

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 14, Number 2, April 2023, pages 123-132

Immobilizing Interstitial Cardiac Fibrosis
Yuriy L. Shevchenkoa ![]() , Alexey V. Plotnitskya, Daniil S. Ulbasheva, b
, Alexey V. Plotnitskya, Daniil S. Ulbasheva, b ![]()
aSt. George Clinic of Thoracic and Cardiovascular Surgery, Pirogov National Medical & Surgical Center, 105203 Moscow, Russia
bCorresponding Author: Daniil S. Ulbashev, St. George Clinic of Thoracic and Cardiovascular Surgery, Pirogov National Medical & Surgical Center, 105203 Moscow, Russia
Manuscript submitted January 12, 2023, accepted March 3, 2023, published online March 25, 2023
Short title: Immobilizing Interstitial Cardiac Fibrosis
doi: https://doi.org/10.14740/cr1467
| Abstract | ▴Top |
Background: The alterations in the endomysium and perimysium might cause compaction and gradual mechanical compression of cardiomyocytes resulting in their immobilization. This process finally leads to severe stiffening, so that the newly formed frame around individual cardiomyocytes and their clusters hinders normal diastole, and later systole. This phenomenon is referred to as immobilizing interstitial cardiac fibrosis (IICF). Deciphering the molecular and structural elements of myocardial changes is the key to understanding the pathogenetic foundations of heart failure development.
Methods: The study included 69 patients. Group I (n = 32) included patients with IICF; group II (n = 37) was comparison group. We evaluated the clinical picture, anamnesis of the disease, the results of physical examination, laboratory and instrumental examination of patients and autopsy data.
Results: In the anamnesis, patients with IICF were more likely to have diseases than patients in the control group: arrhythmia and impaired conductivity (88% vs. 19%, odds ratio (OR): 30.0; 95% confidence interval (CI): 7.918 - 113.7, P < 0.001), systemic connective tissue diseases (78% vs. 5%, OR: 62.5; 95% CI: 11.9 - 326.5, P < 0.001), viral infections (including severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)) (53% vs. 19%, OR: 4.86; 95% CI: 1.66 - 14.25, P = 0.003), type 2 diabetes mellitus (47% vs. 8%, OR: 10.0; 95% CI: 2.54 - 39.34, P < 0.001), radiation therapy for mediastinal lymphoma and other oncological diseases (19% vs. 0%, P = 0.008), focal infections (sinusitis, osteomyelitis, periodontitis, nephritis, cystitis, pyelonephritis, pleurisy, etc.) within 12 months (31% vs. 11%, P = 0.069), chronic kidney disease (25% vs. 8%, P = 0.097), and tuberculosis (9% vs. 0%, P = 0.095). We have identified a statistically significant difference between the groups: the volume of the fibrosis zone (17.5±9.2% vs. 4.9±2.3%, P = 0.001), the expression of type I collagen (5,182 ± 1,301 vs. 2,189 ± 754 in 1 mm2, P = 0.0001), type III collagen (7,562 ± 1,405 vs. 2,320 ± 541 in 1 mm2, P = 0.0001), matrix metalloproteinase (MMP)-2 (12,850 ± 6,200 vs. 9,501 ± 7,145 in 1 mm2, P = 0.005), MMP-9 (15,745 ± 5,695 vs. 6,920 ± 3,125 in 1 mm2, P = 0.0001), connexin-43 (25,689 ± 14,871 vs. 37,523 ± 12,561 in 1 mm2, P = 0.001), fibronectin (3,448 ± 720 vs. 1,544 ± 610 in 1 mm2, P = 0.0001), and transforming growth factor β (TGF-β) (5,121 ± 1,243 vs. 2,531 ± 1,489 in 1 mm2, P = 0.001).
Conclusion: IICF is a separate pathological condition and one of the main causes of chronic heart failure. It is induced by changes in the myocardial connective tissue that prevent normal functioning of the myocardium.
Keywords: Heart failure; Cardiac fibrosis; Connective tissue; Interstitial
| Introduction | ▴Top |
The most common cause of heart failure is a violation of the contractility of cardiomyocytes as a result of coronary artery disease (CAD), inflammation, excessive physical activity (including those in patients with congenital and acquired heart defects), metabolic diseases with electrolyte disorders, intoxication, myocardial contusion, tumors, etc. [1, 2].
However, many patients without any of the abovementioned conditions and any signs of lesions to the myocardium (as confirmed by instrumental or laboratory examinations, such as electrocardiography, echocardiography, scintigraphy, coronary angiography, measurement of laboratory markers, etc.) still suffer from severe heart failure. Standard therapy for heart failure is usually ineffective in these patients. None of the drugs, including cardiac glycosides, direct cardiotonic agents, diuretics, and other well-known medications give a significant clinical effect. As a result, heart failure is explained by cardiomyopathy with a poor prognosis [3, 4].
Many years of clinical practice and research (especially, macro- and micromorphological) and comprehensive analysis and comparison of different facts led us to a conclusion that such myocardial dysfunction might be caused by some mechanical factors located outside the clusters of healthy cardiomyocytes, but structurally close to them. It is connective tissue with altered physical properties, in particular, abnormal thickening, which prevents normal functioning of cardiomyocytes, thereby immobilizing them.
It is known that fibrogenesis is primarily caused by myofibroblasts formed as a result of fibroblast activation, as well as during epithelial-mesenchymal transformation [5-9]. In addition, macrophages, monocytes, T-lymphocytes, mast cells and endotheliocytes play a role in the process. Under the influence of fibrogenic mediators myofibroblasts synthesize collagen fibers, fibronectin, and profibrotic mediators, changing the structure of the extracellular matrix. The main fibrogenic mediators are matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMMP), as well as transforming growth factor β (TGF-β) [10-12]. An increase in the amount of I- and III-type collagen leads to changes in the structural organization of the endomysium and perimysium, violation of the electromechanical properties of the heart, immobilization of intact cardiomyocytes, which reduces the overall contractility of the left ventricle (LV) [13, 14]. Thus, deciphering the molecular and structural elements of myocardial rearrangement in immobilizing interstitial cardiac fibrosis (IICF) is the key to understanding the pathogenetic foundations of heart failure development.
| Materials and Methods | ▴Top |
This was a single-center retrospective observational study organized according to the “case-control” type. Our study was limited only to patients with morphological studies at autopsy, retrospectively such patients were analyzed by clinical, laboratory and instrumental studies. This study was conducted according to the Declaration of Helsinki. The permission for the research was received by the ethical committee of the Federal State Budgetary Institution “National Medical and Surgical Center named after N. I. Pirogov” of the Ministry of Health of the Russian Federation.
Group I (n = 32) included patients with IICF. Group II (n = 37) was comparison group (non-cardiac cause of death). The first group included patients with proven interstitial fibrosis of the heart, with a decrease in left ventricular function. Identification and quantification of myocardial fibrosis was determined by magnetic resonance imaging (MRI) data with delayed contrast (late gadolinium enhancement), and the final diagnosis was established according to morphology data. The control group included patients without interstitial fibrosis of the heart. The average age of patients was 60.25 ± 7.9 years in group I and 69.5 ± 5.4 years in group II (Table 1).
 Click to view | Table 1. Clinical and Demographic Characteristics of Patients |
Histological method
For morphological examination, the material was fixed in 10% neutral buffered formalin immediately after removal. Histological wiring was carried out in a vacuum apparatus by a standard method using isopropyl and ethanol. The material was poured into blocks of homogenized paraffin with a thickness of 5 mm. Histological sections, 4 - 5 µm thick, were made immediately before staining them with hematoxylin and eosin and conducting immunohistochemical reactions. Mounting of histological sections was carried out on positively charged glasses with drying in accordance with the manufacturer’s recommendations. The obtained sections were dewaxed and stained with hematoxylin and eosin according to the standard procedure. Staining of the sections according to Van Gieson and Masson (trichrome method) was carried out using ready-made kits (Bio-Optica, Italy) in accordance with the attached instructions.
Immunohistochemical method
Immunohistochemical staining was performed by an automated method using the Ventana BenchMark Ultra immunohistostainer with dewaxing and unmasking in the apparatus. The expression of MMP-2, MMP-9, tenascin-C, B-cell lymphoma 2 (Bcl-2), connexin-43, collagen types I and III, and TGF-β was studied. In all the cases, a standardized detection system with a benzidine label and an indirect method of detecting ultra VIEWDAB without additional signal amplification was used.
Morphometric method
The intensity of expression of these markers was evaluated automatically using the QuPath v0 platform.2.3 on a four-point scale, where 0 indicates an absence of manifestation, and 3 indicates a pronounced expression. The number of positive cells was calculated in the areas of arbitrary size, followed by the calculation of the average value of positive cells in 1 mm2 area. The illustrative material was obtained using the Ventana iScan HT histological scanner (Roche Diagnostics).
Statistical method
Statistica 12 was used for statistical processing. The normality of the distribution was assessed using the Shapiro-Wilk and Kolmogorov-Smirnov criteria. Taking into account the non-normal distribution of all quantitative indicators, the analysis was performed using the nonparametric Mann-Whitney U-test. The comparison of percentages in the analysis of four-field conjugacy tables was performed using Pearson’s Chi-squared criterion (with values of the expected phenomenon greater than 10), and Fisher’s exact criterion (with values of the expected phenomenon less than 10). The odds ratio was calculated for risk factors. The results of the study are presented as the arithmetic mean ± standard deviation (M ± σ). The critical significance level (P) was taken to be 0.05 when testing hypotheses.
| Results | ▴Top |
Clinical signs of IICF
The most important clinical manifestation of immobilizing interstitial fibrosis is idiopathic heart failure unresponsive to standard therapy. The immobilization of cardiomyocyte clusters impairs the diastolic function, slowly reduces left ventricular ejection fraction (LVEF), and affects the pulmonary and later systemic circulation.
There are five stages of the disease: I - latent asymptomatic stage (early changes in connective tissue); II - stage of minimal manifestations (moderate fibrosis with increased levels of type I and type III collagen); III - stage of diastolic dysfunction (severe fibrosis with a significant predominance of type I collagen); IV - stage of systolic and diastolic dysfunction (severe fibrosis); V - stage of coronary angiopathy (extremely severe fibrosis involving the coronary arteries).
In the anamnesis of patients with fibrosis, the most common diseases were: arrhythmia and impaired conductivity, systemic connective tissue diseases, viral infections (including severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)), type 2 diabetes mellitus, focal infections (sinusitis, osteomyelitis, periodontitis, nephritis, cystitis, pyelonephritis, pleurisy, etc.), chronic kidney disease, radiation therapy for mediastinal lymphoma, thyroid diseases, and tuberculosis (Table 2).
Click to view | Table 2. Concomitant Diseases in Patients |
If coronary bypass surgery or endovascular surgery on the coronary arteries did not improve cardiac activity (no increase/decrease in LVEF) and heart failure aggravated, the patient might have severe post-infarction IICF.
The absence of isolated sites of impaired myocardial contractility along with a decreased systolic function at later stages is an important echocardiographic and scintigraphic sign of IICF, which makes it different from ischemic fibrosis (Figs. 1, 2). However, patients with extremely severe fibrosis with perivasal immobilization of arterioles at the stage of coronary angiopathy may have areas of hypoperfusion and hypokinesia.
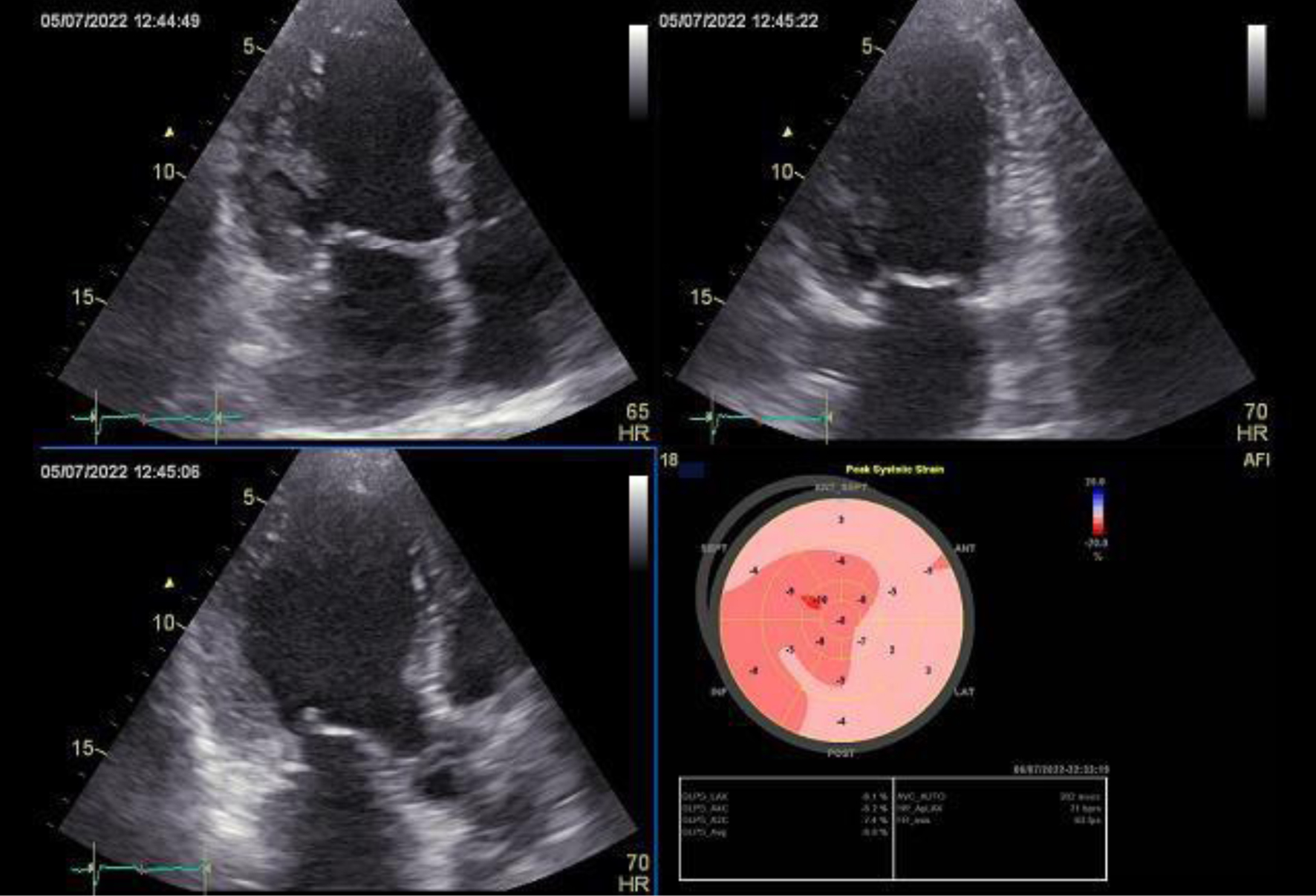 Click for large image | Figure 1. Echocardiography of a 67-year-old male patient showing immobilizing interstitial cardiac fibrosis. Diffuse decrease in LV myocardial contractility was noted. LV contractility was reduced. Total LVEF was 41%. LVEF: left ventricular ejection fraction. |
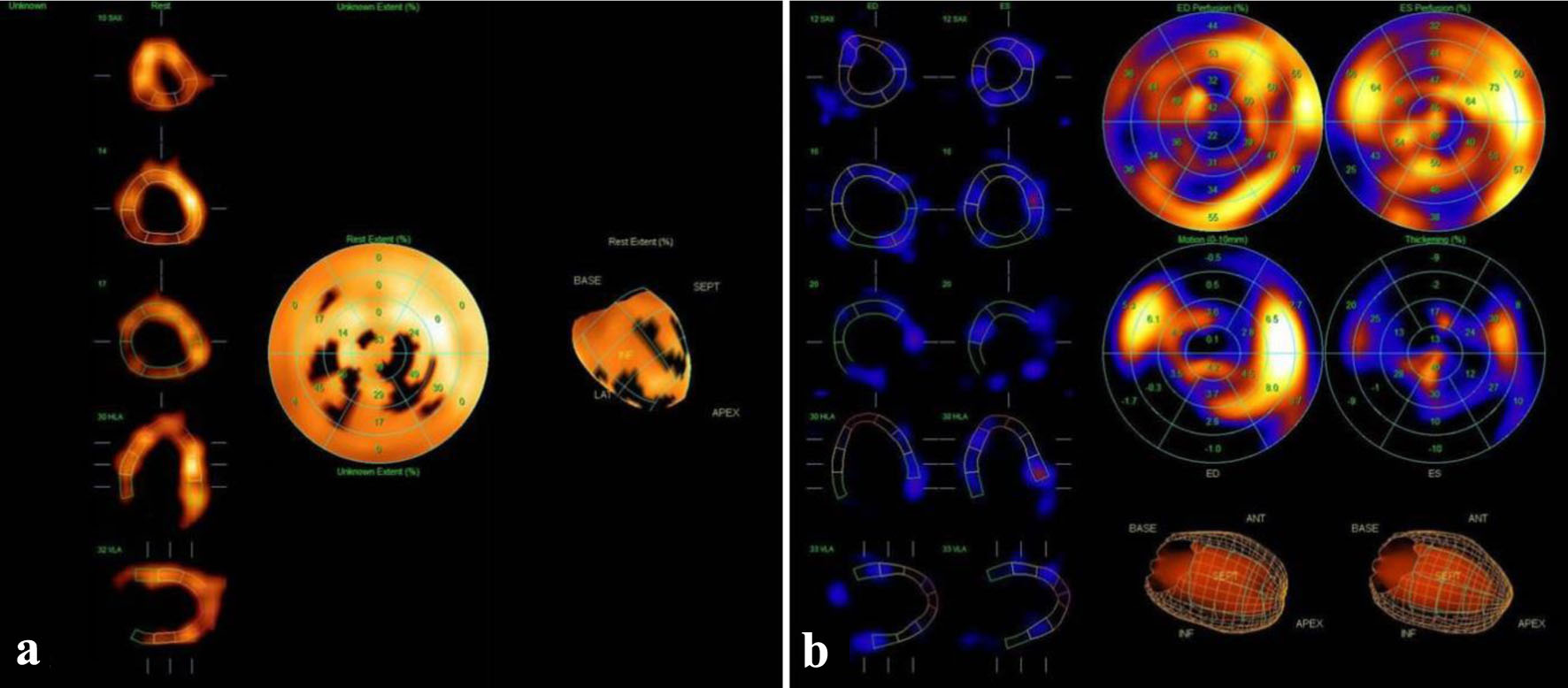 Click for large image | Figure 2. 99mTc scintigraphy of the myocardium (a: LV myocardial perfusion; b: LV myocardial function) of a 49-year-old male patient showing immobilizing interstitial cardiac fibrosis. Diffuse decrease in perfusion and diffuse decrease in regional systolic wall thickening in the entire LV myocardium without a clear differentiation between the areas of local hypoperfusion and local hypokinesia were noted. LV contractility was significantly decreased. Total LVEF was 37%. LVEF: left ventricular ejection fraction. |
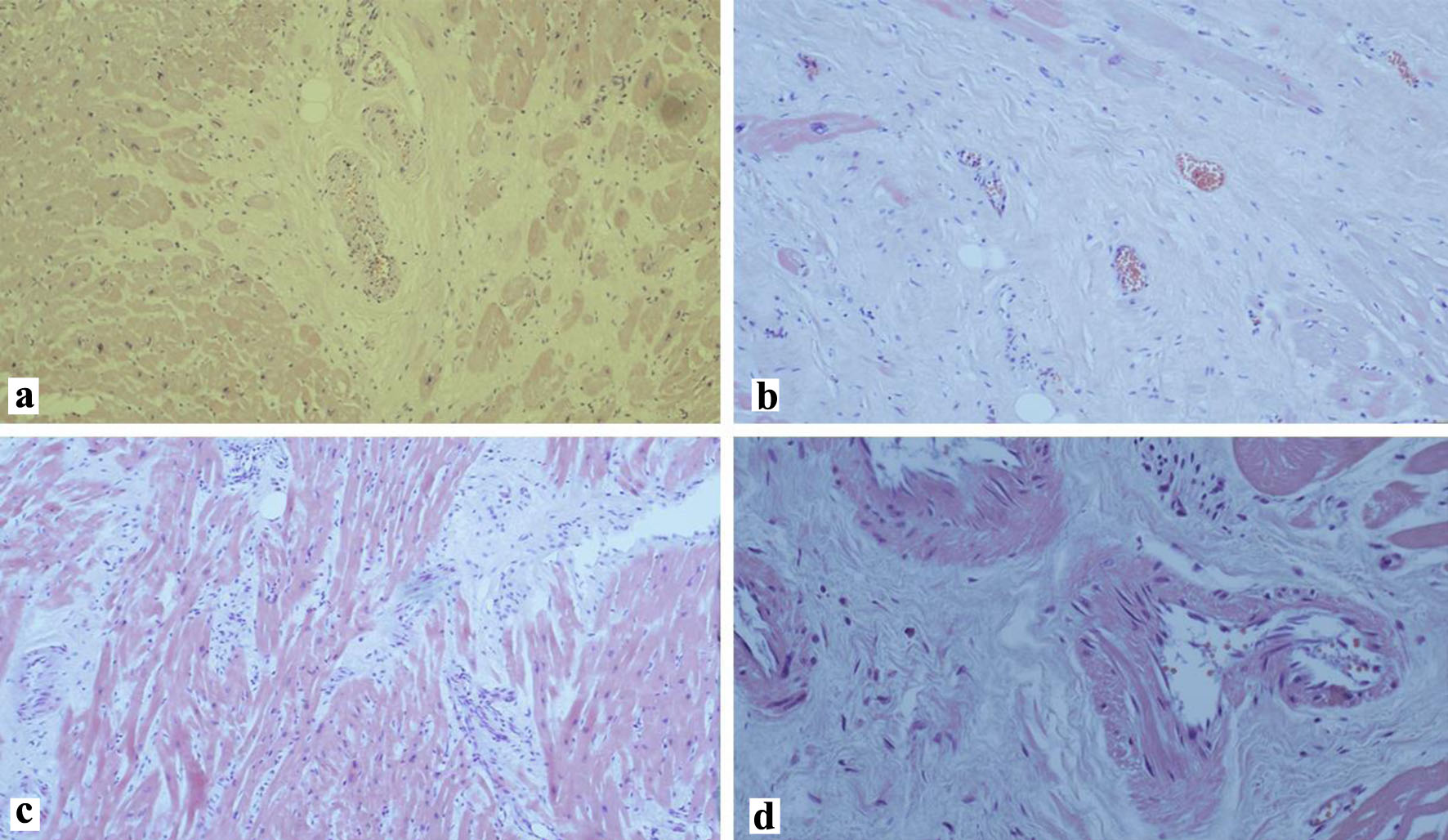
Under certain conditions, post-infarction scarring can induce the development of immobilizing interstitial fibrosis. In this case, perifocal connective tissue starts producing specific mediators, which triggers the formation of dense connective tissue around healthy cardiomyocytes resulting in diffuse interstitial fibrosis with further aggravation of cardiomyocyte immobilization. Heart failure in these patients is caused by a combination of ischemic heart disease, on the one hand, and induced IICF in the non-ischemic areas, on the other hand (Fig. 3).
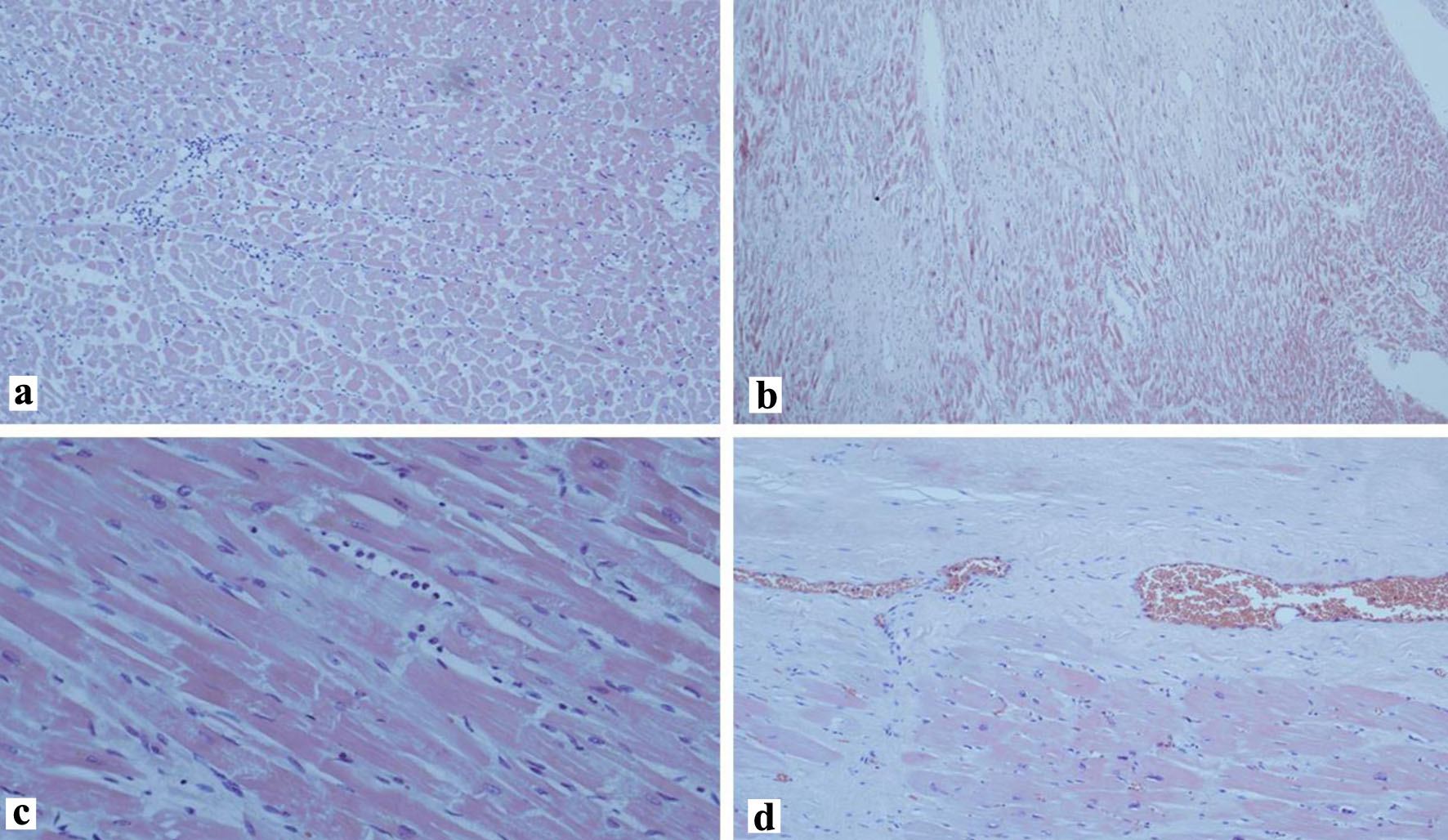 Click for large image | Figure 3. Diffuse spread of induced immobilizing interstitial cardiac fibrosis in a 68-year-old male patient. (a-c) Early stages (approximately 1 month). (d) Extravascular compression of coronary arterioles, areas of scarring (hematoxylin and eosin stain, a: × 100, b: × 80, c, d: × 40). |
Morphology
Volume of the fibrosis zone
The average area of fibrosis zones (% ratio of fibrosis sites to the total area of the examined tissue fragment) was estimated on the preparations stained according to the methods of Weigert, Masson and Van Gieson: 17.5±9.2% in group I and 4.9±2.3% in group II (P = 0.001) (Fig. 4). It turned out that with a diffuse increase in the volume of interstitial fibrosis in the first group, there occurred compression of functionally active cardiomyocytes - their immobilization.
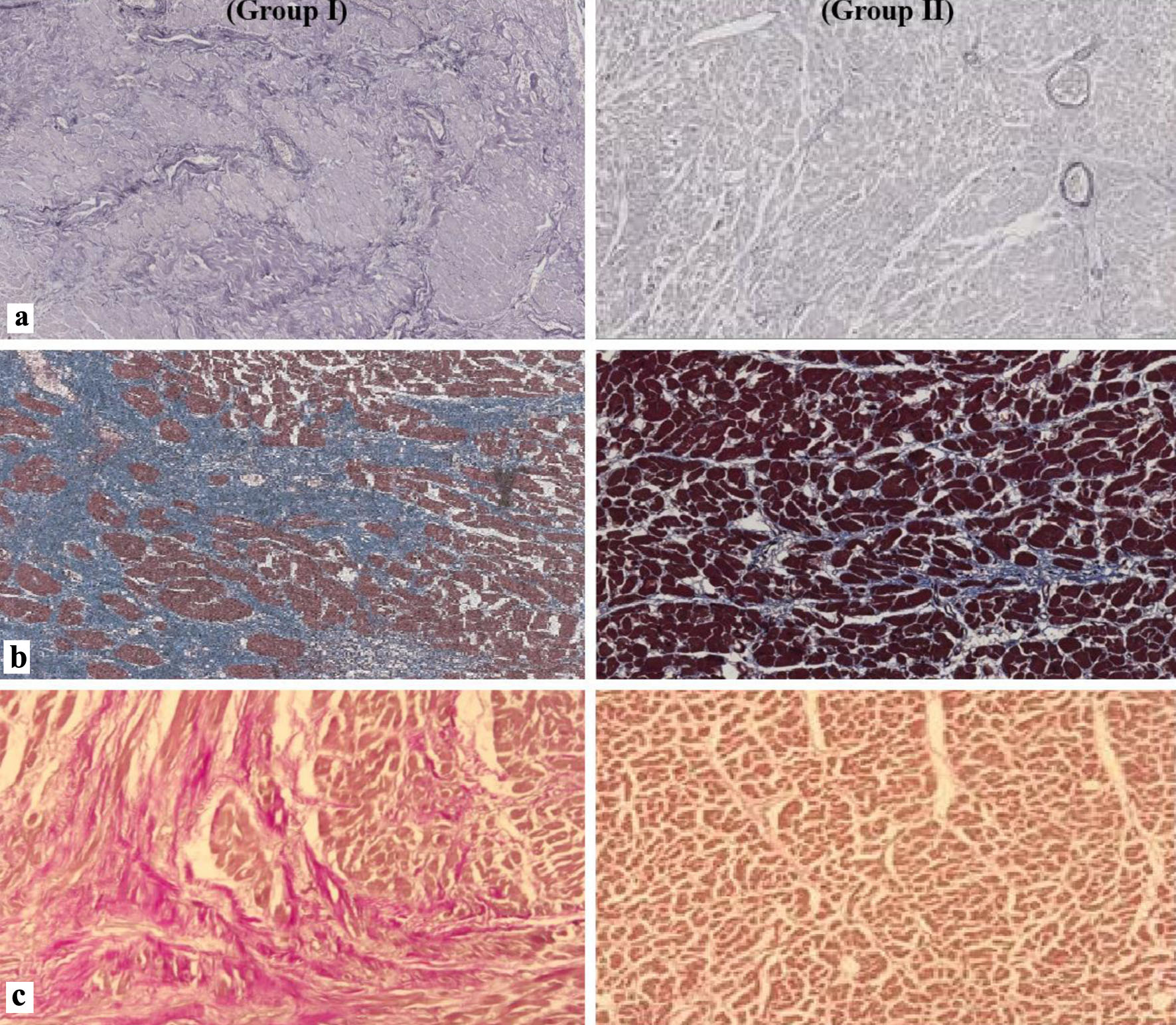 Click for large image | Figure 4. Histological preparations of the myocardium showing a significant increase in the volume of connective tissue in group I patients. (a) Weigert’s stain, × 100. (b) Masson’s stain, × 200. (c) Van Gieson’s stain, × 200. |
In the first group, in cases of the extremely severe stage of IICF, extravasal compression of the myocardial arterioles with the development of significant coronary insufficiency, resulting in myocardial infarction, was revealed (Fig. 5).
 Click for large image | Figure 5. The stage of coronary angiopathy (in group I) is an extremely severe degree of fibrosis with constriction of the peripheral coronary bed (hematoxylin and eosin stain, a-c: × 200, d: × 400). |
I and III collagen
There was a significant increase in the number of type I collagen fibers in patients with IICF (5,182 ± 1,301 in 1 mm2) relative to the comparison group (2,189 ± 754 in 1 mm2) (P = 0.0001). The fibers were arranged randomly, forming network-like structures (Fig. 6a). The amount of type III collagen was also higher in group I: 7,562 ± 1,405 in 1 mm2 (vs. 2,320 ± 541 in 1 mm2 in group II) (P = 0.0001) (Fig. 6b).
 Click for large image | Figure 6. (a) Type I collagen fibers in group I chaotic intersection of bundles forming closed spaces around individual cardiomyocytes; in group II ordered arrangement of collagen fibers. (b) Type III collagen fibers in group I disordered arrangement, without clearly distinguishable spatial structures; in group II rare bundles of collagen fibers (Weigert’s stain, × 400). |
MMPs
Immunohistochemical examination revealed that the expression of MMPs (MMP-2 and MMP-9) in the myocardium is determined in the cytoplasm of cardiomyocytes, endotheliocytes and fibroblasts of interstitial tissue. To assess the level of their expression, cardiomyocytes and fibroblasts were selected as the main target cells for myocardial remodeling. The average amount of MMP-2 was 12,850 ± 6,200 in 1 mm2 in group I and 9,501 ± 7,145 in 1 mm2 in group II (P = 0.005) (Fig. 7a). A significant difference between the groups in the expression of MMP-9 was revealed. The average number of MMP-9 cardiomyocytes and fibroblasts was 15,745 ± 5,695 in 1 mm2 in group I and 6,920 ± 3,125 in 1 mm2 in group II (P = 0.0001) (Fig. 7b).
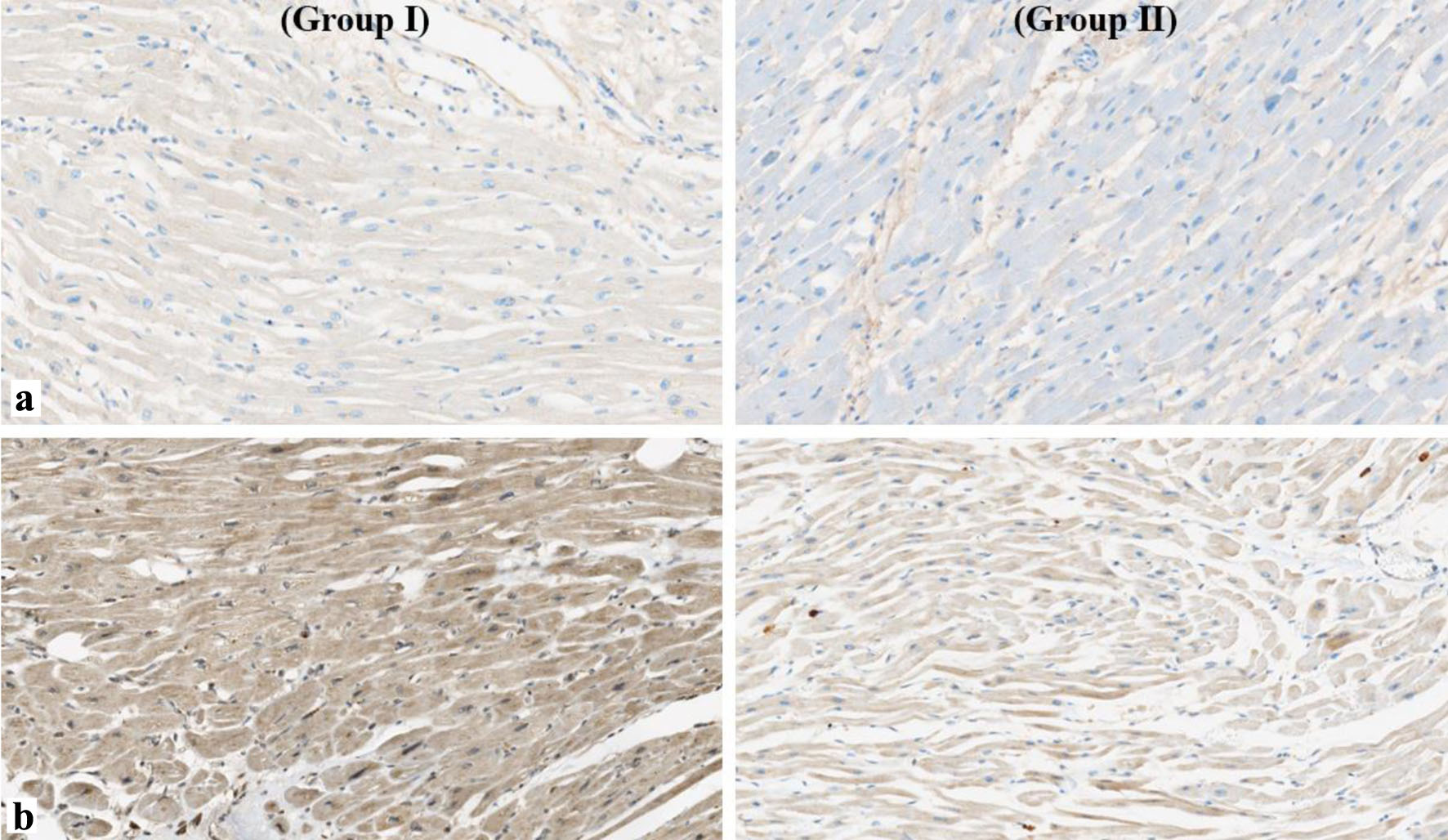 Click for large image | Figure 7. Metalloproteinase expression: (a) MMP-2 (immunohistochemical study, × 200 increase); (b) MMP-9 (immunohistochemical stain, × 200). MMP: matrix metalloproteinase. |
MMPs, especially MMP-9, are very “sensitive” markers of the initial stages of fibrosis. Their content begins to increase primarily due to the appearance of local fibrohistiocytes in the cytoplasm and blood cell elements migrating from the vessels. This indicates a running mechanism of irreversible changes in this part of the myocardium and announces its future deep structural transformation in IICF.
Tenascin-C
Normally, tenascin-C was not found in healthy adult heart tissues, with the exception of tendon chords of papillary muscles and at the base of the heart valve flaps. It is induced or suppressed in developed tissues during damage, remodeling and neoplasms. Directly within the heart tenascin-C interacts with fibronectin, resulting in the expression of MMPs regulation, which is a reliable biomarker of the progression of heart failure and a poor prognosis for such patients. It was determined that tenascin-C appears in the area of acute injury during myocardial infarction, in adjacent areas, and at the initial stages of the formation of immobilizing interstitial fibrosis. It can persist for 14 - 21 days. Tenascin-C expression was not detected in the formed “mature” fibrous zones of the myocardium.
Bcl-2
Bcl-2 is a protein belonging to the family of anti-apoptotic proteins. It is a key factor in the resistance of cardiac fibroblasts to programmed cell death. The resistance of cardiac fibroblasts/myofibroblasts to mitochondrial-dependent apoptosis emphasizes their increased potential in hypoxia.
This protein was detected in the cytoplasm of both cardiomyocytes and fibroblastic cellular elements in the myocardium adjacent to fibrosis or involved in the process zones. The expression of Bcl-2 in patients without a diagnosis of myocardial infarction can serve as one of the criteria indicating the existing interstitial fibrosis. In group II, the expression of Bcl-2, as well as tenascin-C, was not detected.
Connexin-43
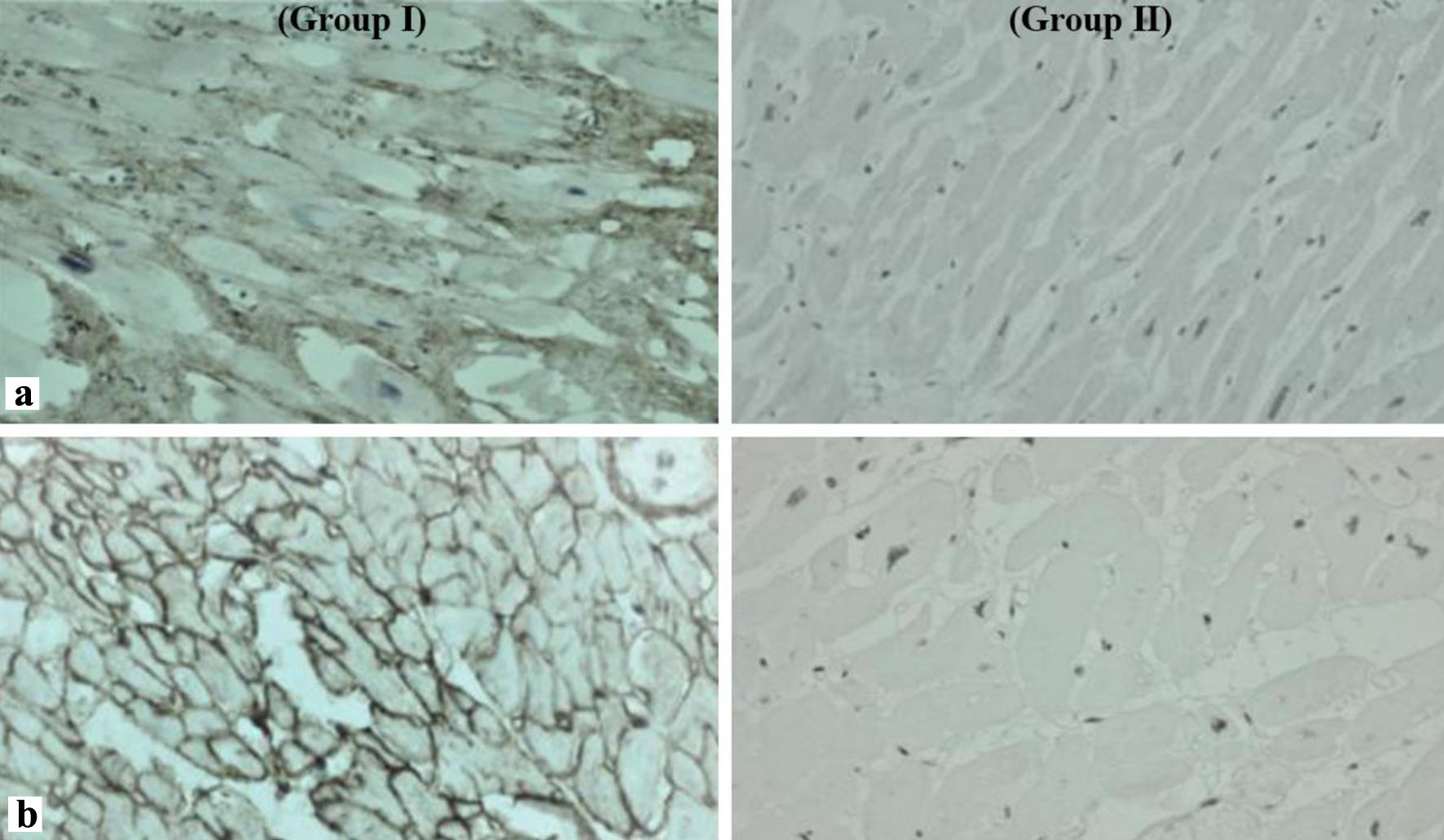
The expression of connexin-43 in group I (25,689 ± 14,871 in 1 mm2) was found in smaller amounts, in contrast to group II (37,523 ± 12,561 in 1 mm2) (P = 0.001). In IICF, connexin-43 was “lateralized”, whereas in patients with healthy myocardium, connexin-43 was detected mainly in the area of insertion discs of cardiomyocytes.
Fibronectin
In the autopsy group of patients with IICF, there was a significant increase in the expression of fibronectin by myofibroblasts and fibroblasts (3,448 ± 720 in 1 mm2) compared with the second group, where it was ill-defined (1,544 ± 610 in 1 mm2) (P = 0.0001).
TGF-β
There were differences in the expression of TGF-β: 5,121 ± 1,243 in 1 mm2 in group I and 2,531 ± 1,489 in 1 mm2 in group II (P = 0.001).
| Discussion | ▴Top |
Many factors (such as viral infections, toxic or radiation effects, autoimmune disorders, etc.) can change the molecular phenotype of the cardiac connective tissue via increasing the expression of fibrogenic mediators, which leads to abnormal ratio of different collagen types and triggers excessive collagen synthesis. The extracellular matrix is remodeled with the formation of network-like structures surrounding healthy cardiomyocytes.
Given the high reactivity of connective tissue, pathological changes usually begin with a pronounced edema. At first, cardiomyocytes remain intact and can maintain normal cardiac contractility. However, gradual thickening of interstitial tissue prevents full relaxation of the cells, thereby affecting the diastolic function. Instead of easy sliding over each other, cardiomyocyte becomes tightly bound and surrounded by thick layers of connective tissue.
Myogenic autoregulation (Frank-Starling mechanism) no longer works in this case. The ventricles are unable to cope with volume overload; left and right ventricular performance cannot be equalized; normal amount of circulating blood and blood pressure cannot be effectively maintained.
Notably, in this case the mechanics of cardiac muscle contraction is generally affected. Severe fibrosis changes the specific structure of the intramyocardial fasciae and prevents normal wringing motion of heart, which, firstly, is crucial in saving energy of heart external work and, secondly, ensures laminar blood flow. IICF increases the myocardial load and changes the configuration of intracardiac hemodynamics.
Compression of the peripheral parts of the coronary arteries is a particularly important step in fibrosis progression; it starts with arterioles, where the muscle layer is relatively thin. Patients can develop clinical and instrumental signs of coronary insufficiency unresponsive to appropriate therapy. Arterial compression by the surrounding connective tissue leads to angiopathy. As a result, peripheral arterioles are affected; the main coronary arteries are more likely to be constricted due to an impaired nervous regulation. Only histological examination at autopsy can show changes in connective tissue and perivascular immobilization. At this stage, primary interstitial cardiac fibrosis might cause acute myocardial infarction due to extravasal constriction of arterioles.
The main cause of myocardial fibrosis is overproduction of type I and III collagen. The synthesis of type I collagen prevails, which explains stiffening of the newly formed connective tissue.
Type I collagen is arranged in chaotic intersecting fibrils and networks that form confined spaces around individual cardiomyocytes. This frame also includes more numerous fibrils of type III collagen, arranged randomly and without distinguishable spatial structures.
Immunohistochemical staining allowed us to detect an increased expression of MMP-2 and MMP-9. These molecules are produced by immune cells and fibroblasts of interstitial cardiac tissue and are involved in endomysium and perimysium remodeling. MMP-2 and MMP-9 are detected at the first stage of normal connective tissue destruction.
Patients with severe myocardial fibrosis demonstrate lower expression of connexin-43 and its lateralization in cardiomyocytes, along with an increased expression of MMPs. This affects the conductivity and permeability for Na+ ions, reducing the number of pulses passing through the contact. We also detected the expression of other fibrogenic markers, such as TGF-β, tenascin C, Bcl-2, and fibronectin.
Patients with IICF develop changes in the structure of connective tissue surrounding separate cardiomyocytes and their clusters: it becomes thicker. Such changes affect lymphatic system causing its sclerosis and impaired lymphatic drainage.
Limitations of the study
Our study has limitations that should be given due attention. Firstly, the study included a small number of observations. Secondly, this is a single-center, retrospective, non-randomized study, so these results cannot be generalized to the entire population of patients with interstitial heart fibrosis. Thirdly, while there are no precise laboratory and instrumental criteria for immobilizing interstitial fibrosis of the heart, a comprehensive diagnosis and comparison of data is necessary, and a histological examination of the heart can serve as the final confirmation of the diagnosis. Fourth, there was only one control group. The next step is to study the data of patients with a large sample size, conducting multicenter, randomized trials.
Conclusion
Thus, deciphering the molecular and structural foundations of myocardial rearrangement in fibrosis is the key to understanding the pathogenetic foundations of the development of heart failure.
Primary IICF develops due to the changes in connective tissue that are often the root cause of myocardial dysfunction. Healthy cardiomyocytes experience mechanical compression from the outside, which results in their restricted motion and impaired cardiac function. The disease develops slowly: from minor enlargement of the interstitium to severe fibrosis with arteriole compression and myocardial trophic impairment.
Secondary (induced) IICF develops due to diffuse changes in the interstitial tissue of the healthy myocardium after its stimulation by post-infarction scars.
The use of immunohistochemical studies and the determination of markers of fibrous rearrangement can contribute to the diagnosis of IICF in its early stages and the possibility of preventing the worsening severity of heart failure.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Not applicable.
Author Contributions
Yuriy L. Shevchenko made significant contribution to the concept and design of the study, editing, approval of the final version, and was fully responsible for the content. Alexey V. Plotnitsky and Daniil S. Ulbashev contributed to data collection, analysis and interpretation, manuscript writing, editing, approval of the final version, and were fully responsible for the content.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Bui AL, Horwich TB, Fonarow GC. Epidemiology and risk profile of heart failure. Nat Rev Cardiol. 2011;8(1):30-41.
doi pubmed pmc - Giamouzis G, Triposkiadis F, Butler J, Westermann D, Giannakoulas G. Heart failure. Cardiol Res Pract. 2011;2011:159608.
doi pubmed pmc - Shevchenko YuL. The immobilizing interstitial fibrosis of the heart. Vestnik NMHC im. N.I. Pirogova. 2022;17(2):4-10. (In Russ).
doi - Shevchenko YuL, Ulbashev DS. The immobilizing interstitial fibrosis of the heart. Part II. Vestnik NMHC im. N.I. Pirogova. 2022;17(3):4-10. (In Russ).
doi - Swierblewska E, Wolf J, Kunicka K, Graff B, Polonis K, Hoffmann M, Chrostowska M, et al. Prevalence and distribution of left ventricular diastolic dysfunction in treated patients with long-lasting hypertension. Blood Press. 2018;27(6):376-384.
doi pubmed - van de Wouw J, Broekhuizen M, Sorop O, Joles JA, Verhaar MC, Duncker DJ, Danser AHJ, et al. Chronic kidney disease as a risk factor for heart failure with preserved ejection fraction: a focus on microcirculatory factors and therapeutic targets. Front Physiol. 2019;10:1108.
doi pubmed pmc - van Riet EE, Hoes AW, Wagenaar KP, Limburg A, Landman MA, Rutten FH. Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur J Heart Fail. 2016;18(3):242-252.
doi pubmed - Mocan M, Mocan Hognogi LD, Anton FP, Chiorescu RM, Goidescu CM, Stoia MA, Farcas AD. Biomarkers of inflammation in left ventricular diastolic dysfunction. Dis Markers. 2019;2019:7583690.
doi pubmed pmc - de Boer RA, De Keulenaer G, Bauersachs J, Brutsaert D, Cleland JG, Diez J, Du XJ, et al. Towards better definition, quantification and treatment of fibrosis in heart failure. A scientific roadmap by the Committee of Translational Research of the Heart Failure Association (HFA) of the European Society of Cardiology. Eur J Heart Fail. 2019;21(3):272-285.
doi pubmed pmc - Suthahar N, Meijers WC, Sillje HHW, de Boer RA. From inflammation to fibrosis-molecular and cellular mechanisms of myocardial tissue remodelling and perspectives on differential treatment opportunities. Curr Heart Fail Rep. 2017;14(4):235-250.
doi pubmed pmc - Legere SA, Haidl ID, Legare JF, Marshall JS. Mast Cells in Cardiac Fibrosis: New Insights Suggest Opportunities for Intervention. Front Immunol. 2019;10:580.
doi pubmed pmc - Nevers T, Salvador AM, Velazquez F, Ngwenyama N, Carrillo-Salinas FJ, Aronovitz M, Blanton RM, et al. Th1 effector T cells selectively orchestrate cardiac fibrosis in nonischemic heart failure. J Exp Med. 2017;214(11):3311-3329.
doi pubmed pmc - Piek A, de Boer RA, Sillje HH. The fibrosis-cell death axis in heart failure. Heart Fail Rev. 2016;21(2):199-211.
doi pubmed pmc - Shevchenko YuL. Consecutive contraction of cardiomyocytes and their clusters. A new concept of the heart physiology. Immobilizing interstitial cardiac fibrosis. Moscow: Publishing House - National Medical and Surgical Center named after N.I.Pirogov. 2022.
doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.