

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 13, Number 4, August 2022, pages 246-249

A Curious Case of an Anomalous Right Coronary Artery
Michael Cinellia, Hamfreth Rahmingb, Marc Assaadb, d, Chetan Singhb, Hussam Aridib, Boutros Karamc, Ruben Kandova
aDepartment of Cardiology, Northwell Health, Staten Island University Hospital, SI, NY 10305, USA
bDepartment of Medicine, Northwell Health Staten Island University Hospital, SI, NY 10305, USA
cDepartment of Interventional Cardiology, NYU Langone Hospital, NY 10016, USA
dCorresponding Author: Marc Assaad, Department of Medicine, Northwell Health Staten Island University Hospital, SI, NY 10305, USA
Manuscript submitted June 29, 2022, accepted July 7, 2022, published online August 15, 2022
Short title: A Curious Case of an Anomalous RCA
doi: https://doi.org/10.14740/cr1406
| Abstract | ▴Top |
Single coronary artery (SCA) is an unusual congenital anomaly, seen by diagnostic coronary angiography. Absence of the right coronary artery (RCA) is one of the rarest coronary artery anomalies occurring when the artery fails to develop in the right atrioventricular (AV) groove. Herein, we describe the case of a 58-year-old man presenting with new onset decompensated congestive heart failure found to have a congenitally absent right coronary ostium. The AV groove extended such that the left circumflex artery supplied the domain of the RCA. Such coronary artery anomalies are rare, and we aim to shed further insight into these congenital processes so that operators may remain vigilant of them in their practice.
Keywords: Single coronary artery; Coronary angiography; Coronary artery anomaly; Right coronary artery
| Introduction | ▴Top |
Single coronary artery (SCA) is an unusual congenital anomaly that is sparsely reported in literature, seen by diagnostic coronary angiography in about 0.024% to 0.066% of cases [1-3]. It is commonly associated with other congenital cardiac malformations such as coronary arteriovenous fistula, bicuspid aortic valve [4], or transposition of the great vessels [5]. Absence of the right coronary artery (RCA) is one of the rarest coronary artery anomalies occurring when the artery does not develop in the right atrioventricular (AV) groove.
We report the case of a patient with new onset combined decompensated heart failure found to have an absent RCA with a left circumflex artery (LCX) that coursed through the AV groove extended, supplying the RCA territory.
| Case Report | ▴Top |
A 58-year-old male patient with history of type II diabetes mellitus and hypertension, not on any medications, presented to the emergency department with progressively increasing lower extremity edema, shortness of breath and dyspnea on minimal effort for the past 2 weeks. He has not been following with his physician for over a year.
Troponins were 0.01 for three consecutive sets, serum pro-brain type natriuretic protein (pro-BNP) was 12,066. Chest X-ray showed small bilateral pleural effusions and subsegmental left atelectasis. Electrocardiogram (ECG) revealed normal sinus rhythm and nonspecific T wave abnormalities. Total cholesterol was 221, triglycerides were 221, high-density lipoprotein (HDL) was 48 and low-density lipoprotein (LDL) was 171. Transthoracic echocardiogram showed a left ventricular ejection fraction (LVEF) of 25-30%, along with grade II diastolic dysfunction. The mitral valve leaflets were tethered due to reduced systolic function and elevated left ventricular diastolic pressure. Mild mitral regurgitation and a left pleural effusion were also visualized.
Cardiology evaluated the patient and started aspirin 81 mg, carvedilol 3.125 mg twice daily, Imdur 30 mg daily, and Lasix 40 mg intravenous (IV) twice daily. The patient was found to have subacute on chronic combined decompensated congestive heart failure and a left heart catheterization was recommended to rule out ischemic cardiomyopathy. Right radial arterial access was performed and indicated a left dominant coronary circulation with normal left main, medium sized left anterior descending artery (LAD) with mild atherosclerosis but no flow limiting lesions. The LCX was large and showed no angiographic evidence of disease. The AV groove extended and the LCX artery supplied the RCA domain. The ostial RCA was congenitally missing and not visualized on angiography (Fig. 1). The aortic pressures were found to be 108/45/76 mm Hg and the left ventricular pressures were found to be 114/4 mm Hg. The patient was discharged from the coronary catheterization laboratory with continuation of medications for aggressive medical management and risk factor modification.
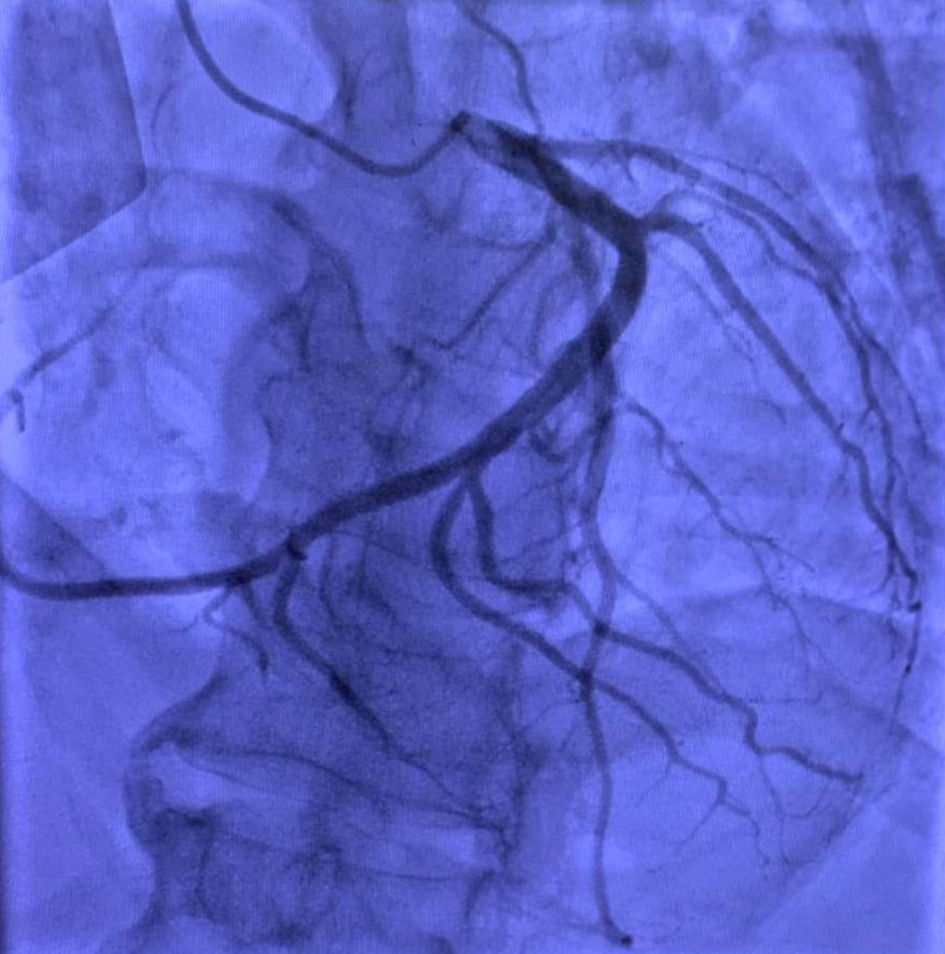 Click for large image | Figure 1. Coronary angiography showing a congenitally absent right coronary ostium and a large left circumflex artery extending down the atrioventricular groove and supplying the right coronary artery myocardial domain. |
| Discussion | ▴Top |
We discuss a rare case of SCA, particularly an absent RCA. The LCX extended down the AV groove thereby supplying the RCA territory. The ostial RCA was congenitally absent and not visualized on angiography. There were no other associated cardiac anomalies and only mild atherosclerosis of the LAD. Incidence of the RCA arising from the left coronary branches varies between 0.1% and 0.9%. To our knowledge, most reported cases involve the proximal or middle portion of the LAD as an origin of the RCA [6]. What is dangerous in this entity, is that patients with similar condition, have only one coronary blood flow system, which in case got affected, might lead to a catastrophic death, arrythmia or subsequent heart failure. Prognosis for patients with SCA ranges widely from normal life span to sudden cardiac arrest [1]. In the presence of other concomitant congenital anomalies, these patients might have higher risk of atherosclerosis, heart failure, or associated congenital cardiomyopathy [1]. In our case, the patient’s heart failure was non ischemic in origin; however, the patient did not follow up with our team; therefore, complete workup was not done, including cardiac magnetic resonance imaging. The SCA in this case was an incidental finding and was unrelated to the patient’s reduced ejection fraction.
There are numerous stratifications of SCA anomalies. The most employed is created by Lipton et al [1], describes the SCA according to origin and distribution of the coronary arteries. The anomalous coronary artery system is classified as either right or left depending on the origin of the dominant artery. When the RCA is arising from the terminal extension of the LCX artery, it is classified as LI. However, if the RCA arises from the left main (LM), LCX and LAD arteries, it will be classified as LIIA, LIIB and LIIP subgroups, respectively. Type III represents the LAD and LCX arteries that originate from the proximal part of the RCA [1]. This grouping was later modified by Yamanaka et al [7] with the addition of the septal and combined types, designated as “S” and “C”, for further classification of the anatomical variation [6]. Our case belongs to the LI type, due to the angiographic finding of the AV groove extension so that the LCX supplied the RCA territory in the absence of an RCA.
Absence of the RCA was found by Yamanaka et al [7] in only 20 patients who underwent cardiac catheterization, out of 126,595 with a frequency of only 0.016% [7]. The exact incidence is unknown, but there have been other reported cases [8-12], with at least 24 cases reported by Pourafkari et al [13].
Patients with congenital absence of the RCA can present with nonspecific symptoms and may be mislabeled as coronary artery disease (CAD) or remain undetected which may explain the low prevalence [14]. SCA, including group I anomalies, have been shown to have a variable clinical course, from benign to serious [6].
Patients can present with atypical chest pain without a significant CAD [15, 16], typical chest pain, unstable angina, dyspnea, and myocardial infarction [12] and sudden cardiac arrest [17]. It has also been reported that myocardial ischemia is a direct result of SCA in the absence of CAD in 15% of patients [18]. One-third of patients with type LI (four out of 12) have required coronary artery bypass graft (CABG) surgery according to Chou et al [19]. Pourafkari et al reported two out of 24 patients who required CABG and six out of 24 cases requiring percutaneous coronary intervention (PCI), with the remaining patients having benign courses [13].
Coronary angiography is the gold standard for diagnosis and classification of SCA [19]. SCA causes diagnostic difficulty during cardiac catheterization and cardiac surgery. Interventional cardiologists need to be familiar with the various categories of this congenital anomaly [17]. To our knowledge this case of a SCA presenting as dyspnea is barely reported [13]. While most patients improve with medical treatment, others require intervention. PCI in similar cases poses technical challenges, difficulties in cannulation of the coronary ostium as well as challenges with providing adequate catheter support due to abnormal origin and course [20].
During cardiac catheterization, when there are difficulties when visualizing the coronary arteries, clinicians should be aware of the potential for aberrant vessels. Being of aware of these abnormalities allows for prompt diagnosis and therapeutic decisions. Donaldson et al reported that in 28 of 75 cases (37%) cardiac catheterization was repeated due to inadequate visualization of the aberrant vessel. Of the patients studied, 15 were reinvestigated once, nine twice, three cases three times, and one four times until a correct diagnosis could be confidently made [21]. These anomalies, when observed in the index case, result in shorter procedure time, lesser quantity of dye, fewer catheter manipulations, and better angiographic images in subsequent cases as the anomalous course of the RCA was known [22].
Conclusions
We present a case of a patient presenting with signs and symptoms of subacute on chronic combined decompensated congestive heart failure, found to have a congenitally absent right coronary ostium on coronary angiography during left heart catheterization, to rule out ischemic cardiomyopathy as the etiology of heart failure. The LCX extended through the AV groove and supplied the territory of the RCA. Such coronary artery anomalies are infrequent, and we aim to shed further insight into these congenital anomalies so that operators may remain vigilant of them in their practice. Standard angiography is affected with these infrequent anomalies, and procedural complications might be higher.
Acknowledgments
We would like to thank the Internal Medicine Research Department at Staten Island University Hospital, especially the director of clinical research Maria Farberov for helping us finalize the project.
Financial Disclosure
This paper received no financial support from any third party.
Conflict of Interest
The authors declare that there is no conflict of interest.
Informed Consent
Patient consent for publication was obtained.
Author Contributions
All authors have participated in writing this case report. Hamfreth Rahming, Chetan Singh, Marc Assaad and Hussam Aridi helped drafting the manuscript. Michael Cinelli, Boutros Karam, and Ruben Kandov not only participated in writing the manuscript, but also followed the patient under their cardiology service, and were responsible for the coronary angiography along with the images that were obtained. Michael Cinelli is also responsible of the concept and Ruben Kandov has also a supervision role.
Data Availability
The authors declare that data supporting the findings of this paper are available within the article.
| References | ▴Top |
- Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979;130(1):39-47.
doi pubmed - Namgung J, Kim JA. The prevalence of coronary anomalies in a single center of Korea: origination, course, and termination anomalies of aberrant coronary arteries detected by ECG-gated cardiac MDCT. BMC Cardiovasc Disord. 2014;14:48.
doi pubmed - Turkmen S, Yolcu M, Sertcelik A, Ipek E, Dokumaci B, Batyraliev T. Single coronary artery incidence in 215,140 patients undergoing coronary angiography. Folia Morphol (Warsz). 2014;73(4):469-474.
doi pubmed - Ogden JA, Goodyer AV. Patterns of distribution of the single coronary artery. Yale J Biol Med. 1970;43(1):11-21.
- Longenecker CG, Reemtsma K, Creech O, Jr. Surgical implications of single coronary artery. A review and two case reports. Am Heart J. 1961;61:382-386.
doi - Elbadawi A, Baig B, Elgendy IY, Alotaki E, Mohamed AH, Barssoum K, Fries D, et al. Single Coronary Artery Anomaly: A Case Report and Review of Literature. Cardiol Ther. 2018;7(1):119-123.
doi pubmed - Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21(1):28-40.
doi pubmed - Ayala F, Badui E, Murillo H, Madrid R, Almazan A, Rangel A, Gutierrez-Vogel S. Right coronary ostium agenesis with anomalous origin of the right coronary artery from an ectasic circumflex artery. A case report. Angiology. 1995;46(7):637-639.
doi pubmed - Choi HY, Kim JW, Moon JM, Kim YJ, Choi CU, Lim HE, Kim EJ, et al. Unusual dominant course of left circumflex coronary artery to right coronary artery territory with absent right coronary artery. J Cardiol. 2010;55(1):117-119.
doi pubmed - Turhan H, Duru E, Yetkin E, Atak R, Senen K. Right coronary artery originating from distal left circumflex: an extremely rare variety of single coronary artery. Int J Cardiol. 2003;88(2-3):309-311.
doi - Singh S, Sahoo SK, Tripathy MP, Jena G. Angiographic Enigma: A single coronary artery with the right coronary artery originating from the distal left circumflex artery. Heart Views. 2015;16(3):104-106.
doi pubmed - Liu H, Guo X, Wang C, Li S, Shi Y. Congenital absence of the right coronary artery with superdominant left circumflex coronary artery. Int J Cardiol. 2012;158(1):e13-14.
doi pubmed - Pourafkari L, Taban M, Ghaffari S. Anomalous origin of right coronary artery from distal left circumflex artery: a case study and a review of its clinical significance. J Cardiovasc Thorac Res. 2014;6(2):127-130.
- Yan GW, Bhetuwal A, Yang GQ, Fu QS, Hu N, Zhao LW, Chen H, et al. Congenital absence of the right coronary artery: A case report and literature review. Medicine (Baltimore). 2018;97(12):e0187.
doi pubmed - Tanawuttiwat T, Harindhanavudhi T, Trivedi D. Anomalous single coronary artery with absent right coronary artery diagnosed with the aid of 64-slice multidetector computed tomographic angiography. Tex Heart Inst J. 2009;36(4):362-363.
- Lee HC, Lai HY, Hsieh KL, Lan GY. Characterizing an absent right coronary artery through 3-dimensional coronary computed tomography angiography. Rev Cardiovasc Med. 2018;19(3):111-112.
doi pubmed - Desmet W, Vanhaecke J, Vrolix M, Van de Werf F, Piessens J, Willems J, de Geest H. Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies. Eur Heart J. 1992;13(12):1637-1640.
doi pubmed - Shirani J, Roberts WC. Solitary coronary ostium in the aorta in the absence of other major congenital cardiovascular anomalies. J Am Coll Cardiol. 1993;21(1):137-143.
doi - Chou LP, Kao C, Lee MC, Lin SL. Right coronary artery originating from distal left circumflex artery in a patient with an unusual type of isolated single coronary artery. Jpn Heart J. 2004;45(2):337-342.
doi pubmed - Caliskan M, Ciftci O, Gullu H, Alpaslan M. Anomalous right coronary artery from the left sinus of Valsalva presenting a challenge for percutaneous coronary intervention. Turk Kardiyol Dern Ars. 2009;37(1):44-47.
- Donaldson RM, Raphael MJ. Missing coronary artery. Review of technical problems in coronary arteriography resulting from anatomical variants. Br Heart J. 1982;47(1):62-70.
doi pubmed - Shammas RL, Miller MJ, Babb JD. Single left coronary artery with origin of the right coronary artery from distal circumflex. Clin Cardiol. 2001;24(1):90-92.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.