

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 14, Number 3, June 2023, pages 221-227

Coronary Artery Disease as an Independent Predictor of Cardiovascular Mortality in COVID-19 Patients
Hywel Soneya, d, Nathan DeRon Jra, Lucas Wanga, Lawrence Hoanga, Mujahed Abualfoula, Yi Zhaoa, Kristopher Atena, Victor Canelaa, Sri Prathivadab, Michael Vua, Manavjot Sidhub, c
aDepartment of Internal Medicine, Methodist Dallas Medical Center, Dallas, TX, USA
bMethodist Dallas Cardiovascular Consultants, Methodist Medical Group, Dallas, TX, USA
cDivision of Cardiology, Methodist Dallas Medical Center, Dallas, TX, USA
dCorresponding Author: Hywel Soney, Department of Internal Medicine, Methodist Dallas Medical Center, Dallas, TX 75203, USA
Manuscript submitted January 22, 2023, accepted February 24, 2023, published online May 26, 2023
Short title: COVID-19 CAD Patient Outcomes
doi: https://doi.org/10.14740/cr1471
| Abstract | ▴Top |
Background: Coronavirus disease 2019 (COVID-19) is associated with increased risk of cardiovascular mortality. However, little is known about the combined effect of coronary artery disease (CAD) and COVID-19 on mortality. We aimed to investigate the incidence of cardiovascular and all-cause mortality in COVID-19 patients with CAD.
Methods: This multicenter retrospective study identified 3,336 COVID-19 patients admitted between March and December 2020. Data points were manually reviewed in the patients’ electronic health records. Multivariate logistic regression was used to assess whether CAD and its subtypes were associated with mortality.
Results: This study shows that CAD was not an independent predictor of all-cause mortality (odds ratio (OR): 1.512, 95% confidence interval (CI): 0.1529 - 14.95, P = 0.723). However, there was a significant increase in cardiovascular mortality in patients with CAD compared to those without (OR: 6.89, 95% CI: 2.706 - 17.53, P < 0.001). There was no significant difference in all-cause mortality in patients with left main artery and left anterior descending artery disease (OR: 1.29, 95% CI: 0.80 - 2.08, P = 0.29). However, CAD patients with a history of interventions (e.g., coronary stenting or coronary artery bypass graft) showed increased mortality compared to those solely treated by medical management (OR: 1.93, 95% CI: 1.12 - 3.33, P = 0.017).
Conclusions: CAD is associated with a higher incidence of cardiovascular mortality but not all-cause mortality in COVID-19 patients. Overall, this study will help clinicians identify characteristics of COVID-19 patients with increased risk of mortality in the setting of CAD.
Keywords: Coronary artery disease; Cardiovascular mortality; COVID-19; Coronary intervention; Medical management
| Introduction | ▴Top |
Cardiovascular disease remains the leading cause of mortality in the world [1] and is associated with a significant increase in morbidity and mortality in hospitalized patients with coronavirus disease 2019 (COVID-19) [2]. Several studies have shown that COVID-19 is associated with myocardial injury [3-5], development of new arrhythmias [6], and elevated incidence of cardiovascular events during hospitalization [7]. Coronary artery disease (CAD), the most common form of cardiovascular disease, is a known risk factor for mortality in COVID-19-infected patients [8, 9]. Studies have also shown that COVID-19 patients with a history of CAD are associated with higher incidence of intensive care unit admission, need for mechanical ventilation, and cardiovascular complications [10-12]. Recent literature suggests that COVID-19 may cause cardiac vasculature calcification remodeling, subsequently predisposing patients to future ischemic events [13], endothelial dysfunction [14], or a proinflammatory state directly leading to myocardial injury [15]. Recognizing the impact of CAD on COVID-19 progression and recovery has the potential to guide specific intervention strategies, impact prognosis, and prevent future COVID-19-related deaths due to cardiovascular disease. In this study, we aimed to explore whether CAD confers a higher risk for mortality in COVID-19 patients. Our objectives were to determine if CAD significantly increases the risk of all-cause and/or cardiovascular mortality in hospitalized COVID-19 patients and to determine if atherosclerosis in a patient’s cardiac anatomy is also associated with increased risk of mortality.
| Materials and Methods | ▴Top |
This multicenter retrospective cohort study included 3,336 unvaccinated adults (≥ 18 years of age) with PCR-confirmed COVID-19 admitted into four hospitals within the Methodist Health System in Dallas, Texas from March 2020 to December 2020. Patient data were abstracted from the electronic medical records. All hospitalized patients who tested PCR-positive for COVID-19 regardless of reason for admission were included (Fig. 1). All patient data were de-identified before analysis, and the study was approved by WCG/Aspire IRB (IRB#: 20201424). The study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration.
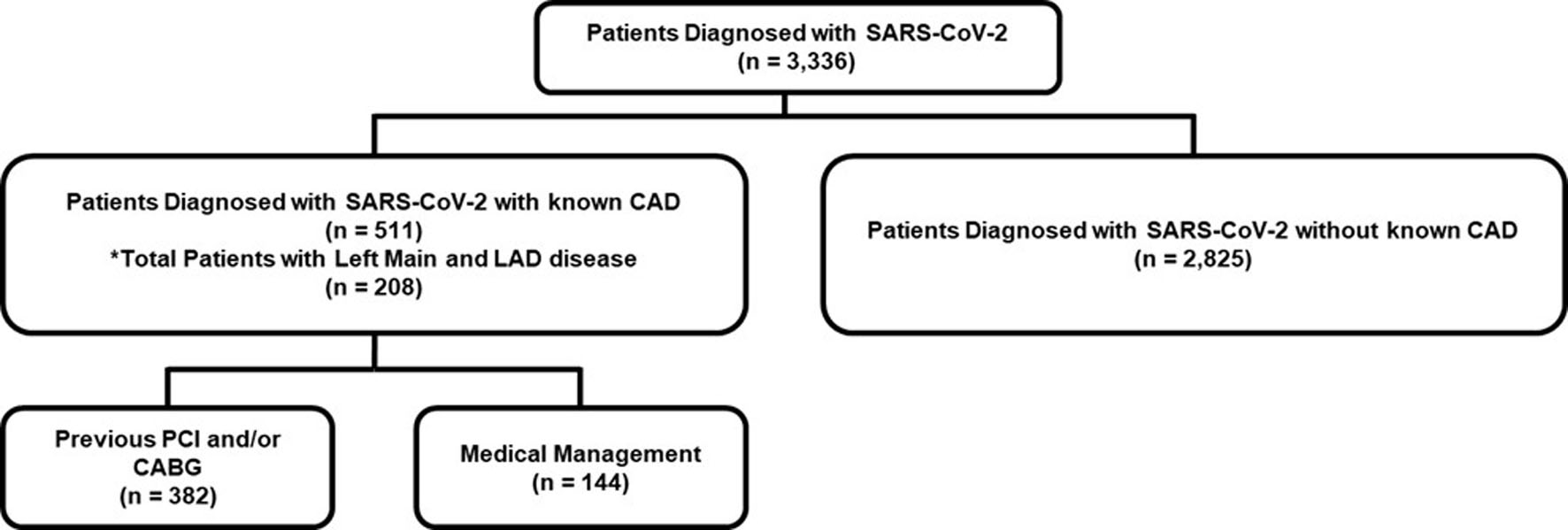 Click for large image | Figure 1. Flow chart of the study’s patient population. CAD: coronary artery disease; LAD: left anterior descending; PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft; SARS-CoV-2: severe acute respiratory syndrome coronavirus 2. |
Data manually collected included baseline demographics, symptoms and vital signs on arrival, comorbidities (e.g., history of congestive heart failure, stroke, diabetes, hypertension, chronic obstructive pulmonary disease (COPD), asthma, chronic kidney disease (CKD), end-stage renal disease (ESRD), hepatic cirrhosis, and human immunodeficiency virus (HIV)), laboratory measurements, inpatient medications, and outcomes (i.e., mortality and major adverse cardiovascular event). Patients were deemed to have a diagnosis of CAD if there was history of a coronary angiography demonstrating stenosis, ST-elevation myocardial infarction (STEMI), non-ST-elevated myocardial infarction (NSTEMI), percutaneous coronary intervention (PCI), or coronary artery bypass grafting (CABG). When applicable, left main artery and left anterior descending (LAD) artery disease was also delineated. CAD patients who had acute coronary syndrome (ACS) in addition to COVID infection were also identified. CAD patients with ACS were then divided into two subcategories: 1) those who only received medical management for ACS; and 2) those who had interventional management (i.e., PCI and/or CABG) for ACS. Mortality was defined as either in-hospital death or discharge to hospice. Cardiovascular mortality was differentiated from non-cardiovascular mortality if the discharge paperwork or death note reported cause of death related to stroke, pulmonary embolism (PE), cardiogenic shock, arrhythmias, STEMI, or a non-STEMI.
Continuous variables were characterized by mean and standard deviation or median and interquartile range depending on whether they were normally distributed. For multiple means or medians, one-way analysis of variance (ANOVA) and/or Kruskal-Wallis’s test was used based on normality. A P-value ≤ 0.05 was considered significant. Multivariate logistic regression was used to assess whether CAD was independently associated with increased incidence of mortality. Multinomial logistic regression was used to assess whether CAD was independently associated with increased incidence of cardiovascular mortality. Regression was constructed to adjust for comorbidities and demographics as noted in baseline data for each analysis subset. The base regression only included variables with data available for > 90% of patients. The subsets included patients with the four subcategories of CAD and left main artery and LAD artery disease compared to non-left main artery and LAD artery disease. We did not perform imputation for missing laboratory values as they were likely non-random. Statistical analysis was performed in R version 4.1.2 using the EZR package version 1.55.
| Results | ▴Top |
Among 3,336 patients with COVID-19, 511 (15.3%) had CAD and 2,825 (84.7%) did not. In patients with CAD, there were proportionally more male patients than female (60.9% vs. 39.1%, P < 0.001), and the median age for patients without CAD was lower than for those with CAD (61 (48 - 80) vs. 71 (63 - 80) years, P < 0.001). Patients with CAD also had a higher prevalence of CKD (26.4% vs. 12.1%, P < 0.001), COPD/asthma (20.5% vs. 13.0%, P < 0.001), diabetes (59.3% vs. 36.2%, P < 0.001), heart failure (36.3% vs. 9.2%, P < 0.001), hypertension (82.8% vs. 58.6%, P < 0.001), and history of stroke (16.2% vs. 7.9%, P < 0.001). Prior intervention with PCI and/or CABG and prevalence of left main and LAD artery disease was also assessed. Of 511 patients with CAD and COVID, 247 (50.7%) had prior PCI and 135 (27.7%) had a prior CABG. Also, 208 patients (42.7%) had known left main and LAD artery disease (Table 1).
 Click to view | Table 1. Demographics of Study Cohort |
In our cohort, there was greater incidence of all-cause mortality in CAD patients, patients with left main and LAD artery disease, and also patients who were on interventional management compared to patients without CAD and those solely on medical management (Fig. 2). However, after adjusting for confounding variables, the adjusted odds ratio (OR) of all-cause mortality of CAD patients was not significantly higher than that of non-CAD patients (OR: 1.512, 95% confidence interval (CI): 0.1529 - 14.95, P = 0.723) (Table 2). Furthermore, adjusted odds of all-cause mortality in patients with CAD specific to the left main and LAD artery disease was not significantly higher than CAD patients without left main and LAD artery disease (OR: 1.29, 95% CI: 0.80 - 2.08, P = 0.29). Amongst evaluation of risk factors, age demonstrated significantly higher adjusted odds of all-cause mortality while obesity and other comorbidities were not significant for all-cause mortality (Table 2). Lastly, when comparing patients who were solely on medical management to those on interventional management, the medical management group had a lower likelihood of adjusted all-cause mortality than those on interventional management (OR: 1.93, 95% CI: 1.12 - 3.33, P = 0.017).
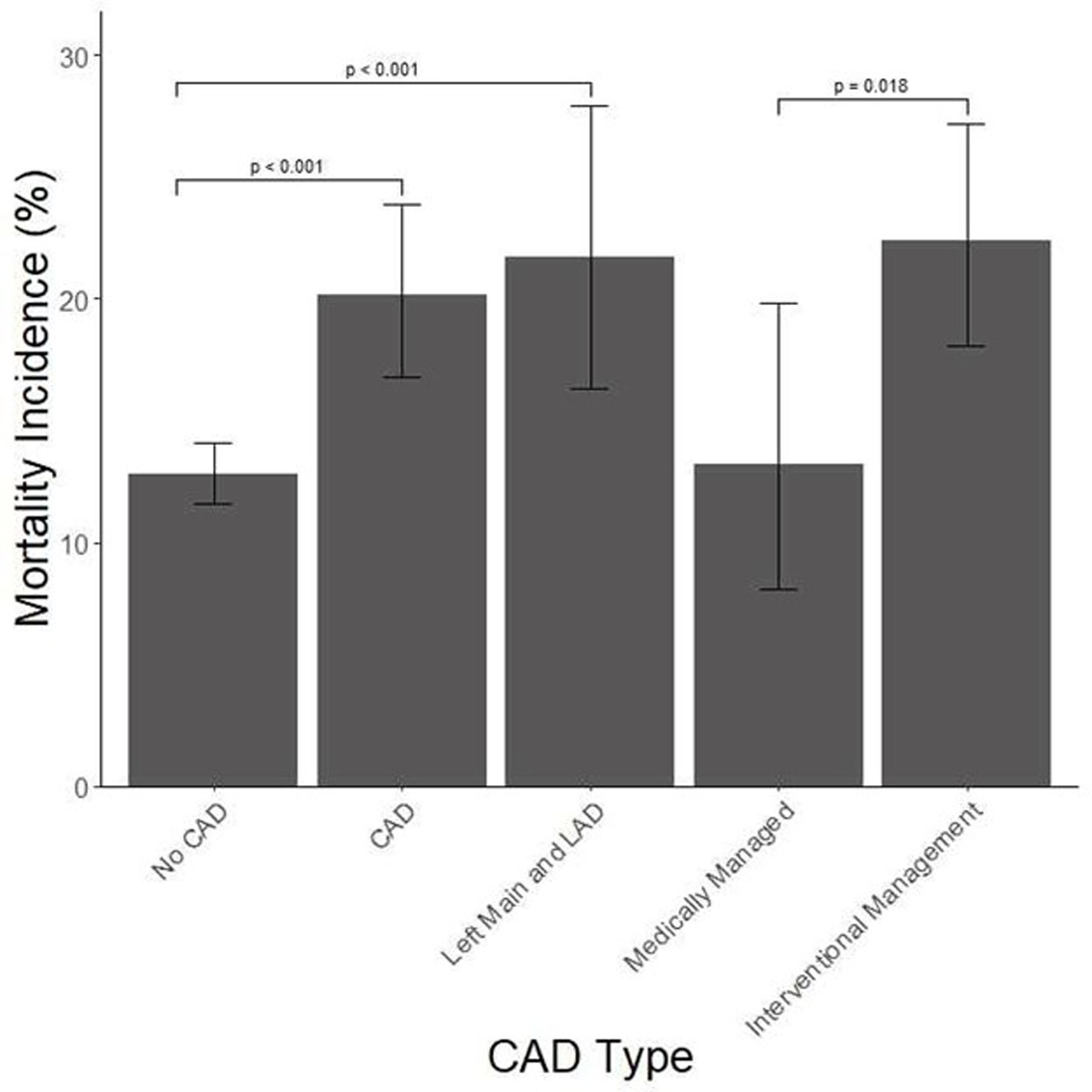 Click for large image | Figure 2. All-cause mortality incidence by coronary artery disease classification. Bars illustrate mean ± SD. CAD: coronary artery disease; LAD: left anterior descending; SD: standard deviation. |
Click to view | Table 2. Logistic Regression Analysis of Coronary Artery Disease and Incidence of All-Cause Mortality |
Incidence of cardiovascular mortality was higher in patients with CAD and in patients with left main and LAD artery disease than those without CAD (Fig. 3). After adjusting for confounding variables, there was a significant increase in cardiovascular mortality in CAD patients compared to non-CAD patients (OR: 6.89, 95% CI: 2.706 - 17.53, P < 0.001) (Table 3). STEMI and cardiogenic shock represented the most common causes of cardiovascular mortality, while other cardiovascular causes, including endocarditis, supraventricular tachycardia, and ventricular tachycardia did not have enough event rates to assess significance (Table 4). Similar to the adjusted all-cause mortality analysis, there was no difference in cardiovascular mortality in CAD patients with left main artery disease and LAD artery disease compared to those without (OR: 1.44, 95% CI: 0.413 - 5.01, P = 0.568). While age demonstrated significant all-cause mortality, it did not demonstrate significance in cardiovascular mortality; however, obesity did demonstrate significant adjusted cardiovascular mortality (Table 3). Unlike the all-cause mortality analysis, CAD patients with history of interventional management did not have higher odds of cardiovascular mortality compared to those with sole medical management (OR: 1.49, 95% CI: 0.294 - 7.58, P = 0.63).
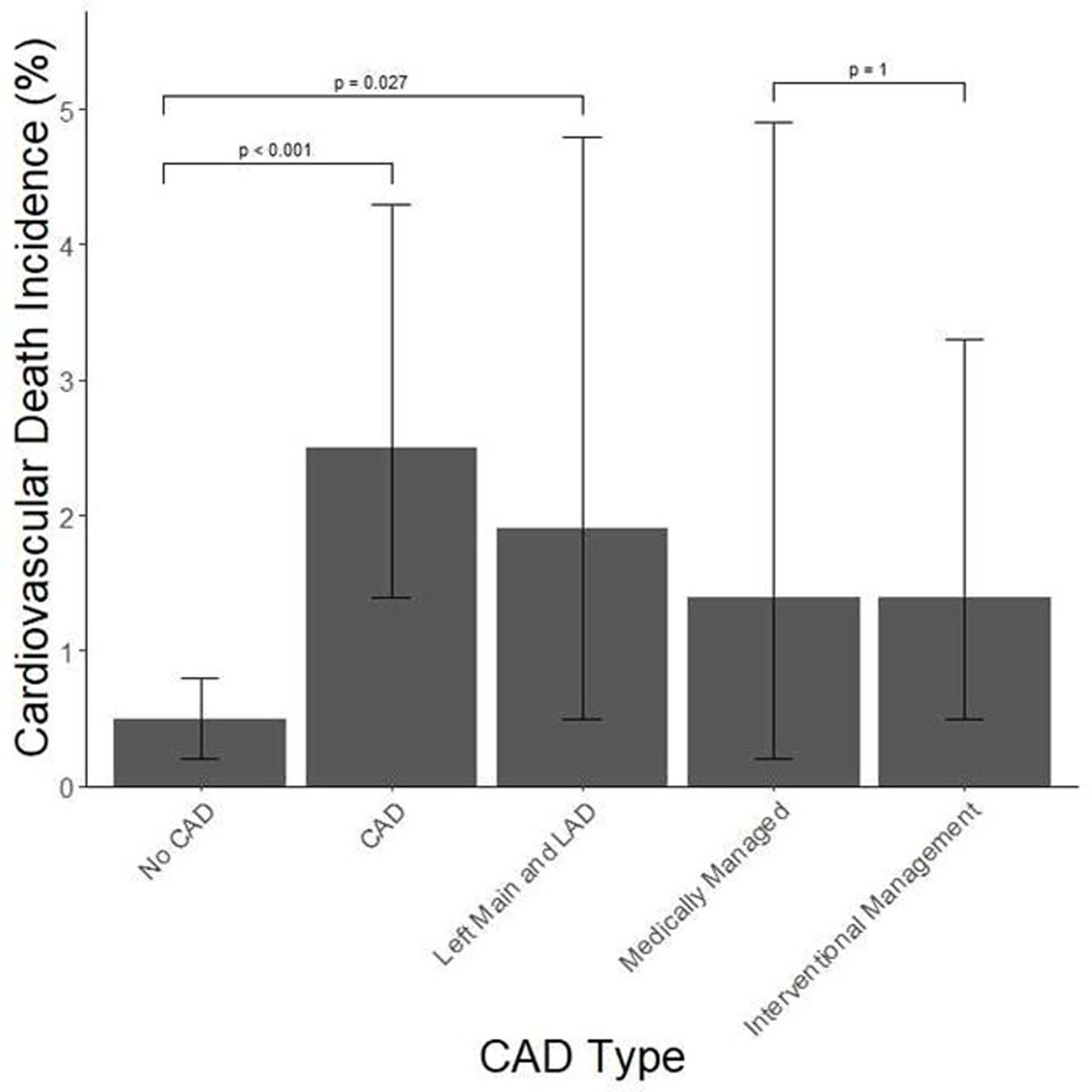 Click for large image | Figure 3. Cardiovascular mortality incidence by coronary artery disease classification. Bars illustrate mean ± SD. CAD: coronary artery disease; LAD: left anterior descending; SD: standard deviation. |
Click to view | Table 3. Logistic Regression for Coronary Artery Disease and Incidence of Cardiovascular Mortality |
Click to view | Table 4. Distribution of Cardiovascular Causes of Mortality |
| Discussion | ▴Top |
We analyzed the outcomes of patients hospitalized with COVID-19 across four hospitals in Dallas, Texas. Here, we demonstrated that CAD was an individual predictor for cardiovascular mortality but not all-cause mortality. We also found that CAD patients who were managed medically were at a significantly lower risk of all-cause mortality compared to CAD patients who were managed with PCI or CABG. Furthermore, left main and LAD artery disease did not increase the risk of mortality in COVID-19 patients.
To our knowledge, this is the first study involving a large cohort of patients to address the effect of CAD in patients hospitalized with COVID-19. Prior studies investigating the association between CAD and COVID-19 suggested the presence of increased mortality in COVID-19 patients with CAD; however, cause of mortality, anatomy of CAD, and types of intervention were not assessed [8]. Guo et al reported similar findings to our study among 187 patients in Wuhan, China, but emphasized the presence of worse outcomes in patients with myocardial injury regardless of cardiovascular disease history [4].
The strengths unique to this study include: 1) a large diverse COVID-19 patient population with known CAD across four different hospitals; 2) a comprehensive validation of data with a thorough chart review of each individual parameter; 3) a direct comparison of all-cause and cardiovascular mortality in the same patient population with a focused comparison based on cardiac anatomy and treatment history; and 4) patient data from a unique point in the history of COVID-19 when all patients were unimmunized because the vaccine was not yet widely distributed.
This study has limitations. The time period that the study encompassed represented an early period in the COVID-19 pandemic in the United States. Since then, a vast amount of knowledge about the disease has been distilled and interventions implemented. The advent of the vaccine has profoundly impacted both infection rate and hospitalization outcomes, which we were not able to evaluate in this study. Not all patients classified as having CAD had a cardiac catheterization report, which impeded our group from quantifying the amount of CAD for each patient. The existence of clinically insignificant undiagnosed CAD may confound our analysis. This study was also limited to data collected from patients admitted to the hospital and hence, the analysis applies only to hospitalized patients diagnosed with COVID-19. We also demonstrate that solely medically managed CAD patients show significantly less risk of mortality compared to patients managed with PCI or CABG. This finding can be explained by the difference in severity of CAD among each of these populations as patients who are solely medically managed likely have less significant CAD burden than patients undergoing PCI or CABG who likely have more pronounced multivessel disease.
In summary, we showed that CAD is associated with increased likelihood of cardiovascular mortality but not all-cause mortality. We also showed that CAD patients who were managed medically were at lower risk of mortality than patients who were managed with either PCI or CABG. Furthermore, likelihood of mortality did not differ when comparing the presence or absence of left main and LAD artery disease. We propose that the results of this study will help clinicians better understand and treat hospitalized COVID-19 patients with a history of CAD. By identifying key characteristics, physicians can better predict outcomes such as mortality to be better prepared to best manage and anticipate complications associated with this disease.
Acknowledgments
The authors thank Anne Murray, PhD, MWC® of the Clinical Research Institute at Methodist Health System for providing editorial support.
Financial Disclosure
The authors report no financial relationships regarding the content herein.
Conflict of Interest
The authors report no conflict of interest regarding the content herein.
Informed Consent
Not applicable.
Author Contributions
Hywel Soney and Nathan DeRon: conceptualization, methodology, investigation, resources, writing - original draft, writing - review and editing, and visualization. Lucas Wang: conceptualization, methodology, investigation, resources, data curation, writing - review and editing, supervision, and project administration. Lawrence Hoang: methodology, validation, formal analysis, investigation, resources, data curation, and visualization. Mujahed Abualfoul and Yi Zhao: conceptualization and investigation. Kristopher Aten, Victor Canela, Sri Prathivada, and Michael Vu: investigation. Manavjot Sidhu: conceptualization, supervision, and project administration.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
ACS: acute coronary syndrome; BMI: body mass index; CABG: coronary artery bypass grafting; CAD: coronary artery disease; CKD: chronic kidney disease; COPD: chronic obstructive pulmonary disease; ESRD: end-stage renal disease; HIV: human immunodeficiency virus; LAD: left anterior descending; PCI: percutaneous coronary intervention; PE: pulmonary embolism; STEMI: ST-elevation myocardial infarction
| References | ▴Top |
- World Health Organization. The top 10 causes of death. World Health Organization. 2020. Retrieved July 3, 2022, from https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
- Ko JY, Danielson ML, Town M, Derado G, Greenlund KJ, Kirley PD, Alden NB, et al. Risk factors for coronavirus disease 2019 (COVID-19)-associated hospitalization: COVID-19-associated hospitalization surveillance network and behavioral risk factor surveillance system. Clin Infect Dis. 2021;72(11):e695-e703.
doi pubmed pmc - Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239-1242.
doi pubmed - Guo T, Fan Y, Chen M, Wu X, Zhang L, He T, Wang H, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(7):811-818.
doi pubmed pmc - Bienvenu LA, Noonan J, Wang X, Peter K. Higher mortality of COVID-19 in males: sex differences in immune response and cardiovascular comorbidities. Cardiovasc Res. 2020;116(14):2197-2206.
doi pubmed pmc - Dewland TA, Whitman IR, Win S, Sanchez JM, Olgin JE, Pletcher MJ, Santhosh L, et al. Prospective arrhythmia surveillance after a COVID-19 diagnosis. Open Heart. 2022;9(1):e001758.
doi pubmed pmc - Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054-1062.
doi pubmed pmc - Szarpak L, Mierzejewska M, Jurek J, Kochanowska A, Gasecka A, Truszewski Z, Pruc M, et al. Effect of coronary artery disease on COVID-19-prognosis and risk assessment: a systematic review and meta-analysis. Biology (Basel). 2022;11(2):221.
doi pubmed pmc - Nai Fovino L, Cademartiri F, Tarantini G. Subclinical coronary artery disease in COVID-19 patients. Eur Heart J Cardiovasc Imaging. 2020;21(9):1055-1056.
doi pubmed pmc - Hendren NS, Drazner MH, Bozkurt B, Cooper LT, Jr. Description and proposed management of the acute COVID-19 cardiovascular syndrome. Circulation. 2020;141(23):1903-1914.
doi pubmed pmc - Sanyaolu A, Okorie C, Marinkovic A, Patidar R, Younis K, Desai P, Hosein Z, et al. Comorbidity and its impact on patients with COVID-19. SN Compr Clin Med. 2020;2(8):1069-1076.
doi pubmed pmc - Guzik TJ, Mohiddin SA, Dimarco A, Patel V, Savvatis K, Marelli-Berg FM, Madhur MS, et al. COVID-19 and the cardiovascular system: implications for risk assessment, diagnosis, and treatment options. Cardiovasc Res. 2020;116(10):1666-1687.
doi pubmed pmc - Mousseaux E, Fayol A, Danchin N, Soulat G, Charpentier E, Livrozet M, Carves JB, et al. Association between coronary artery calcifications and 6-month mortality in hospitalized patients with COVID-19. Diagn Interv Imaging. 2021;102(12):717-725.
doi pubmed pmc - Nagele MP, Haubner B, Tanner FC, Ruschitzka F, Flammer AJ. Endothelial dysfunction in COVID-19: Current findings and therapeutic implications. Atherosclerosis. 2020;314:58-62.
doi pubmed pmc - Unudurthi SD, Luthra P, Bose RJC, McCarthy JR, Kontaridis MI. Cardiac inflammation in COVID-19: Lessons from heart failure. Life Sci. 2020;260:118482.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.