed medical therapy (GDMT). GDMT comprises of at least one medication from each of two categories: an angiotensin-converting enzyme inhibitor (ACEI), angiotensin receptor blocker (ARB), or angiotensin receptor-neprilysin inhibitor (ARNI) in addition to a beta-blocker (BB). In addition, a diuretic may be added as needed for the patient’s symptom and class. Despite significant evidence of GDMT, a majority of HF patients do not receive the complete therapy [4]. This poor implementation has been attributed to a number of factors such as the lack of understanding of treatment goals, a hesitancy to use newly recommended drugs, a focus on symptom relief rather than mortality reduction, or a fear of adverse effects. In addition, some non-medical issues also play a role, such as drug costs, access to health-care systems, and lack of follow-up [5]. The purpose of this study is to further investigate the leading causes of readmission at 30 days in HF exacerbation patients, along with causes for mortality and intensive care unit (ICU) admissions for HF patients.
| Materials and Methods | ▴Top |
Study design
The Hospital Corporation of America (HCA Healthcare) database was used for this study to obtain information regarding patients admitted and discharged from two community hospitals in Florida. A retrospective data analysis was performed on these patients with a diagnosis of HF exacerbation admitted and discharged between January 1, 2016, and December 31, 2020.
Study population
There were a total of 33,400 patients aged 18 to 90+ (90+ coded as 90 due to Safe Harbor Guidelines) admitted and discharged between January 1, 2016 and December 31, 2020 with criteria for acute HF exacerbation with International Classification of Disease 10th Revision (ICD-10) codes: I50.21, I50.23, I50.31, I50.33, I50.41, I50.43, I50.811, I50.813, I11.0, I13.0. Demographic and clinical data extracted included age, gender, race, insurance status, length of stay, the presence of non-cardiac comorbidities, labs such as sodium, brain natriuretic peptide (BNP), creatinine, and albumin, dietary status in the inpatient setting, the time taken for administering the first diuretic, the time taken for the first echocardiogram, ICU admission and length of stay, basic vitals, and readmission. Readmission time for HF exacerbation was limited at 30 days. Excluded patients include coronavirus disease 2019 (COVID-19) positive, unstable angina, acute myocardial infarction, ST elevation myocardial infarction (STEMI), non-ST elevation myocardial infraction (NSTEMI), cardiac tamponade, endocarditis, pneumonia, chronic kidney disease (CKD) stage V, end-stage renal disease (ESRD), septic shock, hemorrhagic shock and hypovolemic shock (Supplementary Material 1, www.cardiologyres.org). Out of 33,400 patients, 6,222 patients were included in the final analysis (Fig. 1).
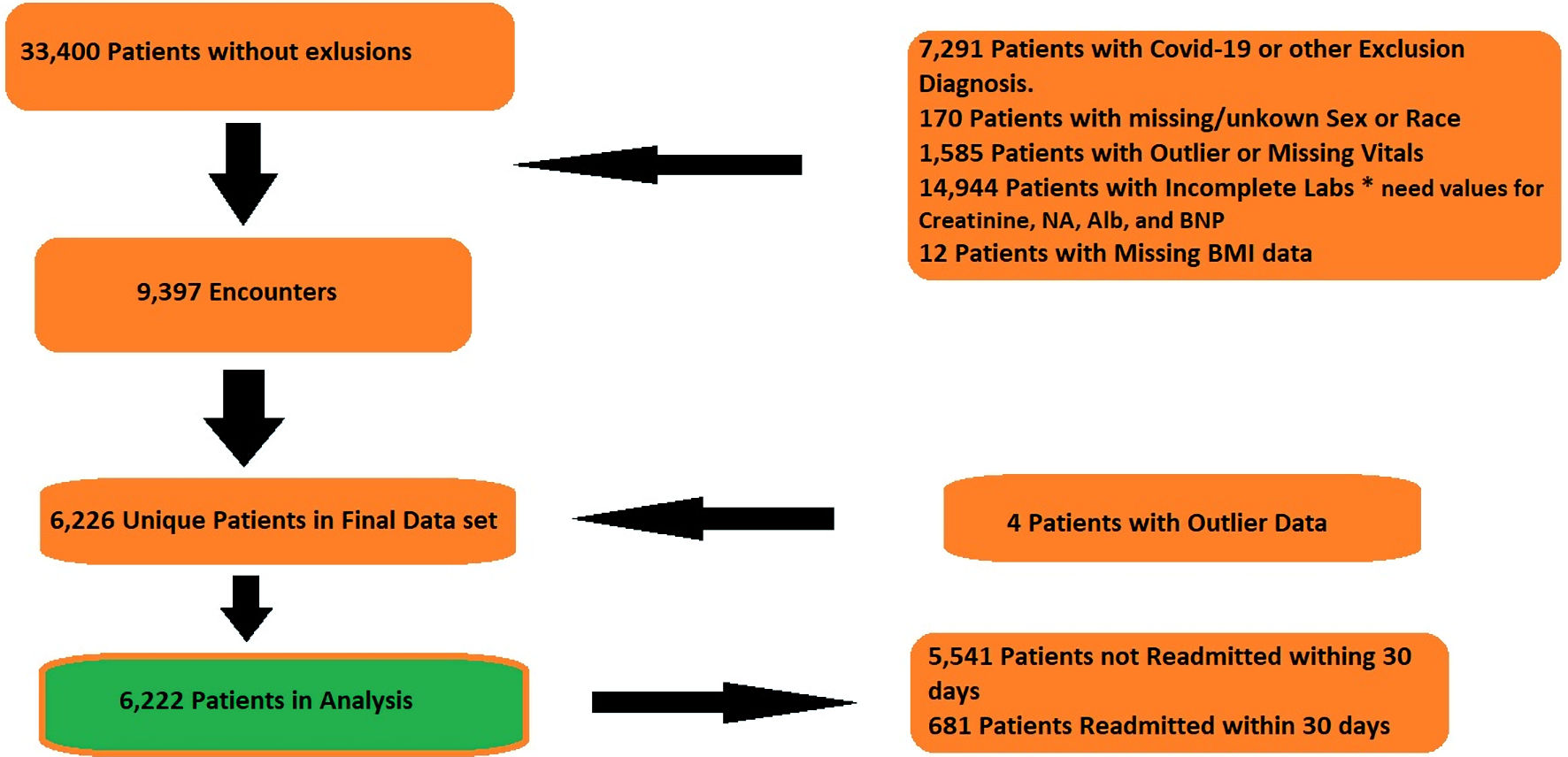 Click for large image | Figure 1. Flowchart of data exclusions. COVID-19: coronavirus disease 2019; BNP: brain natriuretic peptide; Alb: albumin; BMI: body mass index. |
Study objectives
The objective of this study is to identify and stratify the causes of readmission for HF exacerbation at 30 days. The primary endpoints of this study are to determine whether GDMT, length of stay, and time to first diuretic affect readmission rates. Secondary endpoints include time to first chest X-ray, time to first echocardiogram, administration of intravenous fluids or lack of fluid restriction, proper dietary restriction (i.e., cardiac or sodium restricted diet), presence of cardiology consult, and ICU admission.
Statistical analysis
Statistical analysis included univariate analysis with logistic regression, binary logistic regression, and linear regression using SPSS software. The models included readmission, mortality and hospice, ICU admission and ICU length of stay. To determine strength of association, odds ratio (OR) and 95% confidence intervals (CI) were calculated for logistic regression.
Institutional review board approval
This research activity was determined to be exempt or excluded from Institutional Review Board (IRB) oversight in accordance with current regulations and institutional policy. This study was conducted in compliance with the ethical standards of the responsible institution on human subjects.
| Results | ▴Top |
Patient population
Out of 33,400 patients, 6,222 were included in the final analysis. Out of this population, 82% were white and 12.8% were black. Only 38.3% of the patients were on an ACEI/ARB, whereas 67.5% were on a BB. With this in perspective, only 30.7% of the patient were on all components of GDMT for HF; 7.3% of the patients died in addition to 5.8% discharged to hospice; 42.4% of patient never received a diuretic, despite being admitted for acute exacerbation of HF; and only 28.6% received the diuretic within 2 h of arrival to the hospital (Table 1).
 Click to view | Table 1. Frequency Table for Entire Population |
Readmission patient population
Out of the included 6,222 patients, 681 (10.9%) patients were readmitted within 30 days. Out of these 681 patients, 304 (44.6%) were female, 572 (84%) were white, and 19 (2.8%) were uninsured. Almost half (330, 48.5%) never received a diuretic, and only 21.6% of the readmitted patients received a diuretic within 2 h (loop diuretic or potassium sparing diuretics or both), whereas 12.3% received intravenous fluids. Only 243 patients (35.7%) were prescribed ACEI/ARBs, and only 27.9% of patients were on all requirements for GDMT. The majority of readmitted patients (87.4%) had a cardiac consult during their stay. Three hundred twenty-one (47.1%) and 371 (54.5%) of patients had an abnormal albumin and BNP, respectively (Table 2).
Click to view | Table 2. Readmission vs. No Readmission Frequency Table |
Logistic regression for readmission
We investigated factors that could impact the likelihood of a patient with acute HF being readmitted within 30 days in this model (Table 3). Population size was 5,765 patients (excluding patients that expired). Regarding length of stay, the model showed that for each 1-day increase in length of stay, patients are 1.026 times more likely to be readmitted within 30 days (95% CI: 1.006 - 1.047; P = 0.013). Patients that received their first intravenous diuretic 2 h or more after admission were 1.290 times as likely to be readmitted within 30 days, compared to patients that had their first administration of an intravenous diuretic within 2 h of admission (95% CI: 1.018 - 1.634; P = 0.035). In addition, patients that did not receive intravenous diuretics were even more likely to be readmitted within 30 days, when compared to patients that had their first administration of an intravenous diuretic within 2 h of admission (OR: 1.555; 95% CI: 1.237 - 1.955; P < 0.01). Patients who were treated with GDMT had a decreased chance of being readmitted within 30 days compared to patients who did not receive therapy (OR: 0.781; 95% CI: 0.647 - 0.944; P = 0.01). Patients who were either admitted directly to the ICU or were in the ICU during their hospitalization were more likely to have a readmission within 30 days compared to patients who remained on the floors (OR: 1.665; 95% CI: 1.274 - 2.178; P < 0.001). In addition, patients who received an echocardiogram within 1 day of admission were less likely to have a readmission (OR: 0.836; 95% CI: 0.700 - 0.998; P = 0.047) (Table 3, Fig. 2).
Click to view | Table 3. Logistic Regression for Likelihood of Readmission in 30 Days |
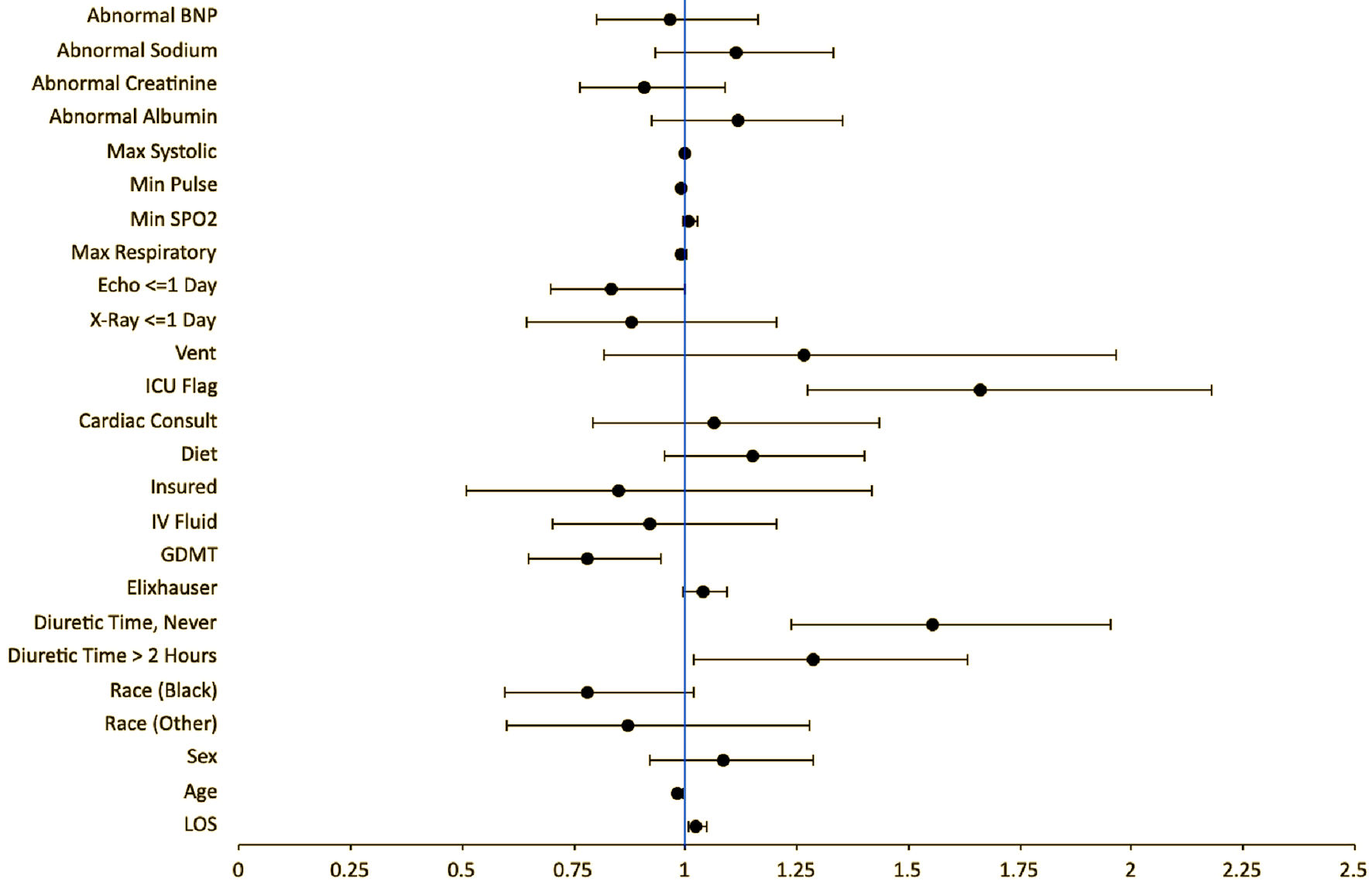 Click for large image | Figure 2. Forest plot for logistic regression for likelihood of readmission in 30 days. ICU: intensive care unit; GDMT: guideline-directed medical therapy; IV: intravenous; BNP: brain natriuretic peptide; SpO2: oxygen saturation; LOS: length of stay. |
Logistic regression for mortality
We investigated factors associated with an increased likelihood of a HF exacerbation patient expiring. Due to insufficient quantities of patients, mortality and hospice are in the same category for this analysis of 6,222 patients. Patients who received GDMT had decreased likelihood of mortality (OR: 0.518; 95% CI: 0.394 - 0.682; P < 0.001). Patients who had an echocardiogram done within 1 day of admission had less likelihood of death or discharge to hospice compared to patients who did not receive an echocardiogram within 1 day (OR: 0.606; 95% CI: 0.483 - 0.759; P < 0.001). Length of stay for patients had an inverse relationship to mortality. For every 1 day increase in length of stay, the patient had a decreased risk of mortality (OR: 0.917; 95% CI: 0.892 - 0.942; P < 0.001). In addition, patients who had a cardiac diet during their hospitalization were 0.632 times less likely to experience mortality (95% CI: 0.502 - 0.797; P < 0.001). Abnormal lab values were all associated with an increased likelihood of mortality when all other variables are held constant. This included abnormal albumin, creatinine, sodium, and BNP with their hazard ratios 1.651, 1.688, 1.473, and 2.268, respectively. These findings were statistically significant with P < 0.001. Patients who had a cardiology consult had a higher likelihood of mortality (OR: 1.828; 95% CI: 1.131 - 2.953; P = 0.014) whereas patient who never received diuretics had a decreased likelihood (OR: 0.68; 95% CI: 0.504 - 0.918; P = 0.012) (Table 4, Fig. 3).
Click to view | Table 4. Logistic Regression for Likelihood of Mortality |
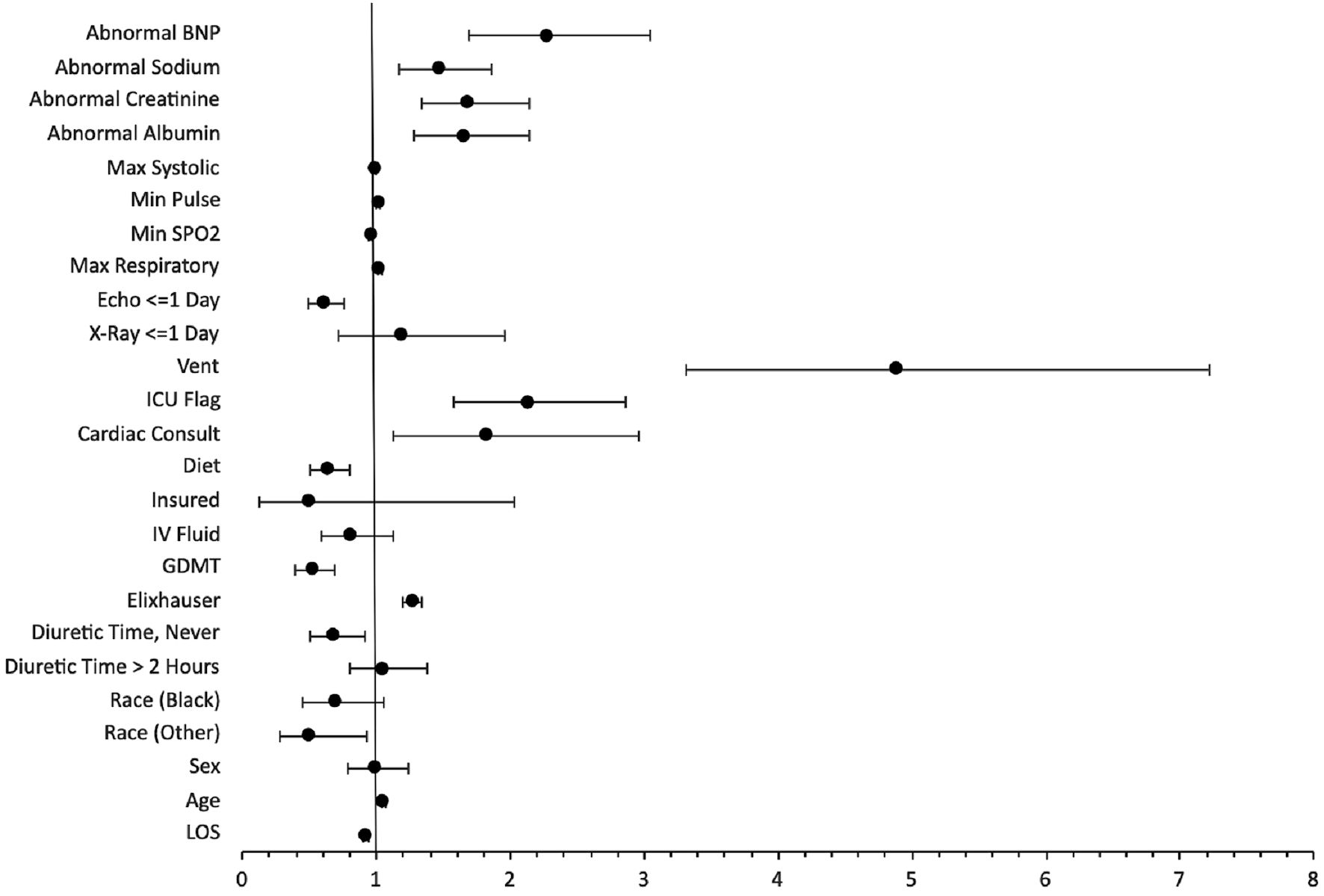 Click for large image | Figure 3. Forest plot for logistic regression of likelihood of mortality. ICU: intensive care unit; GDMT: guideline-directed medical therapy; IV: intravenous; BNP: brain natriuretic peptide; SpO2: oxygen saturation; LOS: length of stay. |
Logistic regression for ICU admission
Using our initial population of 6,222 patients, we investigated if readmitted patients were more likely to have been in the ICU during their initial admission. Patient’s ventilator status and length of stay were removed from this analysis due to collinearity; this was because patients placed on a ventilator and patients with a longer length of stay were much more likely to be admitted to the ICU. The timing of diuretics also affected likelihood of admission to ICU. Patient that received intravenous diuretics 2 h after admission, when compared to patients who received them within 2 h, were more likely to be admitted to the ICU (OR: 1.703; 95% CI: 1.378 - 2.103; P < 0.001). The administration of fluids (OR: 2.306; 95% CI: 1.860 - 2.860; P < 0.001), obtaining an echocardiogram within 1 day (OR: 1.865; 95% CI: 1.562 - 2.227; P < 0.001), and cardiology consults (OR: 1.702; 95% CI: 1.152 - 2.515; P = 0.008) also seemed to increase the chances of ICU admission. In addition, abnormal albumin, sodium, and BNP were 2.964, 1.577, and 1.416 times more likely to be admitted to the ICU respectively (P < 0.0001 for all). Patients on a cardiac diet seemed to be less likely to be in the ICU (OR: 0.726; 95% CI: 0.607 - 0.869; P < 0.001). There was no statistically significant relationship between patients on GDMT and likelihood of ICU admission (Table 5, Fig. 4).
Click to view | Table 5. Logistic Regression for Likelihood of ICU Admission in Their Initial Presentation |
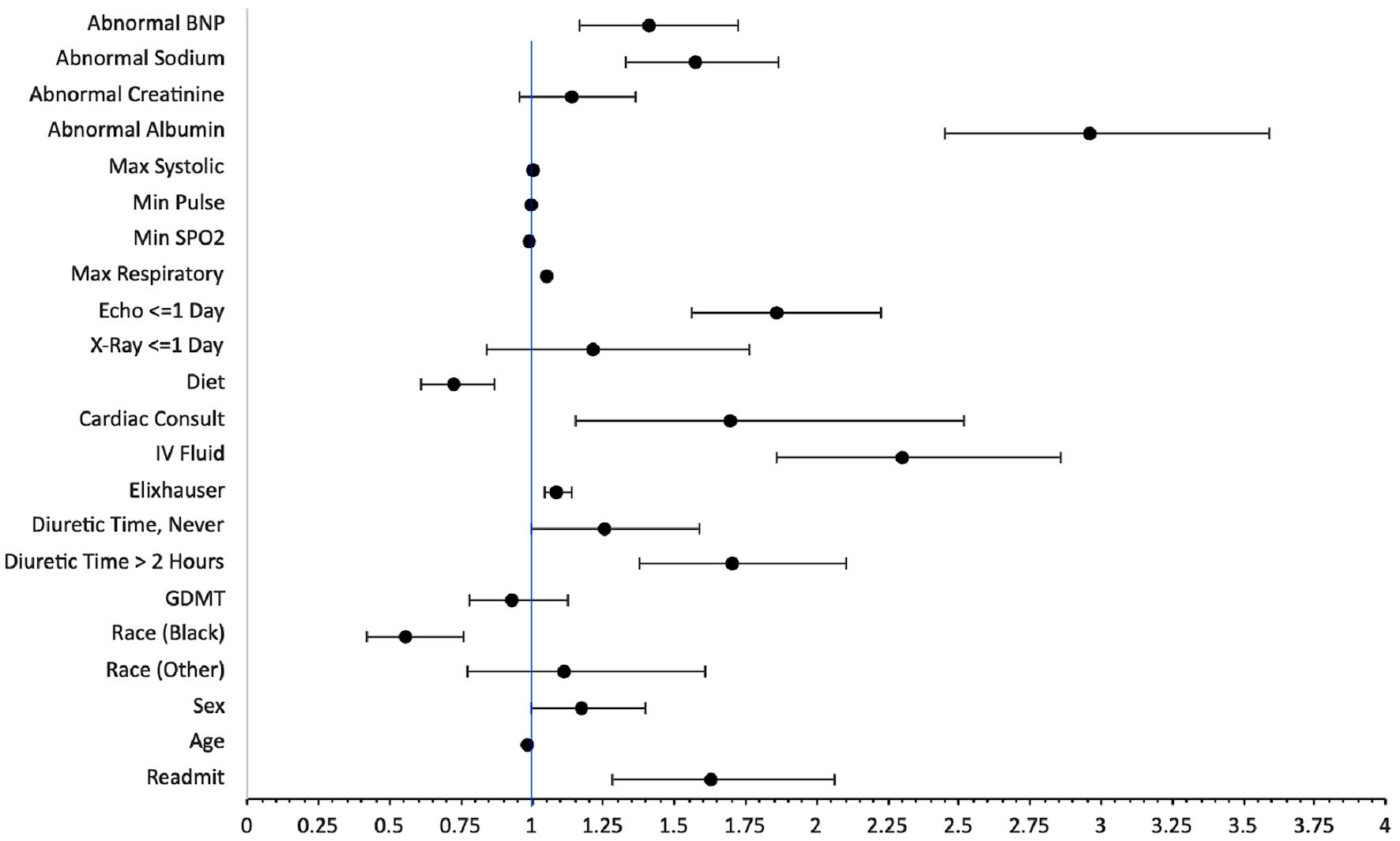 Click for large image | Figure 4. Forest plot for logistic regression for likelihood of ICU admission. GDMT: guideline-directed medical therapy; IV: intravenous; BNP: brain natriuretic peptide; SpO2: oxygen saturation; LOS: length of stay. |
Linear regression for ICU length of stay
We used a population size of 874 patients who had ICU admissions in their initial hospitalization. We investigated if readmitted patients that were in the ICU have a longer length of stay than non-readmitted patients and a linear regression was used to predict the numerical variable. Readmission was not statistically significant in predicting length of stay for ICU, i.e., patients that were readmitted had no statistical difference in length of stay in the ICU compared to non-readmitted patients. Male patients had a 0.554-day longer ICU length of stay when compared to female patients. Patients that received intravenous diuretics more than 2 h after admission had an average increase of length of stay of 1.047 days (95% CI: 0.365 - 1.729; P = 0.003). Abnormal albumin levels (B: 1.121; 95% CI: 0.467 - 1.774; P < 0.001), abnormal creatinine levels (B: 0.646; 95% CI: 0.084 - 1.209; P = 0.024), and abnormal sodium levels (B: 1.098; 95% CI: 0.546 - 1.650; P < 0.001) were associated with increase in length of stay in the ICU (Table 6).
Click to view | Table 6. Linear Regression for ICU Length of Stay |
| Discussion | ▴Top |
HF prevalence continues to grow at an exponential rate. Despite constantly updated guidelines, HF tends to be one of the primary causes of hospitalizations and readmissions in the United States, creating a huge burden for the Unites States healthcare system [6]. In this study, we aimed to stratify and identify potential causes for readmissions in two community hospitals in Central Florida. In addition, we were able to identify the difference in characteristics of patient management for mortality, ICU admission and ICU length of stay.
Patients on GDMT had a decreased likelihood of readmission (OR: 0.781) and decreased likelihood of mortality (OR: 0.518), further enhancing the importance of GDMT. Therapy was not significant for ICU admission. In our patient population, only 30.70% received all components of GDMT, with a majority receiving BBs but only 38.3% of the population receiving ACEI/ARBs. We know that patients with a HF exacerbation may have abnormal kidney function, which could mean that the ACEI/ARB was not started, however our data include medications that were prescribed at discharge, meaning these patients were not discharged on GDMT either. There is potential here for further improvement, including, but not limited to, patient and physician education.
An increase in length of stay (OR: 1.026), receiving first intravenous diuretic two or more hours after admission (OR: 1.290) or never receiving a diuretic (OR: 1.555), ICU admission (OR: 1.665) all seemed to increase likelihood of readmission in 30 days, in a logistic regression model. This would mean that an increase in 1 day of length of stay would mean that the patient is 1.026 times more likely to be readmitted. It would be important to note that patients who had an increase in length of stay also had increased chance of being admitted to the ICU. We can assume that these patients may have been sicker than the remaining population requiring and increased length of stay and possible ICU admission, which led to a decrease in mortality (OR: 0.518) but an increased risk of readmission, because of their level of sickness. Delay in intravenous diuretic administration also led to an increase likelihood of ICU admission (OR: 1.703) with a longer length of stay in the unit (B: 1.047). Despite increasing chances of readmission in 30 days, patients who did not receive diuretics had a decreased risk of mortality (OR: 0.68). Despite no statistical significance, patients that never received diuretics also were more likely to be admitted to the ICU (OR: 1.259, P = 0.053) which may have practical significance. We cannot assume any causation regarding these results, however, given the results we can speculate that the patients who had an increased length of stay were sicker, which increased chances of ICU admission, leading to a decrease in mortality, but however an overall increased risk of readmission. In contrast, patients who never received diuretics may have been healthier than most of the other population, thus the lower mortality.
Surprisingly, patients who had a cardiac consult during their admission had increased likelihood of ICU admission as well as an increase in mortality. Similar to length of stay, we can assume that patients who were sicker likely had cardiology on their care team in the hospital, which could have skewed the results. There was no statistical significance between readmission and cardiac consult. Patients who had an echocardiogram done within 1 day had a decreased chance of readmission in 30 days, decreased chance of mortality, and increased risk of admission to the ICU. We can speculate that patient who had the imaging done may have been diagnosed and managed more appropriately leading to decreased chance of readmission and mortality. In addition, these patients may have presented in a more serious condition, expediting the echocardiogram, but eventually requiring ICU admission, which could explain the association with increased risk of ICU admission. Cardiac diet also played a role in the decreased likelihood of mortality and ICU admission. Administration of intravenous fluids led to an increased risk of admission to the ICU (OR: 2.306). These findings suggest that there may be minor changes in our management that could affect overall readmission rates, such as making sure these patients do not receive fluids. Despite no statistical significance directly between fluids and readmission, fluids led to an increased risk of ICU admission, which had an increased risk of readmission.
Conclusions
Our study does not prove causation; it proves only association. The results from this study can lead to further subgroup analysis and further similar studies with a larger patient population to confirm. More importantly, given this data, we can say that there are many factors that play a role in risk of readmission, ICU admission, and mortality in HF exacerbation patients. The goal would be to improve basic management situations, including recognizing the signs of HF and avoiding fluids, promptly ordering an echocardiogram while the patient is still in the emergency department, ordering a cardiac diet, ordering diuretics promptly and initiating GDMT. This may be achieved with simply patient and physician education as well as electronic medical record checkpoints prompting the physician to treat per guidelines. We hope to implement many quality improvement projects in the future and obtain data to see if we can help decrease the healthcare costs via decreasing readmission rates for HF.
| Supplementary Material | ▴Top |
Suppl 1. Inclusion and exclusion criteria codes.
Acknowledgments
None to declare.
Financial Disclosure
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Informed Consent
This is a retrospective study. Informed consents were not obtained. However, IRB clearance was provided for this project.
Author Contributions
Mrhaf Alsamman: Abstract, Introduction, Materials and Methods. Dewid Zayas: Findings and Conclusions. Karthikram Komanduri: Discussion. Rakesh Prashad: final editing and review. Cristobal Cintron: statistical analysis. Kim N. Page Vicker: statistical analysis. All authors were involved in writing, reviewing, and revising the article prior to submission.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Roger VL. Epidemiology of heart failure. Circ Res. 2013;113(6):646-659.
doi pubmed - Ziaeian B, Fonarow GC. The prevention of hospital readmissions in heart failure. Prog Cardiovasc Dis. 2016;58(4):379-385.
doi pubmed - Singh L, Carly D. Mixed method study focusing on cost effectiveness of utilizing guideline directed medical therapy using secondary and primary data. View of mixed method study focusing on cost effectiveness of utilizing guideline directed medical therapy using secondary and primary data. https://journals.iupui.edu/index.php/IMPRS/article/view/24768/23435.
- McCullough PA, Mehta HS, Barker CM, Houten JV, Mollenkopf S, Gunnarsson C, Ryan M, et al. Healthcare utilization and guideline-directed medical therapy in heart failure patients with reduced ejection fraction. J Comp Eff Res. 2021;10(14):1055-1063.
doi pubmed - Komajda M, Anker SD, Cowie MR, Filippatos GS, Mengelle B, Ponikowski P, Tavazzi L, et al. Physicians' adherence to guideline-recommended medications in heart failure with reduced ejection fraction: data from the QUALIFY global survey. Eur J Heart Fail. 2016;18(5):514-522.
doi pubmed - Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139-e596.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.