

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 14, Number 2, April 2023, pages 97-105

Chest Pain in Acute Myocardial Infarction and Its Association With the Culprit Artery and Fibrotic Segment Identified by Cardiac Magnetic Resonance
Weverton Ferreira Leitea, g ![]() , Rui Manuel dos Santos Povoaa, Adriano Mendes Caixetab, Celso Amodeoa, Gilberto Szarfc, Maria Teresa Nogueira Bombiga, Maria Cristina Oliveira Izard, Luciana Netto Gioiae, Wilma Noia Ribeirof, Francisco Antonio Helfenstein Fonsecad
, Rui Manuel dos Santos Povoaa, Adriano Mendes Caixetab, Celso Amodeoa, Gilberto Szarfc, Maria Teresa Nogueira Bombiga, Maria Cristina Oliveira Izard, Luciana Netto Gioiae, Wilma Noia Ribeirof, Francisco Antonio Helfenstein Fonsecad
aDepartment of Hypertensive Heart Disease, Escola Paulista de Medicina, Universidade Federal de Sao Paulo, SP, Brazil
bDepartment of Hemodynamics, Escola Paulista de Medicina, Universidade Federal de Sao Paulo, SP, Brazil
cDepartment of Magnetic Resonance, Escola Paulista de Medicina, Universidade Federal de Sao Paulo, SP, Brazil
dDepartment of Lipids, Atherosclerosis and Vascular Biology, Escola Paulista de Medicina, Universidade Federal de Sao Paulo, SP, Brazil
eEscola Paulista de Medicina, Universidade Federal de Sao Paulo, SP, Brazil
fDepartment of Coronary Artery Disease, Escola Paulista de Medicina, Universidade Federal de Sao Paulo, SP, Brazil
gCorresponding Author: Weverton Ferreira Leite, Department of Hypertensive Heart Disease, Escola Paulista de Medicina, Universidade Federal de Sao Paulo, Paraiso, Sao Paulo - SP, CEP 01321-000, Brazil
Manuscript submitted January 16, 2023, accepted March 18, 2023, published online April 8, 2023
Short title: Chest Pain, Culprit Artery, Fibrosis in AMI
doi: https://doi.org/10.14740/cr1468
| Abstract | ▴Top |
Background: It is still very controversial whether the characteristics of pain in the acute myocardial infarction could be related to the culprit coronary artery. There are no data about associations of pain with the ST-segment elevation myocardial infarction (STEMI) and left ventricular (LV) fibrotic segments.
Methods: Data from 328 participants who had STEMI and were included in the B and T Types of Lymphocytes Evaluation in Acute Myocardial Infarction (BATTLE-AMI) study were analyzed. The culprit artery was identified by coronary angiography and the injured myocardial segments by cardiac magnetic resonance. The statistical significance was established by P value < 0.05.
Results: A total of 223 patients (68%) were selected. Association was not observed between chest pain and the culprit artery (P = 0.237), as well as between pain irradiation and the culprit artery (P = 0.473). No significant difference was observed in the pain localization in relation to the segments in the short axis basal, mid, apical, and long axis, except for the mid inferior segment. The data were not considered clinically relevant because this association was observed in only one of 17 segments after multiple comparisons.
Conclusions: In patients with STEMI, no associations were observed between the location or irradiation of acute chest pain and/or adjacent areas and the culprit artery, or between pain and segmental myocardial fibrosis in the LV.
Keywords: Chest pain; Myocardial infarction; Culprit coronary artery; Fibrosis; Cardiac magnetic resonance imaging
| Introduction | ▴Top |
Cardiovascular diseases are the main cause of death in Brazil and in the world, especially because of acute myocardial infarction (AMI) [1, 2]. Despite the contemporary advances in technology and diagnostic imaging, the clinical history should not be disbelieved and downgraded to the background in the search for suitable diagnosis of AMI.
“Angina pectoris is the most important clinical expression of coronary insufficiency or myocardial hypoxia” [3]. “Chest pain is the most common symptom of coronary artery disease and should not be described as typical but as cardiac, possibly cardiac and non-cardiac” [4].
Although the clinical characteristics of pain in some patients could be similar between AMI and unstable angina, this symptom is more intense in AMI, because the severity of ischemia is more prolonged, to the point of causing enough myocardial damage to release necrosis markers [5].
To Braunwald et al [6], the angina pectoris could be defined as discomfort in the chest and/or adjacent areas associated with myocardial ischemia, but without myocardial necrosis. Angina means tightness and not pain. According to this concept, it is not appropriate to speak of angina in AMI, but rather of acute cardiac pain.
In the past, it had believed that the localization and irradiation of the cardiac pain in coronary artery disease were associated with the culprit coronary artery [3]. Our aim was to evaluate whether these characteristics of the cardiac pain were associated with the artery responsible for the ST-segment elevation myocardial infarction (STEMI).
We believe that this information could help in the identification of the culprit artery in patients with occlusion in more than one coronary artery, and in situations in which there were difficult to identify the infarcted wall on the electrocardiogram, as left bundle branch block.
In the current management of the STEMI, the staged completed revascularization is recommended in patients presenting with multivessel coronary disease [7, 8]. Therefore, the association between the characteristics of the chest pain and culprit artery could be used in the algorithms of the management of patients with STEMI.
Furthermore, we evaluated if the cardiac pain was also related with the 17 injured left ventricular (LV) myocardial segments, analyzed by means of cardiac magnetic resonance (CMR). To the best of our knowledge, this new data would be added in the literature: the association between LV segmental anatomical and the clinical history.
Objective
The objective of this study was to assess the associations between the characteristics of acute chest pain and/or pain in adjacent areas and the artery responsible for the STEMI and the 17 injured LV myocardial segments.
| Materials and Methods | ▴Top |
The study was performed from the database of the 328 patients who were admitted to the emergency room of the Hospital Sao Paulo, Escola Paulista de Medicina of the Universidade Federal de Sao Paulo with AMI and those who were included in the B and T Types of Lymphocytes Evaluation in Acute Myocardial Infarction (BATTLE-AMI) [9] study, with the registration site (clinicaltrials.gov, identifier NCT02428374). The culprit artery was identified by coronary angiography and the injured LV myocardial segments by CMR.
All participants or their representatives signed an informed consent form, and the study was approved by the Ethics and Research Committee of Hospital Sao Paulo on November 25, 2014 under number 940.105. This study was performed in line with the principles of the Declaration of Helsinki.
LV myocardium segmentation
The associations among cardiac pain, the culprit artery and the 17 LV myocardial segments injured in AMI were assessed by using the schematic representation of the American Heart Association Scientific Statement [10]. In this representation, left anterior descending (LAD) coronary artery supplies the following segments: basal anterior, basal anteroseptal, mid anterior, mid anteroseptal, apical anterior e apical septal and apex.
The segments which are assigned to the dominant right coronary artery (RCA) are basal inferoseptal, basal inferior, mid inferoseptal, mid inferior and apical inferior. Left circumflex (LCX) artery supplies the basal inferolateral, basal anterolateral, mid inferolateral, mid anterolateral and apical lateral segments.
Semiology of pain
A search was carried out on the data from the clinical records in the BATTLE-AMI [9] study to obtain information about the semiology of pain located between the upper abdomen and the nasal region related to AMI.
The following anatomical nomenclatures were used: retrosternal, precordial, right and left upper limb, epigastric, neck and mandible [11]. Upper limb included the pain localized in the upper limb girdle, shoulder with its anterior and dorsal surfaces, arm, cubital region, forearm, carpal region, or hand.
Ineligibility criteria
The following criteria were considered for patients ineligibility: absence of cardiac pain; myocardial infarction with non-obstructive coronary arteries (MINOCA) [1]; failure to define the artery responsible for the AMI in the coronary angiography, such as significant obstructive stenotic lesions in several arteries; absence of CMR (patients who for some reason did not undergo the examination); absence of LV myocardial necrosis/fibrosis or late enhancement patterns of non-coronary origin on CMR, such as: cardiomyopathy or myocarditis.
Statistical analysis
Data were presented as median and mean ± standard deviation for continuous variables and in absolute frequencies and percentages for categorical variables. To test the degree of association between the categorical variables, the Chi-square test or Fisher’s exact test was used. Statistical significance was established by P value < 0.05 in SPSS analysis.
| Results | ▴Top |
During the period from May 2015 to March 2020, a total of 328 patients with STEMI were included in the BATTLE-AMI [9] study. This analysis was performed from the database of these patients. Among them, 105 (32%) were considered ineligible for the study (Fig. 1).
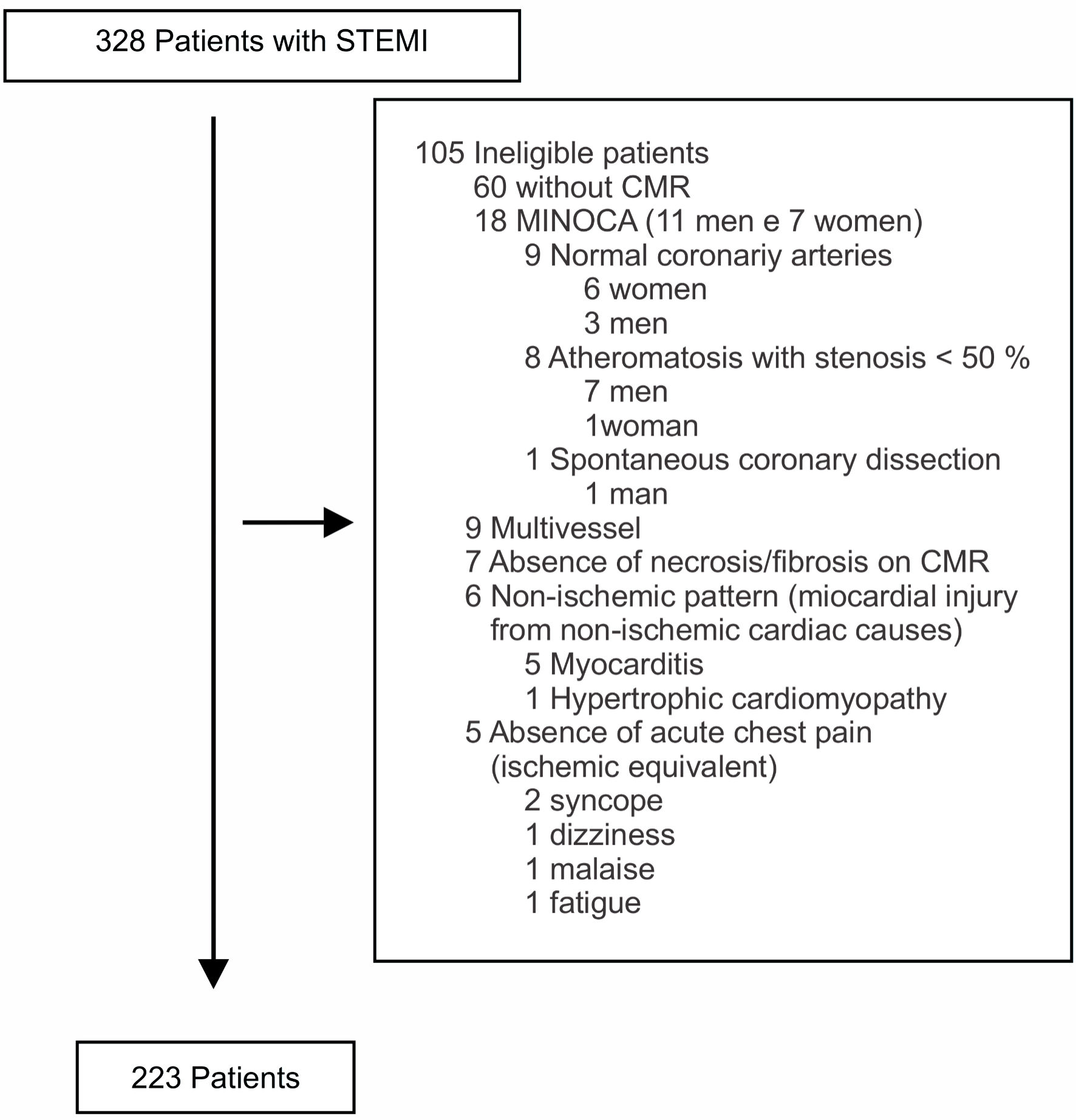 Click for large image | Figure 1. Distribution of causes of ineligibility for the study. STEMI: ST-segment elevation myocardial infarction; CMR: cardiac magnetic resonance; MINOCA: myocardial infarction with non-obstructive coronary arteries. |
Therefore, 223 consecutive patients (68%) aged between 35 and 74 years (57.3 ± 8.2 years) were included and most of them were male (72.2%). One hundred twenty-four (55.6%) participants had systemic arterial hypertension and 67 (30.0%) had diabetes mellitus. The mean value of high-sensitivity cardiac troponin was 7,244.84 ± 5,852.58 pg/mL (upper reference limit: 14 pg/mL) (Table 1).
 Click to view | Table 1. Baseline Characteristics of the Study Participants |
Table 2 shows the location and irradiation of pain.
Click to view | Table 2. Absolute and Relative Frequencies of Pain Site and Irradiation of Patients Evaluated in the Study |
Patients employed 21 adjectives to describe the quality of pain that they felt. Between the most common descriptions, it was observed that 93 (41.7%) participants classified the pain as tightness, 50 (22.4%) patients as burning and 15 (6.6%) as twinge.
The analysis of angiographic data allowed us to determine the absolute and relative frequencies of the arteries responsible for STEMI: RCA in 88 patients (39.5%), LCX artery in 25 (11.2%) and LAD artery in 110 (49.3%).
Tables 3 and 4 present the association between the pain sites and irradiations with the culprit artery, according to the angiographic and semiological data. No significant differences were observed between the arteries in terms of pain site (likelihood ratio Chi-square test, P = 0.237) and irradiation (likelihood ratio Chi-square test, P = 0.473).
Click to view | Table 3. Absolute and Relative Frequencies of Pain Sites According to the Culprit Arteries |
Click to view | Table 4. Distribution of Arterial Territories According to Pain Irradiation |
There were no significant differences among gender (P = 0.828), age (P = 0.966), systemic arterial hypertension (P = 0.666) and diabetes mellitus (P = 0.685) in relation to the pain site.
Figure 2 shows three different patients (A, B and C) who described their pain in the same location: the retrosternal region. However, these patients did not share the same STEMI culprit artery. In patient A it was found the RCA, in B was the LCX artery and in C was LAD artery.
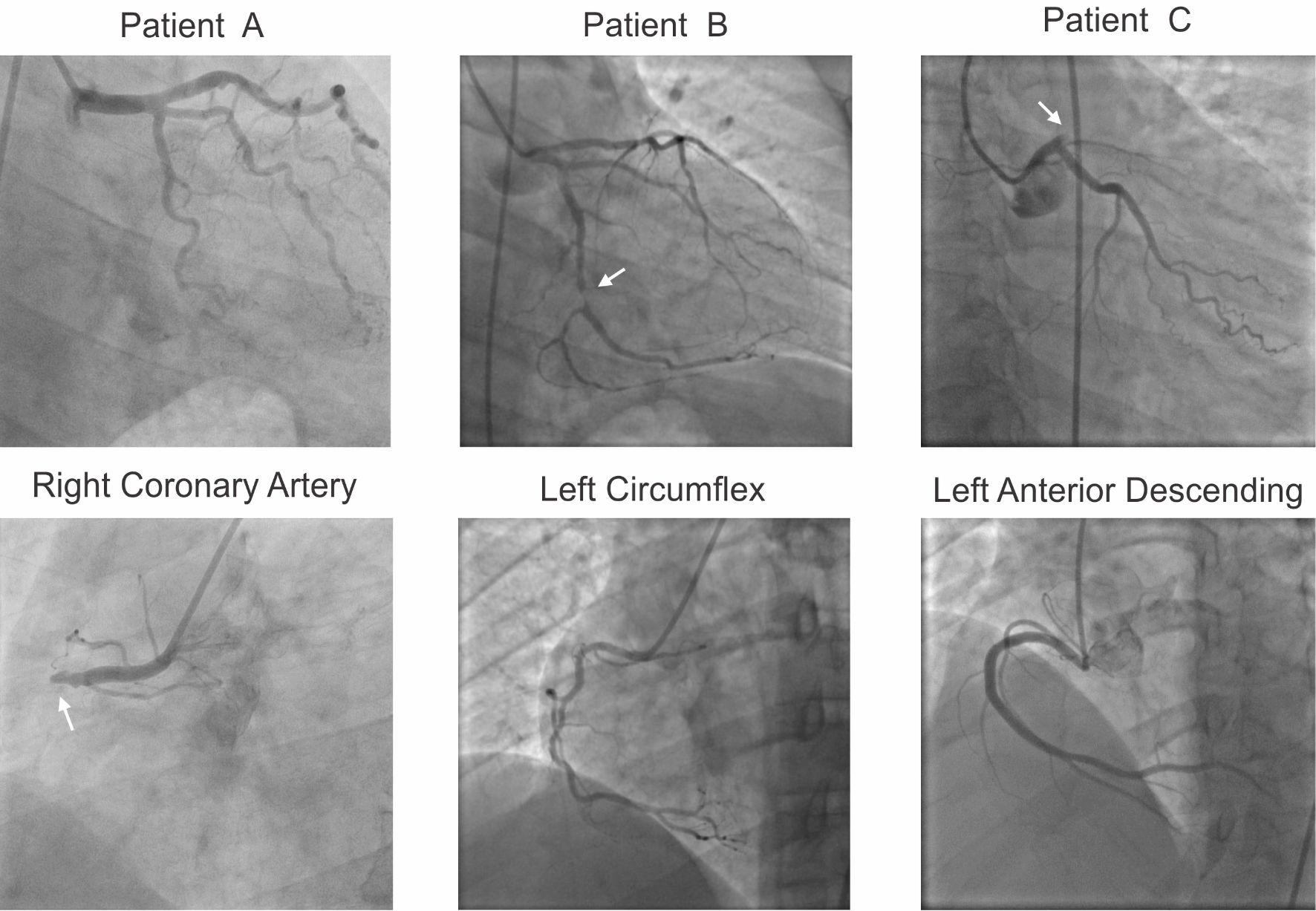 Click for large image | Figure 2. Acute retrosternal pain and culprit coronary artery for STEMI. Three patients (A, B and C) with the same retrosternal location of pain and different obstructed coronary arteries (arrows). STEMI: ST-segment elevation myocardial infarction. |
Table 5 shows the LV fibrotic segments evaluated according to the pain site. No significant differences were observed in pain sites in relation to segments in the basal short axis, short apical axis, and long axis. In the short mid axis, the only exception was the mid inferior segment (segment 10), in which there was a significant difference between the locations.
Click to view | Table 5. Absolute and Relative Frequencies of Fibrotic Segments According to Pain Sites and Axis Evaluated on Cardiac Magnetic Resonance |
| Discussion | ▴Top |
In our study, it was not observed the association between the localization and irradiation of the cardiac pain in STEMI and the culprit coronary artery or the 17 injured LV myocardial segments. Our results add knowledge on the subject because they showed that these characteristics of chest pain should not be used in the algorithms of the management of patients with STEMI.
Pain is the most frequent clinical manifestation in AMI, and according to Panju et al [12], three-quarters of all patients with recognized AMI have chest pain. In the initial sample of patients evaluated in the BATTLE-AMI [9] study, chest pain was reported for 323 of the individuals (98.4%).
The definition of pain adopted in the BATTLE-AMI [9] project was used, stating that: “Pain can be seen as a multidimensional phenomenon that involves physiological, sensory, affective, cognitive, behavioral and sociocultural aspects.” It is worth remembering that pain: “can be influenced by memory, expectations and emotions, in addition to factors such as: socioeconomic conditions, thoughts, cultural context, vital signs, medical-surgical history, coping strategies, among other aspects” [9], including the assistant physician.
Christie et al [13] already called attention to the clinician to carry out a spontaneous but not a directed anamnesis, with the aim of allowing the patient to describe his pain as it was felt. This could reduce the influence of the assistant physician’s interpretation on the description of the patient’s pain.
In 1973, Macruz el at [3] evaluated the importance of cardiac pain characteristics, such as location, quality, and irradiation, described by 151 patients with acute and chronic coronary insufficiency, to determine the location of coronary obstruction. In our study, we decided to reassess this information only in individuals with STEMI, as well as to evaluate the association between cardiac pain and the injured myocardial segments, with the anatomical refinement obtained through the CMR.
Location of pain
Christie et al [13] stated that: “To dispel an old myth, chest pain with reference to the left arm is in no way pathognomonic of cardiac pain and may arise from aggression from other organs. In addition, cardiac pain is not referred to the arm in approximately 50% of cases.” In our findings, pain in left upper limb alone occurred in only 15 (6.7%) participants and associated with right upper limb in three of the patients (1.3%).
Berger et al [14] drew attention to the fact that: “A more in-depth analysis of cardiac chest pain, in terms of right and left distribution, revealed that the left side of the chest and the left arm are, in fact, more frequent than in the right arm.”
Everts et al [15] analyzed 903 consecutive patients hospitalized for AMI and concluded that pain in the right upper quadrant of the chest or both arms was more frequently reported in patients who were confirmed with AMI. However, in both AMI and non-AMI cases, the location of chest pain was of limited use to predict which patients would eventually have AMI.
In our analysis, there was a clear predominance of pain in the thoracic region. It was described by 175 individuals (78.5%), being retrosternal in 90 (40.4%) patients and precordial in 85 (38.1%). Such data confirmed the reports by Macruz et al [3] about the location of pain that precordial or retrosternal sites corresponded to 68% of the painful manifestations. For Braunwald et al [6], the predominant location was retrosternal.
Irradiation of pain
According to Berger et al [14], when analyzing the irradiation of chest pain: “Pain with wide irradiation involving the right arm strongly suggests that an AMI is evolving. Thus, pain irradiation to right arm, although less frequent (41%) is more specific (94%). While irradiation to the left arm is more frequent (55%) and less specific (76%).”
Panju et al [12] wrote that: “Among the most powerful resources that increase the probability of diagnosis of AMI is chest pain radiating to both arms simultaneously (seven times), right shoulder (three times) and left arm (two times)”. These data were also corroborated by McConaghy et al [16].
Braunwald et al [6] reported that cardiac pain in STEMI spreads to both sides of the anterior chest wall, irradiating to the ulnar aspect of the left arm. According to the same authors, “Irradiation of pain from the chest to the neck and mandible is typical of myocardial infarction.” Our data showed that irradiation for left upper limb alone occurred in the most of patients (27.8%) and that radiation to the neck and mandible had low prevalence and was present in only seven patients (3.1%). Pain without irradiation occurred in 79 of our patients (35.4%).
Pain quality
In our analysis of the adjectives reported by patients to express the quality of pain in STEMI, findings like those described by other authors [6] were observed. The most frequent adjectives reported in our study were: tightness, burning, and twinge.
Location of pain and culprit artery
Although cardiac chest pain was frequent in our patients, it was not able to indicate with statistical significance an association between its location and the artery responsible for the STEMI.
Macruz et al [3] did not identify an association between the arteries responsible for the event and the region where the pain was located. These authors reported that in the RCA occlusion, four patients described pain in the precordial region, one in the retrosternal region, one in the forearms and none in the epigastric. In our analysis of 38 patient with isolated obstruction in RCA, LCX or LAD arteries, only one of them referred to the epigastric location and in this situation, the culprit artery was the LAD.
Irradiation of pain and culprit artery
According to Macruz et al [3], “Cardiac pain secondary to left anterior descending artery obstruction determines no irradiation or irradiation to the internal surface of the left arm.” In our data, it was found that the pain without radiation did not determine the culprit artery, and this occurred in our patients with distribution as follows: 35 (31.8%) in the involvement of the LAD, 12 (48%) for LCX and 32 (36.4%) for RCA, without statistical significance.
In our analyses, the irradiation to left upper limb was described by the patients when the LAD artery was the culprit artery in 33 patients (30%), LCX in four (16%) and RCA in 25 (28.4%). It was not possible to confirm the associations described by Macruz et al [3], because irradiation to the left upper limb or any other region was not related to the artery responsible for AMI.
Another conclusion reported by these authors [3] stated that RCA obstruction causes pain with right or bilateral irradiation to the upper limbs and higher regions (cervical and mandibular) and right hemithorax. Our data did not corroborate these statements; irradiation to right upper limb occurred in RCA lesions in four of the patients (4.5%), LCX in zero (0%) and LAD in three of the individuals (2.7%), without statistical significance. The same result occurred in the irradiation to both upper limbs; our data revealed that there was no statistical significance, with LAD occlusion in 10 cases (9.1%), RCA in seven (8%) and LCX in four (16%).
According to Macruz et al [3], in the analysis of obstruction in the LCX, in the presence of dominant RCA, the irradiation was to the left region, upper limbs and higher regions; the irradiation was bilateral when LCX was dominant. In our data, this association was also not statistically significant.
Our data did not show an association between the localization and irradiation of the cardiac pain and the artery responsible for the STEMI. Therefore, the anamnesis should primarily emphasize the time of onset of the chest pain for the management of the STEMI according to the current guidelines [7, 8], and not its exact location or irradiation.
Location of pain and segment of injured LV myocardium
To the best of our knowledge, this study is the first to evaluate the possibility of an association between acute chest pain or pain in adjacent regions and the 17 injured LV myocardium segments in STEMI, identified through CMR.
In the analysis between pain sites and LV fibrotic myocardial segments, there were no significant differences in relation to the basal short axis, apical short and long axis. However, this difference was observed to the mid inferior segment (segment 10). The data were not considered clinically relevant because this association was observed in only one of 17 segments after multiple comparisons.
We recognize that our study has some limitations: 1) The small sample size of our study; 2) The size of the infarcted area may have varied as a function of the times for reperfusion after thrombolytic and/or mechanical recanalization, as well as the presence of collateral circulation; 3) It was not possible to rule out possible interobserver bias in the initial collection of anamnesis data referring to pain.
Conclusions
In this series of patients with STEMI, no associations were observed between the location or irradiation of acute chest pain and/or adjacent areas and the culprit artery, or between pain and segmental myocardial fibrosis in the left ventricle.
Acknowledgments
We are grateful to all the patients who participated in the BATTLE-AMI study, and in a distinct way, to Professor Jose Antonio Franchini Ramires, for his suggestions and review of this article.
Financial Disclosure
The authors did not receive support from any organization for the submitted work.
Conflict of Interest
The authors declare that they have no conflict of interests.
Informed Consent
All participants or their representatives signed an informed consent form.
Author Contributions
Weverton Ferreira Leite: concept of the study, data collection and tabulation, statistical analysis, writing, review and editing. Rui Manuel dos Santos Povoa, MD, PhD, suggestions, and text review. Adriano Mendes Caixeta, MD, PhD, suggestions and reviews of coronary angiography images and text. Celso Amodeo, MD, PhD, suggestions, text review and translation: Portuguese into English. Gilberto Szarf, MD, PhD, review of text and images of CMR imaging. Maria Teresa Nogueira Bombig, MD, PhD, suggestions, and text review. Maria Cristina Oliveira Izar, MD, PhD, suggestions and text review. Luciana Netto Gioia, MD, data collection and tabulation. Wilma Noia Ribeiro, MD, PhD, suggestions, text review and translation: Portuguese into English. Francisco Antonio Helfenstein Fonseca, MD, PhD, concept of the study, statistical analysis, suggestions, and text review.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Nicolau JC, Feitosa Filho GS, Petriz JL, Furtado RHM, Precoma DB, Lemke W, Lopes RD, et al. Brazilian society of cardiology guidelines on unstable angina and acute myocardial infarction without ST-segment elevation - 2021. Arq Bras Cardiol. 2021;117(1):181-264.
doi pubmed pmc - G. B. D. Mortality, Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117-171.
doi pubmed pmc - Macruz R, Toriano N, Carvalho VB, Arie S, Marrara JP, Tranchesi J, Pileggi F, et al. Dor cardiaca, valor de sua caracterizacao para a localizacao da obstrucao coronaria. Arq Bras Cardiol. 1973;26:525-549
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, Blankstein R, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22):e368-e454.
doi - Leite WF. Analise comparativa entre a proteina C-reativa de alta sensibilidade em veia periferica e seio coronario na angina estavel e instavel. [thesis]. Sao Paulo: Faculdade de Medicina. 2014. Cited on Sep 24, 2022. Available from: http://www.teses.usp.br/teses/disponiveis/5/5131/tde-26022015-152337.
- Zipes DP, Libby P, Bonow RO, Braunwald E. Braunwald, Tratado de Doencas Cardiovasculares. Translation of the original in English. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 7th ed. Elsevier. 2006; p. 66-68, 1129 e 1155.
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119-177.
doi - Writing Committee Members, Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(2):e21-e129.
doi - Fonseca FAH, Izar MC, Maugeri IML, Berwanger O, Damiani LP, Pinto IM, Szarf G, et al. Effects of four antiplatelet/statin combined strategies on immune and inflammatory responses in patients with acute myocardial infarction undergoing pharmacoinvasive strategy: Design and rationale of the B and T Types of Lymphocytes Evaluation in Acute Myocardial Infarction (BATTLE-AMI) study: study protocol for a randomized controlled trial. Trials. 2017;18(1):601.
doi pubmed pmc - Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, Pennell DJ, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002;105(4):539-542.
doi - Paulsen F, Sobotta WJ. Atlas de anatomia humana: Anatomia Geral e Sistema muscular, 23rd ed. Rio de Janeiro: Guanabara Koogan Ltda editora. 2015;1:e3.
- Panju AA, Hemmelgarn BR, Guyatt GH, Simel DL. The rational clinical examination. Is this patient having a myocardial infarction? JAMA. 1998;280(14):1256-1263.
doi - Christie LG, Jr., Conti CR. Systematic approach to evaluation of angina-like chest pain: pathophysiology and clinical testing with emphasis on objective documentation of myocardial ischemia. Am Heart J. 1981;102(5):897-912.
doi - Berger JP, Buclin T, Haller E, Van Melle G, Yersin B. Right arm involvement and pain extension can help to differentiate coronary diseases from chest pain of other origin: a prospective emergency ward study of 278 consecutive patients admitted for chest pain. J Intern Med. 1990;227(3):165-172.
doi - Everts B, Karlson BW, Wahrborg P, Hedner T, Herlitz J. Localization of pain in suspected acute myocardial infarction in relation to final diagnosis, age and sex, and site and type of infarction. Heart Lung. 1996;25(6):430-437.
doi - McConaghy JR, Oza RS. Outpatient diagnosis of acute chest pain in adults. Am Fam Physician. 2013;87(3):177-182
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.